
Abstract
Currently diagnostic modalities to evaluate lesions of the tongue are limited. Ultrasonography is a potential source of diagnostic information that can be utilized, if developed properly, to evaluate these lesions. This study investigates prospective windows sonography use to examine the tongue externally, lessening invasive measures currently used to diagnose and treat pathology. Based on results of this study, five of eight windows and methods tested were shown to have potential for evaluating the tongue externally. These were shown to be reproducible, acceptable windows for sonographers, providing a prospective means for sonographic evaluation of the tongue with hopes of developing a standardized protocol.
Oral cancer is considered to be highly aggressive among cancers and can be difficult to diagnose. Oral cavity cancers are broadly defined as areas affecting the tongue, salivary glands, lip, mouth floor, gingivae, palate, and buccal area. It has been estimated that approximately 3% to 5% of all cancers in the United States involve the oral and pharyngeal cavity, of which there are 30 100 new cases annually and 7800 are fatal. 1 Ninety percent of oral malignancies affect those in the fourth to sixth decade of life. More recently there has been an increase in incidence in men and women at much earlier ages, as young as in their 20s and 30s, without the common predisposing factors of chronic tobacco use (including smokeless tobacco) and alcohol consumption but possibly related to human papillomavirus (HPV) infection. 2 Furthermore, there is a low five-year survival rate for these patients at 58% overall. Oral cancers have a high chance of metastasis, lymph node involvement, reoccurrence, and development of new primary and secondary cancers. In patients that survive, there is up to a 30% chance of development of a new primary cancer involving the head or neck. 1 The trend is not progressing positively either; in the past 30 years it has remained relatively unchanged. Although the incidence of oral malignancy is relatively low among types, it is obvious that they are highly malignant and aggressive. Contributing to the low survival rates, limited diagnostic options typically mean that oral cancers are commonly diagnosed in advanced stages. This report focuses on the results of a pilot research study investigating potential external and universally accessible windows for viewing the tongue using ultrasound technology to determine the diagnostic potential of sonography.
Materials and Methods
Data analyzed in this study were collected from a sample of 15 volunteers. The institution’s Health Sciences Institutional Review Board approved the overall study after careful consideration. Each participant was given ample opportunity prior to the start of the study to consider his or her involvement. Once the volunteer decided to participate in this investigation, written informed consent was obtained according to standardized human research protocols. Personal health information was protected as no identifying markers were used in the collection or evaluation of data. No images obtained from the volunteers were saved on machines, but were printed for immediate evaluation and analysis for results. Universal precautions were observed for all testing, and since some parts of the study involved probe contact with saliva, the probe was cleaned and disinfected prior to each test according to the manufacturer’s specifications.
Each participant was scanned on the same type of machine: GE Logiq7 (GE Healthcare, Milwaukee, Wisconsin). Since the tongue was considered a superficial structure through the windows being tested in this study, a 14 MHz broadband linear matrix array transducer was used. All sonographic examinations were conducted using the musculoskeletal and upper extremity arterial (UEA) presets on the machine. The high frequency was chosen for this study for enhanced resolution of the tongue structures since deep penetration was not required. Quality control of each gray-scale image produced in this study was crucial for sufficient determination of visualization of the tongue. Overall gain, time gain compensation, focal points, and depth were carefully adjusted prior to each image obtained to help achieve the highest quality images possible.
Throughout the study, eight possible acoustic access windows to visualize the tongue were assessed. For seven of the eight windows evaluated, the volunteer was placed in an erect position sitting at the edge of the examination table; the exception to this was for the approach testing the neck in which the volunteer was asked to slightly direct the head superiorly looking up toward the ceiling. Each transducer probe placement was chosen to maximize the likelihood of reproducibility and to test accessibility of viewing the tongue. In certain windows chosen in this study, the volunteer was asked to hold water in the mouth to give the sound waves a medium in which to propagate.
The first two windows analyzed in this study involved the tongue sticking out of the volunteer’s mouth as far as possible. For the first of the two, the transducer probe was placed directly on the tongue surface to test if a quality image of tongue parenchyma could be obtained (Figure 1) and if the body’s natural saliva could act as a coupling medium for the sound waves to travel. The second approach used a probe cover placed over the transducer with sterile gel acting as a coupling medium (Figure 2); no gel was placed on the outside of the probe cover for this approach. For both of the windows involving direct probe placement on the tongue, the transducer was placed in a longitudinal plane mid-tongue with the marker on the probe directed toward the patient’s throat.
