
Abstract
Ectopic pregnancy is a life-threatening condition if not detected early, prior to it rupturing. This case study presents a situation where an ectopic pregnancy is sonographically detected prerupture and treated with methotrexate. Based on serial sonograms, a salpingectomy was performed several weeks later when the pregnancy had not resolved. Sonographic findings indicative of an ectopic pregnancy are presented, along with the importance of correlating findings between serial sonograms and β–human chorionic gonadotropin serum levels.
An ectopic pregnancy is defined as a fertilized ovum implanting outside the uterus. 1 An ectopic pregnancy can occur in a variety of locations, such as the fallopian tubes, cervix, ovary, cornual region, and, in rare cases, the abdominal cavity. 2 The most common site of implantation is the fallopian tubes, where approximately 98% of ectopic pregnancies occur. Ectopic pregnancies are caused by impaired transport of an embryo to the uterus, often the result of chronic scarring of the fallopian tubes. 3 Risk factors for ectopic pregnancy include age older than 35 years, multiple sexual partners, tubal ligation, smoking, endometriosis, use of an intrauterine device (IUD), and fertility treatments. 2
The following case demonstrates the importance of correlating endovaginal sonography with serial β–human chorionic gonadotropin (β-hCG) levels to diagnose and treat an ectopic pregnancy in the appropriate manner. It is imperative to make this diagnosis early in the pregnancy to avoid rupture. A ruptured ectopic pregnancy is a serious medical emergency that can cause severe blood loss, shock, and maternal death.
Case Presentation
A 40-year-old woman presented to the emergency room complaining of abdominal cramping and spotting. The patient reported seeing a fertility specialist and had undergone in vitro fertilization (IVF). The patient had a positive pregnancy test and estimated a five-week, four-day gestation. The patient reported a gravida 1, para 0.
An endovaginal sonogram was performed using an Acuson Sequoia (Siemens Ultrasound, Malvern, Pennsylvania) with an EV-8C4 tightly curved endovaginal transducer operating at 9 MHz. The examination showed a hypoechoic, heterogeneous endometrium measuring 16 mm in the anterior-posterior diameter. There were also multiple uterine fibroids present, the largest measuring 2.2 by 1.9 cm. The right ovary contained a probable hemorrhagic cyst measuring 2.2 cm and a 2-cm simple cyst. The left ovary also contained a probable hemorrhagic cyst, measuring 1.9 cm. Within the left adnexa, between the uterus and left ovary, there appeared to be a gestational sac (Figure 1). The gestational sac contained a yolk sac and measured 6.9 mm, which corresponds to a gestational age of five weeks, three days (Figure 2). There was no evidence of an intrauterine pregnancy. After considering the β-hCG serum result of 3521 mIU/mL and the ultrasound findings, the diagnosis of ectopic pregnancy was made. Immediately following the sonogram, the patient was treated with a single intramuscular injection of methotrexate and asked to return for serial β-hCG tests.
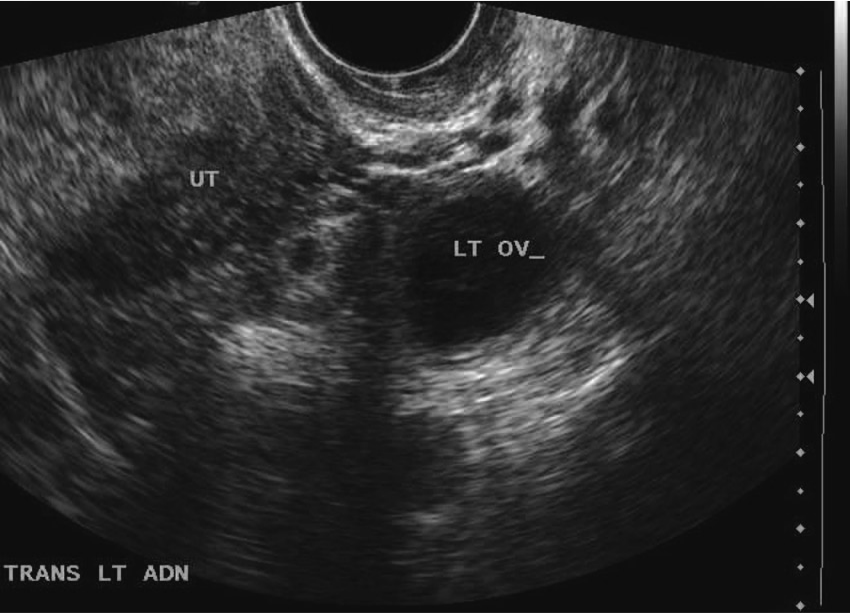
Initial sonogram showing a gestational sac located between the uterus and left ovary.
