
Abstract
Objective
To investigate ultrasonographic characteristics and diagnostic approaches of unruptured tubal pregnancy (UTP).
Methods
One hundred forty-six cases of early tubal pregnancy, which were confirmed surgically, were analyzed.
Results
Among 146 cases of UTP, 130 were diagnosed by ultrasonography. Furthermore, 16 cases of UTP were missed by ultrasonography. A total of 130 patients had a mass detected by ultrasonography, among whom the mass and ipsilateral ovary were distinguishable in 102. The embryo sac type was found in 40.00% (52/130), while the heterogeneous mass type was found in 60.00% (78/130) of patients. The maximum length and diameter of the ectopic pregnancy mass ranged from 10 to 68 mm (mean size, 26.42 ± 11.39 mm). No blood flow was observed in or around the mass in 67.69% (88/130) of patients. Lateral tubal thickening of the mass was found in 47.69% (62/130) of patients. Endometrial thickness was ≤10 mm in 67.80% (99/146) of patients. The intima was mostly hyperechoic in 72.60% (106/146) of patients.
Conclusion
A paraovarian mass, thickened fallopian tube, uterine endometrium with a thickness of ≤10 mm, and high echo are important indicators of early UTP. Ultrasound examinations should focus on these indicators to help improve detection of early tubal pregnancy.
Keywords
Introduction
Ectopic pregnancy is a common gynecological emergency of the abdomen, and is the most common in tubal pregnancy, with a rate of 95% to 98%. To date, there is no gold standard non-invasive technique for diagnosing ectopic pregnancy. 1 If an ectopic pregnancy cannot be detected early and accurately, timely diagnosis and treatment are not provided. This can lead to rupture hemorrhage, shock, and even become life-threatening.2,3 Therefore, early unruptured tubal pregnancy (UTP) should be highly considered when a pregnancy test in blood or urine of the patient is positive and no pregnancy is found in utero. The objectives of this study were to investigate the ultrasonographic characteristics and diagnostic approaches of UTP. These have clinical significance for community hospitals if ectopic pregnancy can be detected earlier, especially under the limited conditions of a primary hospital.
Materials and methods
This study was conducted in accordance with the declaration of Helsinki. The study protocol was approved by the Ethics Committee of Chongming branch of Xinhua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine. Written informed consent was obtained from the participants.
Data collection
Patients who had a tubal pregnancy from January 2011 to December 2018 were included. The types of unruptured pregnancy were confirmed by an operation in our hospital. The duration of amenorrhea was 33 to 57 days in 134 patients and unknown in 12. These patients were all positive for urine human chorionic gonadotropin.
Instruments and methods
A GE Voluson 730 Expert system (General Electric Medical Systems, Milwaukee, WI, USA) and a GE Logic E9 color Doppler ultrasound diagnostic instrument (General Electric Medical Systems) were used coupled with a vaginal probe frequency of 5 to 9 MHz and an abdominal probe frequency of 2 to 5 MHz.
The bladder was properly filled during abdominal ultrasonography. When transvaginal ultrasonography was performed, the bladder was emptied and the lithotomy position was used. The vaginal probe was coated with a coupling agent, covered with a condom, and slowly placed into the posterior fornix of the vagina. Finally, the probe was inserted into the uterine cavity with or without a pregnancy sac or false pregnancy sac. The state of the bilateral accessory area was defined as no mass, the fallopian tube had no thickening, there was a relationship between the mass and fallopian tube, and the mass showed blood flow. A low echo was represented by a dark shade of gray. A medium echo was represented by a moderate shade of gray. A high echo was represented by a reflection coefficient >20%, the gray scale was bright, and there was no sound and shadow behind the echo.
All examinations were performed by physicians with more than 5 years of experience in gynecological ultrasound.