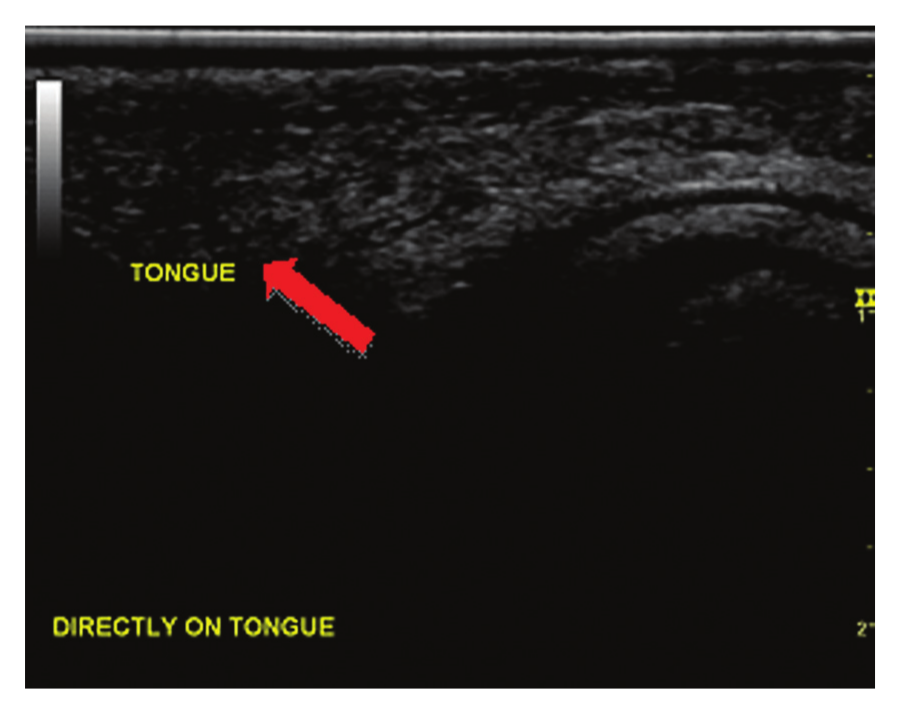
Transducer placed directly onto surface of tongue, using saliva as a couplant. The arrow indicates tongue parenchyma visualized.
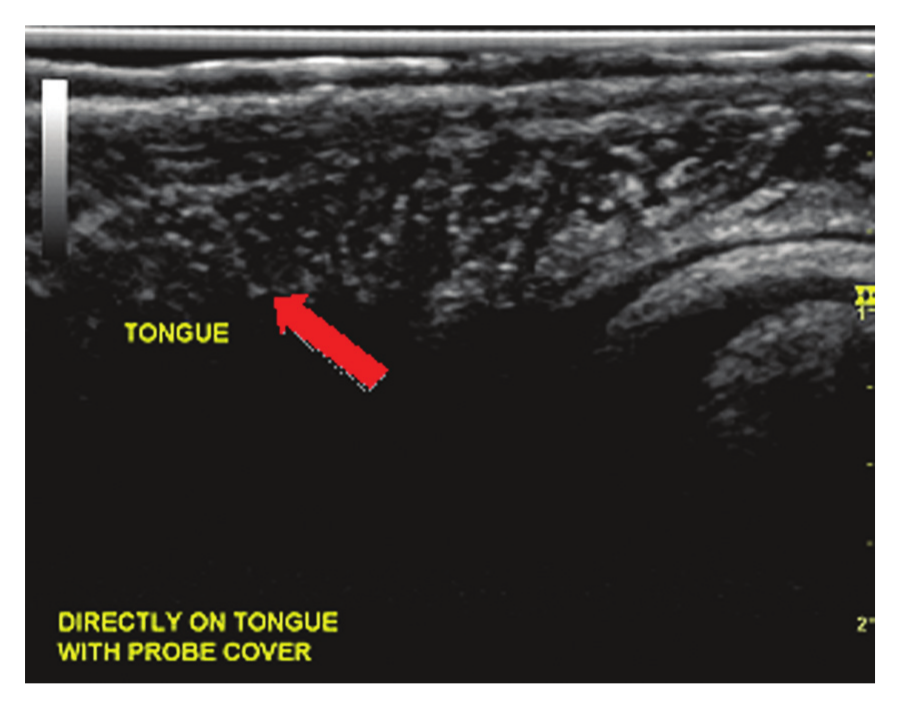
Transducer placed directly onto surface of tongue with probe cover containing ultrasound gel as a couplant. The arrow indicates tongue parenchyma visualized.