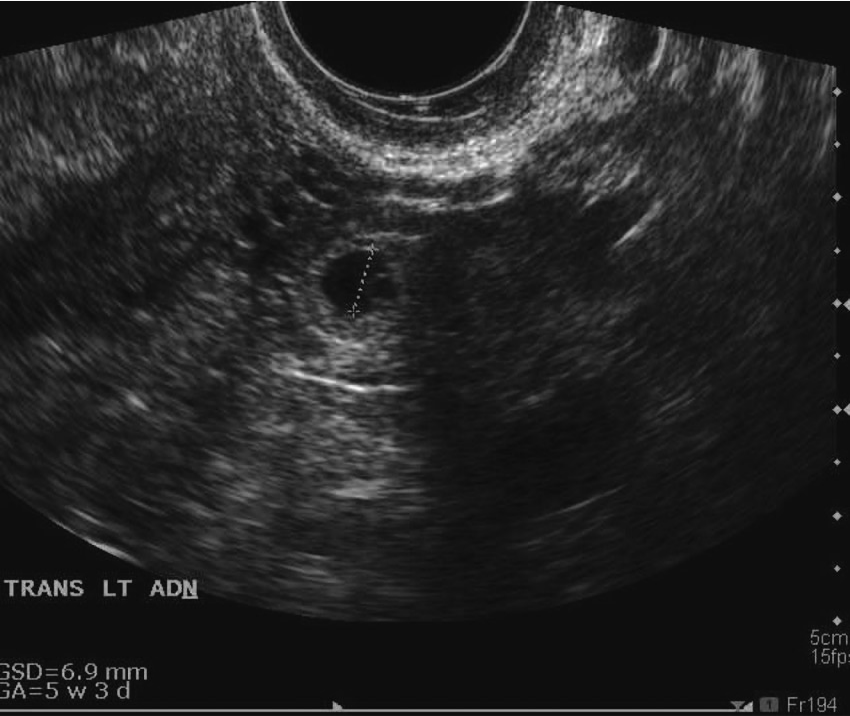
Initial sonogram showing a yolk sac within the gestational sac, measuring 6.9 mm in diameter, consistent with a gestational age of five weeks, three days. No embryo is seen.
Six days following the methotrexate injection, the β-hCG level rose to 6421 mIU/mL. On the 12th and 16th days, the β-hCG level fell to 4436 mIU/mL and 2100 mIU/mL, respectively. On the 19th day following the initial sonogram and methotrexate administration, a follow-up endovaginal sonogram was performed. This examination was performed on a Siemens Antares (Siemens Ultrasound), again using a 9-MHz endovaginal transducer. The sonogram showed a normal-appearing endometrium that measured 3 mm. The previously noted uterine fibroids appeared unchanged. Small, probable hemorrhagic cysts were again found within each ovary. Adjacent to the left ovary, the ectopic pregnancy was noted as before. The gestational sac contained an embryonic pole, in addition to the yolk sac previously seen. No heart tone was detected. The crown rump length of 3.2 mm suggested a gestational age of six weeks, zero days (Figure 3).

Follow-up sonogram showing a crown rump length measuring 3.2 mm, consistent with a gestational age of six weeks, zero days. No heart tone was detected.
On day 25 following the methotrexate injection, the β-hCG level fell further to 1285 mIU/mL (Figure 4). At that time, the attending obstetrician performed a left-sided salpingectomy based on a preoperative diagnosis of a persistent left ectopic pregnancy. A 7.2-cm segment of the left fallopian tube, including the fimbriated end at the left ovary, was removed and sent to pathology. The patient had a good surgical outcome, and no follow-up β-hCG serum tests or sonograms were ordered.
