
Abstract
A 40-year-old female patient came to an outpatient sonography department for a follow-up scan of calculi in the right ureter that were originally found at another medical facility. The study was ordered to see if the stones caused hydronephrosis within the right kidney. Bilaterally, echogenic renal medullae were visualized, indicating a case of medullary sponge kidney and medullary nephrocalcinosis.
Introduction
Sonography has become an important diagnostic tool for imaging the kidneys. This modality gives high resolution visualization of abnormalities of the renal parenchyma including medullary sponge kidney (MSK). Medullary sponge kidney is a condition in which the collecting tubules in the renal pyramids are dilated or ectatic, and it may manifest focally or diffusely. 1 The etiology of MSK is not known; however, it has been found to occur in 12% of patients with renal stones, typically in patients in their fourth or fifth decade of life. 1 A patient is presented here who came in for a follow-up sonographic examination of her kidneys for renal calculi and was determined to have MSK. The purpose of this case study is to offer an example of MSK sonographic features as well as to discuss the need for recognition of this condition because of the potential complications of MSK.
Case Report
A 40-year-old female patient came to the outpatient sonography department for a follow-up scan of calculi in the right ureter that were originally found at another medical facility. The study was ordered to see if the stones had caused hydronephrosis within the right kidney. Evaluation of the kidneys and urinary bladder was performed using a Philips IU22 (Philips Ultrasound, Andover, Massachusetts, USA) with a 5.0 MHz curved array transducer. Gray-scale images with appropriate measurements were obtained from both kidneys in the longitudinal and transverse planes as well as color Doppler images. The urinary bladder was also imaged.
The right kidney measured 10.1 × 4.6 × 5.2 cm. The renal pyramids of the right kidney were uniformly highly echogenic within the right kidney (Figure 1). There were a few prominent small cystic structures that might have represented normal pyramids or necrotic papilla (Figure 2). The left kidney measured 10.6 × 5.7 × 4.8 cm. The parenchyma of the pyramids within the left kidney was the same as in the right side but with only one simple cyst measuring 9.4 mm in diameter (Figure 3). The urinary bladder was not distended and was otherwise unremarkable. No kidney stones were found during the examination. An incidental finding of cholelithiasis was seen with a stone measuring 7.5 mm in diameter. Based on the highly echogenic appearance of the medullary pyramids in both kidneys, medullary nephrocalcinosis with coexisting MSK was diagnosed. Papillary necrosis of a pyramid in the superior pole of the right kidney was also noted.

Longitudinal image of the mid right kidney showing strongly echogenic renal pyramids and a heterogeneous cystic structure located in the superior pole containing debris.
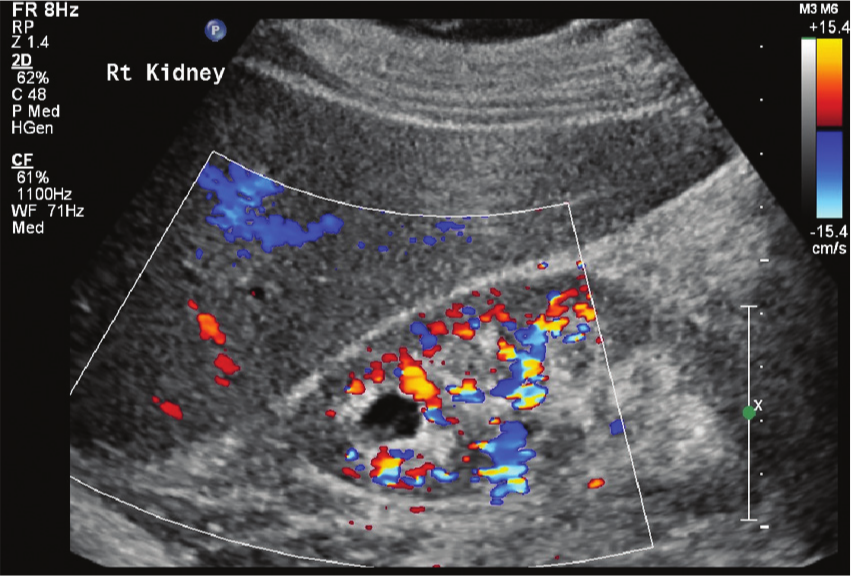
Longitudinal image of the mid right kidney with color Doppler confirming the lesion as an avascular cystic structure.