The third and fourth approaches placed the transducer on the outer surface of the buccal area with coupling gel placed between the transducer and the outer surface of the cheek. The transducer was placed on the volunteer’s mid-left cheek in a transverse plane. For consistency of orientation, the marker on the probe was pointed toward the participant’s right side. The volunteer was asked to separate the teeth while keeping the lips closed. For the third image, the volunteer’s mouth was empty so the medium for the sound waves between the inner cheek surface and tongue might contain air (Figure 3). The fourth method asked the volunteer to take a mouth full of water such that the water acted as a medium between the inner surface of the cheek and tongue for potential visualization (Figure 4).
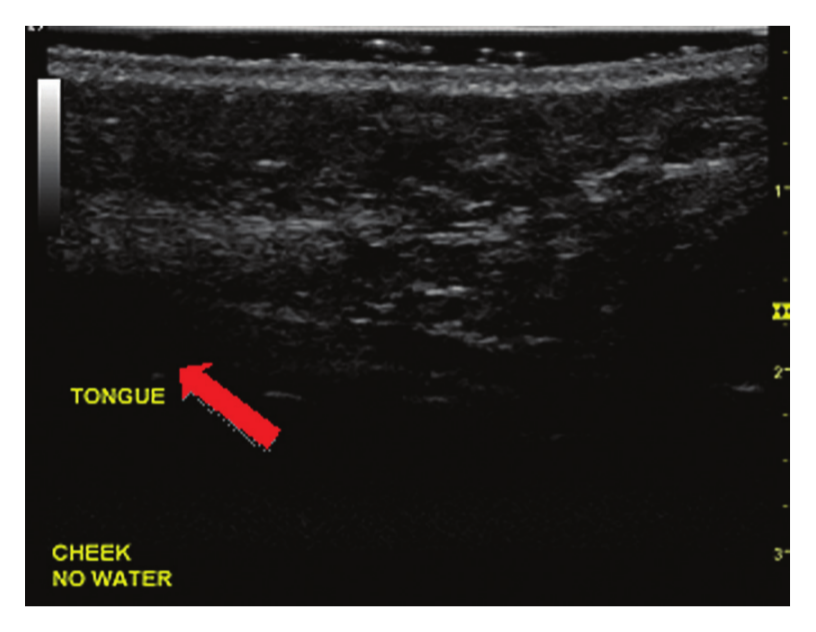
Transducer placed on the cheek with no water held in mouth. The arrow indicates where the tongue parenchyma should be visualized.
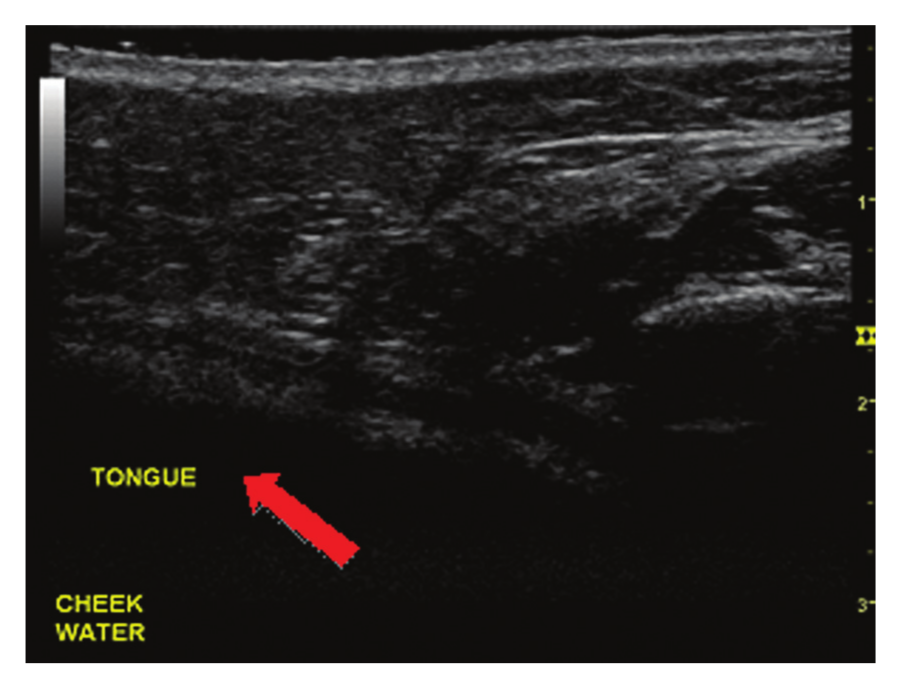
Transducer placed on the cheek with water held in mouth. The arrow indicates where the tongue parenchyma should be visualized.
