
Abstract
This case report illustrates the sequential imaging of pregnancy beginning as an angular pregnancy, and eventually descending to a centric location within the uterine cavity. This case also describes the potential benefit of three-dimensional sonography in the management of a pregnancy, initially recognized as an angular pregnancy.
With the increased use of three-dimensional transvaginal sonography (3DTVS), a more precise visualization of an ectopic pregnancy (EP) has become possible, causing an evolution of our resultant terminology.1–3 An angular pregnancy (AP) is defined as a gestation that is implanted within a lateral angle of the endometrial lining of the uterus, medial to the uterotubal junction (i.e., cornual aspect of the uterine lumen), and can have the risk of uterine rupture, with potentially catastrophic consequences. With the increased resolution afforded by 3DTVS, the particular site of the gestational implantation can be more precise, determining whether it is an interstitial ectopic pregnancy (IEP) or an AP. This case report sequentially illustrates the apparent migration of an AP to a more centric position within the uterine intraluminal space, as opposed to migration to an interstitial ectopic location, where uterotubal rupture can alternatively occur.4,5
Case Report
A 30-year-old gravida 1, para 0 woman was referred to a gynecologic specialist for possible surgical management of suspected interstitial pregnancy. She had a history of infertility and her current pregnancy was conceived with in vitro fertilization (IVF), after three prior failed intrauterine insemination cycles. An initial sonographic examination showed a possible interstitial pregnancy, and a follow-up sonogram revealed borderline findings.
A 3DTVS was then performed at 6 weeks’ gestational age, revealing a gestational sac in an eccentric location within the right horn of a minimal arcuate uterus, which was most consistent with an AP (Figure 1). As endometrium was seen lateral to the gestation, she was deemed appropriate for expectant management with close sonographic surveillance. Repeat 3DTVS 1 week later (Figure 2) showed further evidence of an AP with a broad connection between the gestational sac and endometrial cavity measuring 18.3 mm. The distance from the gestational sac to the uterine serosa had progressed to 7.7 mm, suggesting migration of the pregnancy into the more medial location in the uterine cavity.
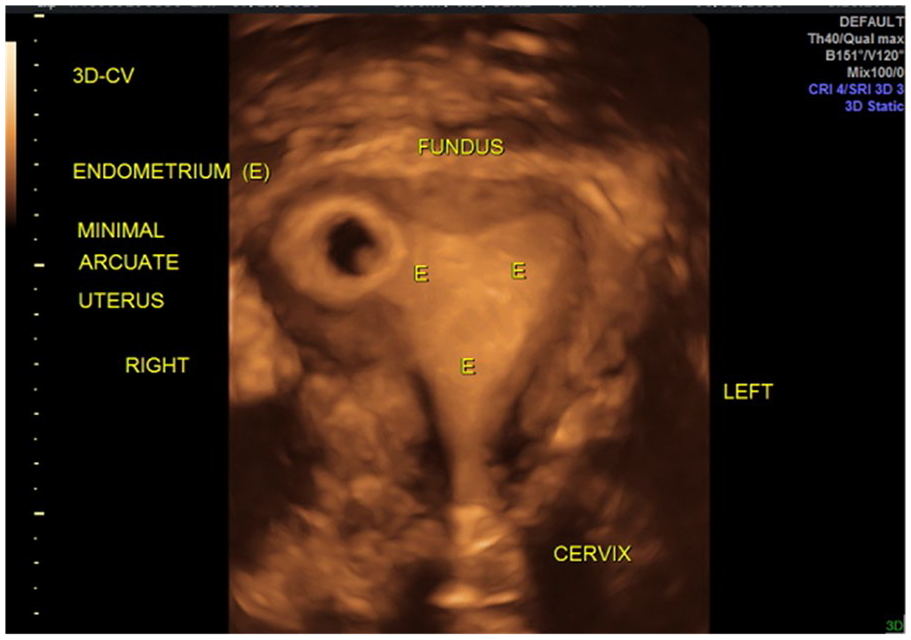
Rendered 3D sonogram revealing an eccentric positioned gestational sac in the right lateral corner of the endometrial cavity. Myometrium can be seen surrounding the lateral border of the gestational sac.