Longitudinal image of the mid left kidney similarly shows an echogenic medulla as well as a simple cyst in the inferior pole.
Discussion
Medullary sponge kidney is a focal or diffuse ectatic dilation of the medullary collecting tubules. 1 This causes stasis of urine and may eventually lead to calculi deposits. Although considered idiopathic, MSK appears as an anatomic defect with no metabolic process determinants. 2 As this condition does not always affect the entire kidney, MSK may have focal manifestations within the kidney. Whereas many patients are asymptomatic, some may present with renal stones, hematuria, or infection. Sonographically, MSK will appear as hyperechoic calyces when stones begin to form in the dilated collecting tubules.2,3 Smaller calcifications may not shadow; however, larger stones will produce shadowing. In the case presented, the sonographer found that the renal pyramids were highly echogenic, and this hyperechoic texture of the medulla was strongly suggestive of MSK with medullary nephrocalcinosis. Since this abnormal echo texture is a classic sign for MSK as well as an indication for a wide range of associated pathology, sonographers need to be able to recognize it in a sonogram.
Nephrocalcinosis is the formation of diffuse deposits of calcium throughout the kidneys. 2 This usually occurs within the renal medulla but occasionally it has been found in the cortex or within both the medulla and the cortex. 2 Causes of nephrocalcinosis include hyperthyroidism, ischemia, necrosis, renal tubular acidosis, renal failure, and hypercalcemia. 2 Medullary nephrocalcinosis usually occurs in the presence of other disorders including hyperparathyroidism (40%), renal tubular acidosis (20%), MSK, papillary necrosis, chronic pyelonephritis, hyperthyroidism, and sickle cell disease. 2 According to Glazer et al, increased echogenicity of the medullary pyramids can indicate the presence of renal disease as well as nephrocalcinosis. 4 When the kidneys do not function properly, they can atrophy, becoming small and echogenic.
Distinguishing between MSK and medullary nephrocalcinosis can be difficult sonographically, as many times these conditions coexist. Research has demonstrated that medullary nephrocalcinosis is not as easily diagnosed as cortical nephrocalcinosis because there are several differential diagnoses for echogenic renal pyramids, whereas increased echogenicity of the renal cortex is usually cortical nephrocalcinosis. 5 The primary difference between MSK and medullary nephrocalcinosis is that MSK is dilation of the collecting ducts of Bellini, whereas medullary nephrocalcinosis is calcium deposits or kidney stones within the dilated collecting ducts. The dilation of the collecting tubules and resulting stasis cause urine to become concentrated and acidic, which often leads to the calcification of the nephrons within the medulla. Calcification of the nephrons can then lead to the formation of kidney stones.
Papillary necrosis is the degeneration and sloughing off of the renal papillae as a result of vascular ischemia of the renal pyramids. 6 The sloughed parenchyma can calcify and obstruct the calyces or ureters, which leads to hydronephrosis. This condition typically affects patients bilaterally; however, it can be present as focal necrosis of one papilla or diffusely by affecting an entire kidney. 6 Clinical symptoms include flank or abdominal pain, hypertension, fever, dysuria, and hematuria. Sonographically, papillary necrosis may present as round or triangular cystic collections within the renal pyramids. Sloughed papillae look echogenic and may shadow if they calcify. Severe necrosis causes the replacement of medullary pyramids with multiple cystic structures filled with urine. The case presented demonstrates one irregular anechoic cystic area with debris noted in the superior pole of the right kidney, which is consistent with a focal papillary necrosis.
Conclusion
Sonographic evaluation of the kidneys is an important diagnostic tool used to identify pathology of the renal system, including MSK and medullary nephrocalcinosis. Medullary sponge kidney without calcifications may appear on sonography as a kidney with prominent hypoechoic calyces and thus may be difficult to diagnose. Conversely, MSK with nephrocalcinosis has a classic appearance of highly echogenic renal pyramids, which all sonographers need to be able to identify. This case study presented an example of a patient with nonshadowing echogenic medulla bilaterally. In addition, a simple cyst was found in the left kidney and evidence of papillary necrosis was found on the right kidney. Sonography can indeed distinguish between MSK with or without calcifications, and sonographers should be aware of the findings for this condition.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.