The fifth and sixth approaches placed the transducer below the jaw line in the medial submental area. The transducer was held in a transverse plane to the middle portion of the tongue (true coronal plane to the volunteer) with the notch pointed toward the volunteer’s right. For the first submental approach, no water was held in the mouth (Figure 5). The second submental approach required the volunteer to again hold a mouth full of water for image acquisition (Figure 6).
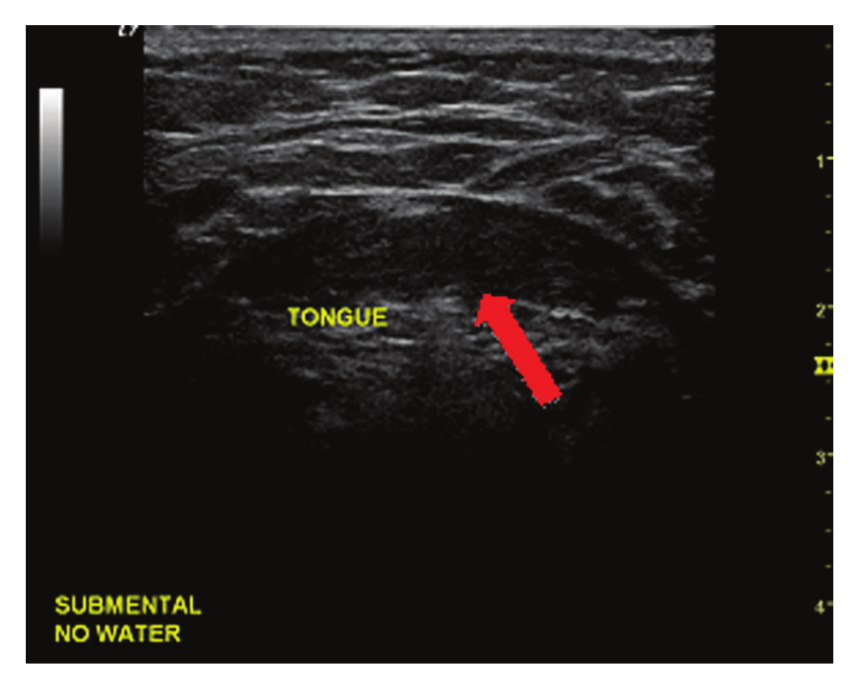
Transducer placed submentally with no water held in mouth. The arrow indicates tongue parenchyma visualized.
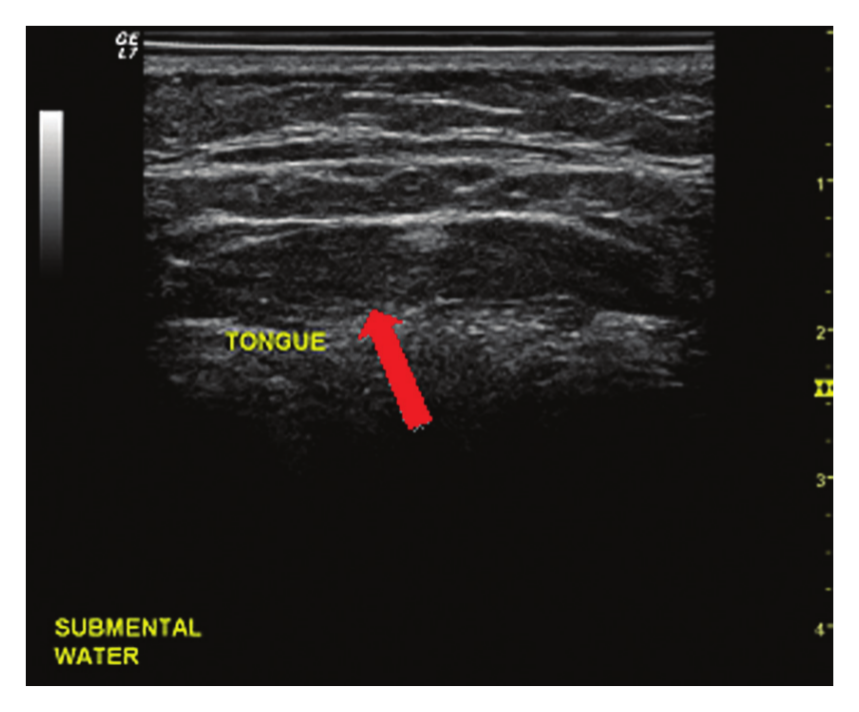
Transducer placed submentally with water held in the mouth. The arrow indicates tongue parenchyma visualized.