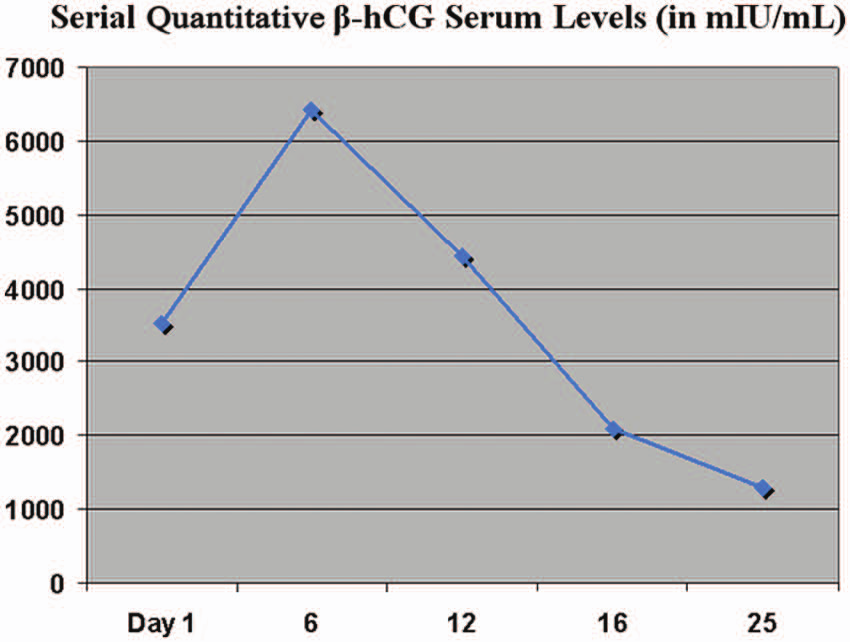
Graph of the patient’s serial β–human chorionic gonadotropin values following the initial sonogram and methotrexate injection.
Discussion
Ectopic pregnancies occur when a fertilized ovum implants outside the uterus. Any event that impairs the migration of the embryo into the uterus can result in an ectopic pregnancy. The most common site of implantation is the ampullary portion of the fallopian tube. 2 As the gestational sac enlarges, the potential for rupture increases, which can lead to hemorrhage, shock, and, in some cases, death. Ruptured ectopic pregnancies are the leading cause of maternal mortality in the first trimester, responsible for 70% to 75% of such deaths.4–6 This is why it is imperative to have an early diagnosis and to continue following the patient until the ectopic pregnancy has resolved.
Ectopic pregnancies occur in about 1% of all pregnancies. 7 The most significant risk factors for an ectopic pregnancy include women who have had a previous ectopic pregnancy, age older than 35 years, anything that may cause inflammation or infection of the fallopian tube (especially pelvic inflammatory disease), use of fertility drugs, women who have structural damages from prior surgery, and women who use an IUD. 2 In this particular case, the patient was 40 years old and had undergone IVF, both risk factors for an ectopic pregnancy.
Women who undergo IVF have a much higher rate of ectopic pregnancies than the general population. About 4% to 5% of IVF patients present with an ectopic pregnancy, approximately twice the rate for women who have not received IVF. One of the reasons ectopic pregnancies occur more often in the IVF population is because many of the risk factors for ectopic pregnancies overlap those for infertility, such as increased age and smoking. In addition, the use of superovulating agents in IVF alters tubal mobility. Another risk of IVF is retrograde migration. When retrograde migration occurs, embryos may enter and implant in the fallopian tubes after being transferred into the uterus. 8
In a normal pregnancy, β-hCG levels double approximately every 48 hours. Due to the size of the fallopian tube, growth of an ectopic pregnancy is restricted, and the β-hCG value will not double at the expected rate. Unfortunately, an early baseline β-hCG value was not available for this patient at the time of the initial sonogram. With the addition of endovaginal sonography, however, a diagnosis was readily made. Such early diagnoses are important in preventing an ectopic pregnancy from rupturing or to document an already ruptured ectopic pregnancy so that measures can be taken to prevent the patient from excessive blood loss and shock.
Several sonographic characteristics indicate the pregnancy is ectopic. The least specific of these is an empty uterus. An empty uterus can also indicate a missed abortion or a pregnancy too early to be visualized sonographically. It is also important to realize that the presence of an intrauterine pregnancy does not necessarily exclude an ectopic pregnancy. A heterotropic pregnancy occurs when a gestational sac in the uterus and an ectopic pregnancy coexist. The only way to make a definitive diagnosis of ectopic pregnancy is to find an echogenic ring outside the uterus, termed the decidual reaction. This can be in variable locations, and in this case it was located in the left adnexa. The decidual ring will have increased flow (trophoblastic flow) and an anechoic center (Figure 5).