Gestational sac and pseudosac identification
In the endometrium, a real pregnant sac was determined if there was a “double ring sign” and the neck tube was not connected. In contrast, some anechoic areas located in the uterine cavity, which had no “double ring sign” and could be extended into the cervical canal, were considered to be a false pregnancy sac. 4
Scanning method of the ectopic pregnancy mass
When there was no clear pregnancy sound image in the uterine cavity, the direction of the probe was adjusted to scan the transverse plane, and the sound image was set to the maximum diameter line of the transverse plane of the uterine fundus. The fallopian tube and ovary were then observed from the corner of the uterus by slowly moving the probe to the side of the body and scanning the accessory areas outside this area in detail. Thickening of the fallopian tube and an attached mass were found. Individual differences existed, and thickening of the fallopian tube and attached mass could easily suffer from interference, such as bowel gas fecal mass when scanning and appropriately pressing the abdomen.
Results
The age of the patients ranged from 20 to 45 years old, with a mean (standard deviation) age of 33.42 ± 5.35 years. In the present study, among 146 cases of UTP, 130 were diagnosed by ultrasound and the diagnostic coincidence rate was 89.04% (130/146). The location of ectopic pregnancy was as follows. There were six (4.1%) cases of interstitial tubal pregnancy, 10 (6.84%) in the isthmus, 128 (87.67%) in the abdomen, and two (1.37%) in the fimbriae. Furthermore, there were 16 cases of missed diagnosis by ultrasonography and the missed diagnostic rate was 10.96% (16/146). Among these cases, 12 were located in the abdomen, two in the isthmus, and two in the interstitial area. Three cases were misdiagnosed by transabdominal ultrasonography. The maximum length and diameter of the ectopic pregnancy mass ranged from 10 to 68 mm, with a mean size of 26.42 ± 11.39 mm.
According to the echo characteristics of the ectopic pregnancy mass, blood flow was distributed around the mass and the relationship of the mass with the ipsilateral ovaries was examined (Table 1). Sixty-two (47.69%) patients had ipsilateral tubal thickening and 68 (52.30%) had no tubal thickening. We measured the thickness of the endometrium and the echo characteristics (Table 2). Most patients had an intimal thickness ≤10 mm and a high echo. The presence or absence of a three-line sign and a false pregnancy sac in utero is shown in Table 2.
Analysis of ultrasonographic features of the ectopic pregnancy mass.
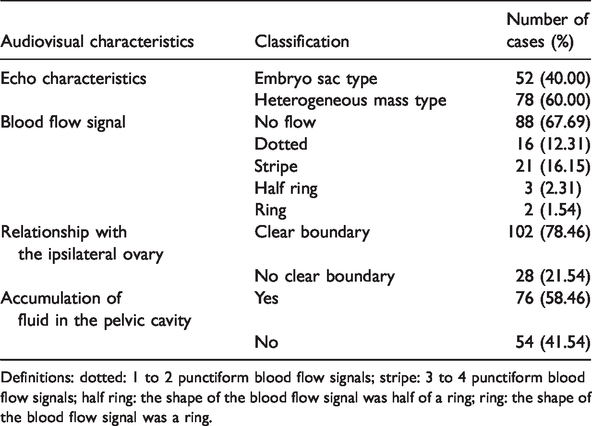
Definitions: dotted: 1 to 2 punctiform blood flow signals; stripe: 3 to 4 punctiform blood flow signals; half ring: the shape of the blood flow signal was half of a ring; ring: the shape of the blood flow signal was a ring.
Characteristics of ultrasonography of the uterine endometrium in tubal pregnancy.

Three-line sign refers to the lateral line of high echo formed between the endometrium and the myometrium and the center line of high echo formed by two layers of the endometrium.
Discussion
Ectopic pregnancy accounts for 2% of pregnancies.5,6 Among these pregnancies, tubal pregnancy is the one of most common types.7–9 The shape of the fallopian tube is tortuous and its position is changeable. Occurrence of a tubal pregnancy is often misdiagnosed because it is located deeply in the pelvic cavity. Rupture often occurs during tubal pregnancy in patients with internal bleeding, which can lead to a state of shock. When rupture is severe, it can lead to death of patients. Therefore, physicians need to perform a timely and accurate examination of ectopic pregnancy for diagnosis. Additionally, more attention should be applied to guidance of clinical treatment. 10 Transvaginal ultrasonography has good accuracy in the diagnosis of early pregnancy. 11 Therefore, this technique is considered as the first choice of a non-invasive examination. Importantly, medical workers can determine how to reduce misdiagnosis of ectopic tubal pregnancy and detect an unruptured ectopic pregnancy at an early stage.
