
Abstract
In this case, it is described the importance of ultrasound in children with sliding ovaries in inguinal hernias. If the child has no symptoms, an emergency ultrasound could suggest the manner of the operation, scheduled or emergency.
Introduction
Inguinal hernias are the commonest pathologies seen in pediatric surgery. Although in infants are operated as soon as possible for the fear of incarceration, it is referred that there is no urgent in cases of sliding ovaries in inguinal female hernias.1,2 Herein, it is described a case of a sliding ovary in an inguinal hernia and the role of ultrasound (US) that revealed the emergency operation.
Case report
A 6-month-old female presented with her parents at the emergency department of our hospital because of left inguinal painless swelling which appeared 2 days ago. The infant was otherwise healthy without any significant past medical history. Her parents reported also that they did not notice anything different in her reactions because like all infants she cried from time to time for no particular reason. When examined, a firm mass was palpated in the left groin. The hematological examination revealed only elevated white blood cell (WBC) (12,5 103 cells/mcL. Normal limits: 4,5-11 103 cells/mcL) and all the other markers within normal limits. The child was calm, eating well, and cried only when a manual reduction was tried. Τhe effort of the manual reduction was very gentle to avoid any injury and lasted a few seconds. (The child as soon as the doctor tried to touch her mass in her groin she reacted strongly and made the doctor to stop immediately.). The first evaluation was of an irreducible inguinal hernia.
After the failure of reduction, the child became calm again in her mother’s hug. With the possible clinical diagnosis of a sliding ovary in the inguinal sac (due to the child’s lack of irritability when a stranger was not near her), a US was followed. US exam revealed a well-circumscribed structure with peripheral, mostly, situated microcysts. Findings consistent with an ovary (with follicles) sitting on the anterior abdominal wall in the inguinal canal. The ovary was also enlarged and heterogeneous in appearance with somewhat hyperechoic areas, findings indicating an edematous process (Figure 1). Furthermore, on US and Color Doppler Imaging (CDI) exam, whirlpool-like appearance of vascular structures depicted. The vascular supply was not sufficient in CDI exam (Figure 2).
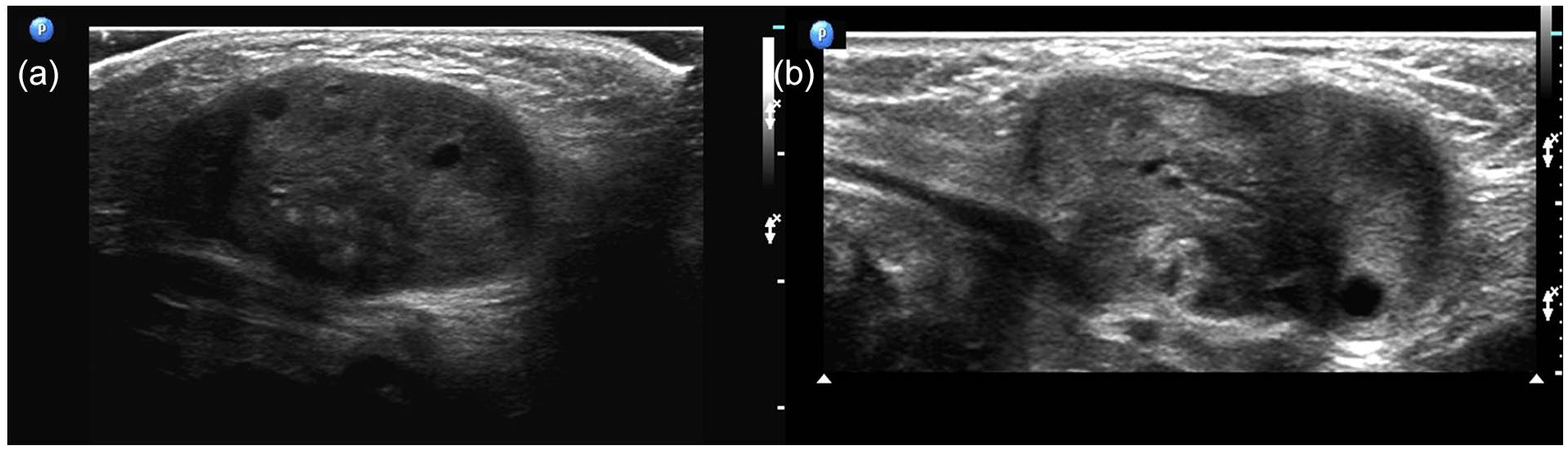
US exam, axial (a) and parasagittal (b) views, revealed a well-circumscribed structure with peripheral, mostly, situated microcysts (ovary with follicles) sitting superficially on the anterior abdominal wall in the inguinal canal. The ovary gives a sense of somewhat enlarged and heterogeneous depiction with somewhat hyperechoic areas in it. The findings are consisted with edematous process.