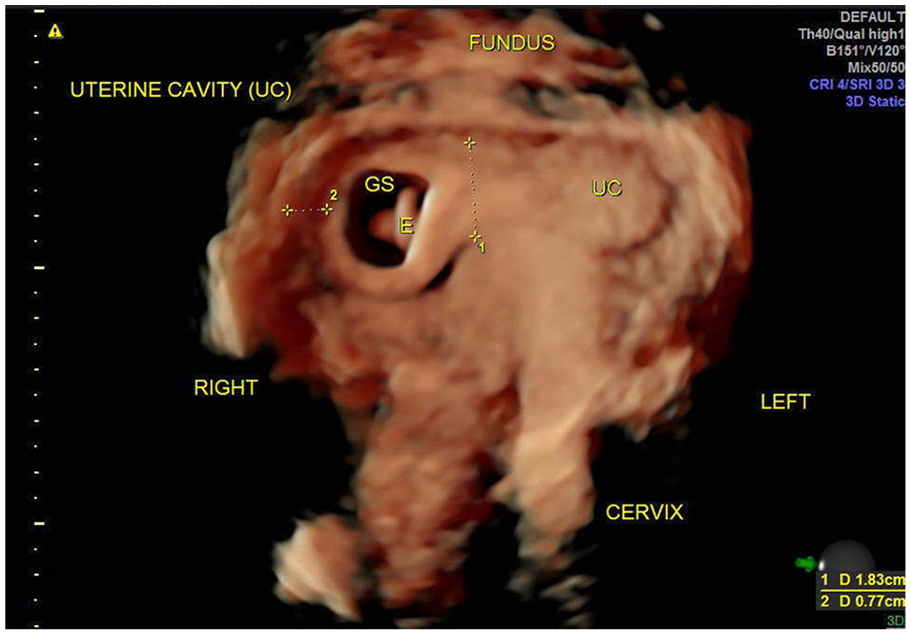
Rendered 3D sonographic image distinctly within the uterine lumen, seen more medially positioned than the previous image 1 week earlier.
A repeat 3DTVS 2 weeks later at 9 weeks’ gestational age revealed a live intrauterine pregnancy at the center of the uterine cavity (Figure 3). The distance from the gestational sac to the right uterine serosa was now 13 mm. The patient resumed her prenatal care at the outside institution, eventually resulting in a live birth.
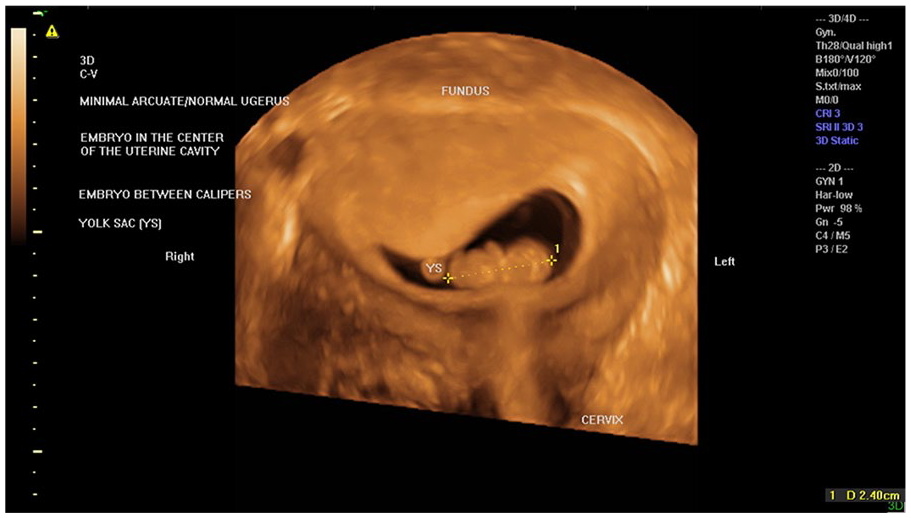
Rendered 3D sonographic image of the same gestation as seen 3 weeks previously, now in a more centric location within the uterine cavity.
Discussion
With the availability of 3D sonography, it is possible to be more specific as to a gestational implantation site, such that it is possible to distinguish between an IEP and an AP, each with different clinical consequences. Three-dimensional sonography allows for more specificity regarding the implantation site, and Baltarowich has suggested newer terminology relating to cornual pregnancies in general. 6 An AP should specifically refer to an intrauterine pregnancy that is implanted in one of the lateral angles of the uterine cavity, medial to the uterotubal junction. In this case report, full-term delivery occurred, resulting from the gestational sac descending into a medial location within the uterine cavity.
Several complications of AP have been previously described, as AP can result in spontaneous abortion, or uterine rupture. According to previous reports, AP has a higher rate of adverse outcomes. Yet, a case regarded as an AP may have been an IEP in prior reports.1,7 Therefore, the true incidence of obstetric complications in patients with AP remains unclear. A strategy of expectant management may be reasonable if continuous and careful monitoring of the mother and fetus is performed. Some references have reported expectant management of AP, with results similar to this case report.8,9
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.