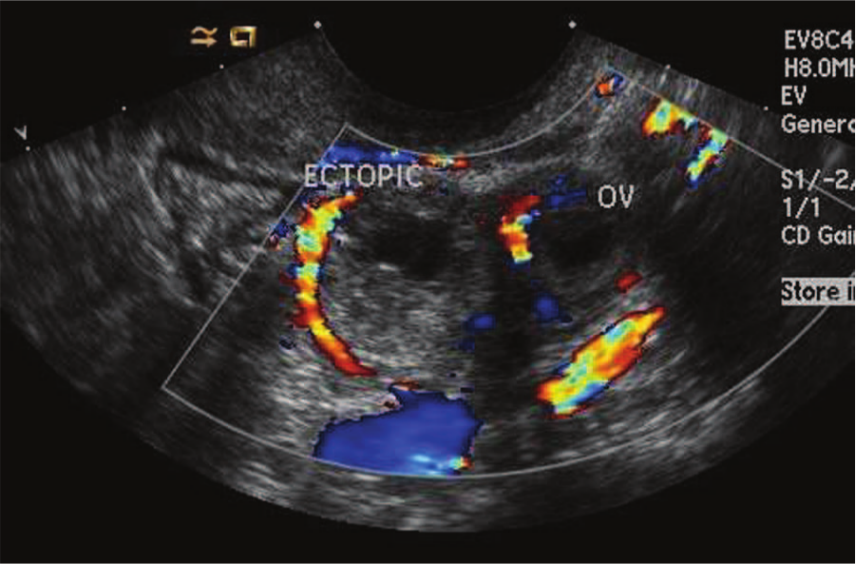
A color Doppler endovaginal image of the left ovary and ectopic pregnancy showing the decidual reaction and trophoblastic flow. Concomitant corpus luteum flow is seen adjacent to the gestational sac.
If an ectopic pregnancy is found before it has ruptured, conventional treatment is to administer methotrexate via intramuscular injection. When the β-hCG level is below 5000 mIU/mL, a single dose of methotrexate has been shown to have high success rates. There is a significant increase in failure rates when the β-hCG level is above 5000 mIU/mL. 9 The average time for an ectopic pregnancy to resolve with a single dose of methotrexate is 32 days. 7 However, recent research suggests physicians can predict whether an ectopic pregnancy will resolve after a single dose of methotrexate by following the trends of β-hCG levels for the first four days. If there is a rise in β-hCG levels within the first four days, there is only a 42% chance the ectopic pregnancy will resolve on its own, compared with an 88% chance with a decrease in β-hCG during that time interval. 9
Although the patient’s initial β-hCG was below 5000 mIU/mL, it subsequently rose after the methotrexate injection, indicating that this patient would likely require more aggressive action to resolve the ectopic pregnancy. In this case of unsuccessful conservative treatment, a salpingectomy was done, involving the removal of the involved segment of the fallopian tube to avoid an eventual ruptured ectopic pregnancy.
Prognosis following surgery and/or methotrexate injection is good, as long as the ectopic pregnancy has completely resolved. Ideally, methotrexate injection will be successful, as more invasive treatments may decrease fertility and increase the risk of developing another ectopic pregnancy. 2 Most patients are likely to desire noninvasive treatment to maintain fertility, especially in the case of IVF patients. The risk for an ectopic pregnancy continues to rise with each additional ectopic pregnancy; however, this risk declines if there is a subsequent intrauterine pregnancy.
Conclusion
Correlating serial β-hCG levels with sonographic findings is essential for the accurate diagnosis of an ectopic pregnancy and monitoring the patient to ensure the efficacy of treatment. As with this patient, methotrexate is not always a reliable solution. It is crucial to continue serial patient monitoring with β-hCG values and sonograms until the ectopic pregnancy has resolved.
Footnotes
Acknowledgements
The author thanks Heather Darr, RDMS, Cindy Beus, RDMS, Jana Crain-Dummermuth, RDMS, Sharlette Anderson, RDMS, RDCS, RVT, and Kelsy Merideth, RDMS, RDCS, RVT, for their assistance, support, and guidance while preparing this case study.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.