Axial (a) and CDI (b) views at the level of the inguinal canal revealed a not sufficient vascular supply and a whirlpool-like appearance (arrow) of vascular structures was noticed (open arrow: common femoral artery).
Final diagnosis
Torsion of the left ovary in an irreducible hernia was diagnosed.
Hospital course
US results suggested urgent surgical exploration of the left inguinal sac. In the operation, the sac had a small amount of serous fluid and the left ovary, which was deep blue with its vascular pedicle twisted twice (Figure 3). After detorsion of the pedicle and placement of the ovary in warm water for about 10 min, serious improvement of ovary perfusion was noticed and the placement of the ovary in the sac was decided (Figure 4). Then, the hernial sac was ligated. The child’s postoperative progress was uneventful, and she was discharged on the second postoperative day.
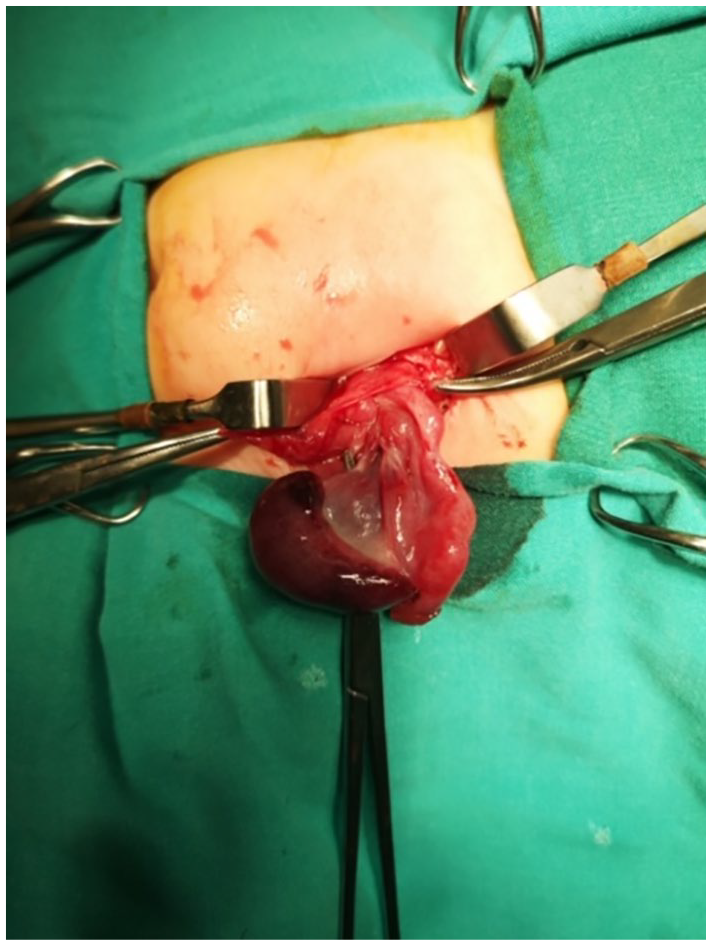
The ovary in deep blue color after the opening of the hernia sac.