In this study, we applied the ultrasonographic method to diagnose UTP. We investigated the clinical characteristics of ultrasonographic diagnosis for an ectopic tubal pregnancy. We found that tubal pregnancy occurred in the ampullary tubal area in 128 (87.67%) patients. A total of 48% of patients had ipsilateral tubal thickening. Ipsilateral fallopian tubes were often accompanied by varying degrees of changes in thickening. Ultrasound images showed long and low echoes extending from one side of the horn of the uterus to the outside, which finally continued to the detected mass echo. The reasons for tubal thickening were as follows. (1) During the ectopic tubal pregnancy, the fertilized egg was implanted in the tubal mucous folds to form a decidual membrane reaction, thereby resulting in tubal thickening. (2) The muscular layer of the fallopian tube was less thick and tough than the muscular wall of the uterus. When the fertilized egg was implanted into the fallopian tube, a blood vessel ruptured and bled at the implantation site because of the lack of the muscular layer protection of the fallopian tube. Blood perfusion then occurred in the fallopian tube and the fallopian tube became thickened. Therefore, close attention should be paid to enlargement of the fallopian tubes and early identification of a tubal mass in pregnancy.
The intima in most patients (72.60%) was hyperechoic. The critical value of the thickness of the intima was 10 mm. An intima with a thickness of ≤10 mm was found in 67.80% of patients, while an intima with a thickness of >10 mm was found in 26.03% of patients. Other authors have suggested that 9.8 mm could be used as the threshold of endometrial thickness to distinguish ectopic pregnancy from functional pregnancy. 12 Furthermore, the endometrium is significantly thinner in an ectopic pregnancy than in an intrauterine pregnancy. 13
Characteristic fallopian tube rings are often present during early tubal pregnancy. 14 This condition is due to thickening of the fallopian tube wall by edema, and formation of pregnancy tissue and blood clots in the tube cavity together. Fallopian tube rings are located in the fallopian tube area, with 10 to 30 mm in diameter and a ring wall of 5 to 10 mm and high echogenicity. The center of the ring is anechoic (regular or irregular pregnancy sac), and a few fallopian tube rings are observed with the embryo and cardiac beat, which is also known as “bagel sign”. 15 In an ectopic pregnancy mass, various yolk sacs and primitive heartbeats of the embryo are present, 16 allowing it to be easily diagnosed. However, identifying part of the ectopic pregnancy sac and the type of thick-walled pregnant corpus luteum is still difficult. According to observation of distribution of blood flow in color Doppler flow imaging, the findings of an ectopic pregnancy sac with no surrounding blood flow signals, a blood flow signal of the mass that is semi-circular, and a visible pregnant corpus luteum around the ring or half-ring rich blood flow signal are relatively rare. 17
In the present study, 16 cases of ectopic pregnancy mass were not detected by ultrasound, with a missed diagnostic rate of 10.96% (16/146). Among these cases, 12 cases were located in the ampulla, two were in the isthmus, and two were in the interstitium. Furthermore, among these patients, the operative time and ultrasonic examination time of five patients were longer than 4 days. Regardless of whether the follow-up time was too long, further analysis is required with a larger sample size. Cystic masses were observed in the ipsilateral adnexal area in two cases of ipsilateral ectopic pregnancy, in which the ectopic masses may have been obstructed and misdiagnosed. During the process of the examination, the scope of scanning should be expanded as far as possible to reduce a missed diagnosis. Three cases were misdiagnosed by transabdominal ultrasonography, which may have been due to interference by peritoneal gas and the patient’s obesity during transabdominal ultrasonography, or due to the ectopic pregnancy mass, which was small and could not be detected during transabdominal ultrasonography. 18 If ectopic pregnancy is suspected in the clinic, transvaginal ultrasonography should be performed.
There are some limitations to our study, such as the lack of grouping of patients and statistical analysis. Therefore, more prospective studies are required to confirm our findings.
Conclusion
A paraovarian mass, thickened fallopian tube, uterine endometrium with a thickness of ≤10 mm, and high echo may be important indicators of early UTP. The validity of our results need to be further confirmed.