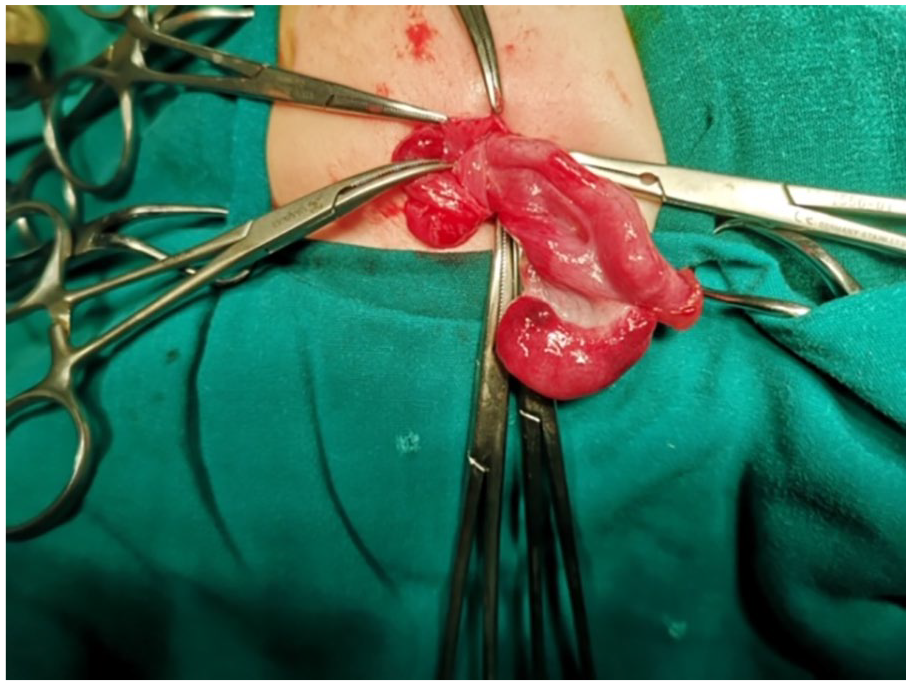
The ovary after its placement in warm water for 10 min.
Discussion
Inguinal hernias containing ovaries are not uncommon in infants since it is stated that 31% of inguinal hernias in girls younger than 2 years contain fallopian tubes and/or ovaries. 1 Although the ovaries come first among the structures that incarcerate in the inguinal hernia sac and in some studies it is reported that the rate of ovarian incarceration reaches 43%, the management of a girl with an irreducible ovary remains controversial in pediatric surgical centers.3,4 Most of the cases of irreducible hernias containing ovaries are scheduled according to the availability of space in a routine operating list because there is a consensus that irreducible sliding ovary does not pose a threat to its blood supply. However, there are several reports of twisted ovaries in hernial sacs. The incidence of non-reducible ovary in these reports was between 4% and 11% of which 2%–33% ovaries were twisted and infracted. 5 Due to these two different opinions, it is obvious that there is a controversy among surgeons about the time of operating a sliding hernia in an infant girl. In the case, it is described here it is referred that in infants where the clinical symptoms are absent, the US could inform whether the case is a true emergency, and the child must be operated as soon as possible and not scheduled.
The mechanism of torsion of an ovary in the inguinal sac probably is related to the fact that the ovarian vascular pedicle is narrow at the internal inguinal ring and the size of the ovary is greater than the pedicle predisposing to rotation. The mechanism seems to be similar to the “bell clapper” variant which is responsible for spontaneous testicular torsion. 6
The role of US exam in the diagnosis of inguinal hernias is important. In cases of herniation ovary, the US findings can give us information about the position and the dimensions of the ovary. The increase in the ovarian dimensions together with the heterogeneity and the presence of peripherally located multiple cysts are US findings raising the suspicion of ovarian torsion like in the case we describe here. 7 The presence of these findings alone is not sufficient to suggest ovarian torsion and to guide the surgeon for emergency operation. It is the tool of CDI which permits the examiner to evaluate the vascularity of the ovarian peduncle and suggests if the ovary is torsioned and ischemic or not. 6 In our case, the whirlpool-like appearance of the vascular structures and the insufficient vascular supply in the ovary suggested the torsion, and therefore, the urgent surgical exploration although in the clinical examination the child was calm and her history predisposed to irreducible hernia with ovary and not to incarceration or torsion. The valuable information of the US and the urgent operation led to the reperfusion and preservation of the infant’s ovary.
Conclusion
As a conclusion, the management of sliding ovaries in inguinal hernias should be treated in different ways. If the child has symptoms of acute pain or the mass in the groin is with limited mobility, the child should be treated with an emergency operation. If the girl has an irreducible hernia, but no symptoms could be scheduled if the ovary has sufficient blood supply. Otherwise, if there is a strong possibility of ovarian torsion, the child could be operated as an emergency case. This valuable information could be given by an emergency US which will suggest the manner of the operation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient’s parents for their anonymized information to be published in this article.