The transducer was placed at the junction of the submental area and neck, just to the left of the trachea, for the final two approaches. Longitudinal scan planes for these methods were used to test best visualization of the tongue base with the transducer oriented toward the participant’s head. The participant was asked to slightly raise the head superiorly. The seventh approach was tested with no water held in the mouth (Figure 7) while the final method was tested with a mouthful of water in the same plane (Figure 8).
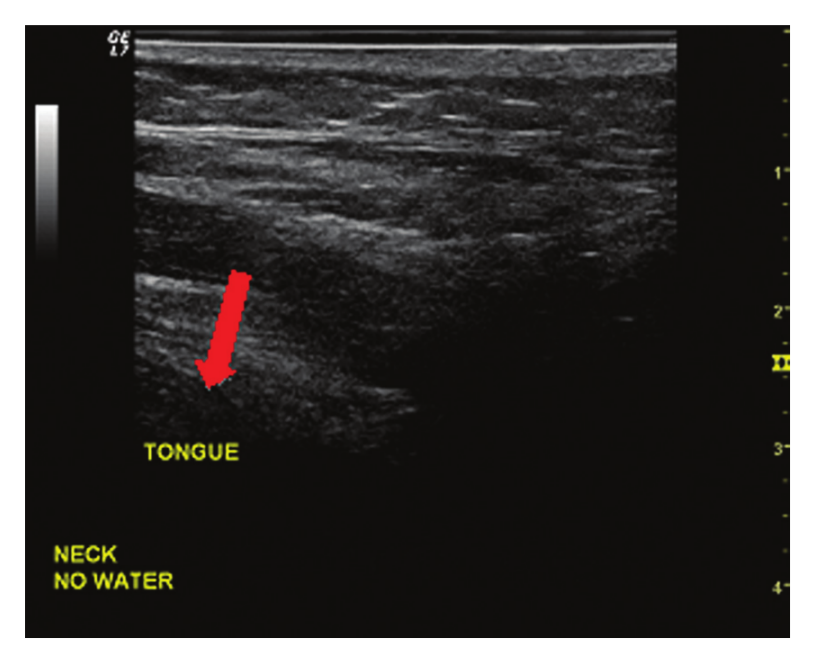
Transducer placed on the neck with no water held in the mouth. The arrow indicates tongue parenchyma visualized.
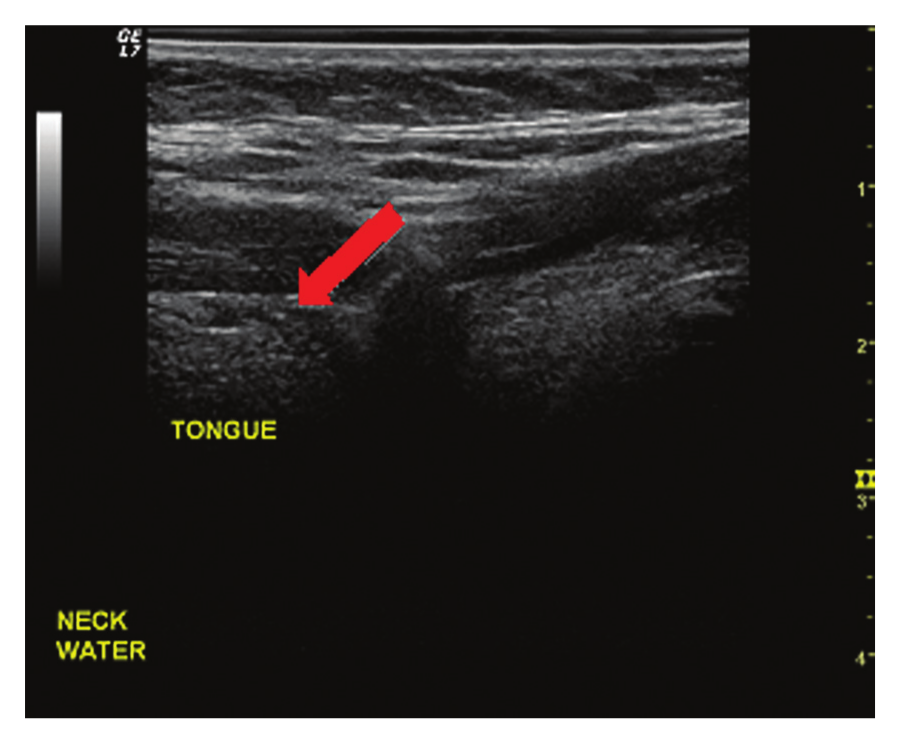
Transducer placed on the neck with water held in mouth. The arrow indicates tongue parenchyma visualized.
It was the goal of this study to estimate p, the true population proportion of ultrasound images of acceptable quality. In computing sample size requirements for the true proportion of acceptable-quality ultrasound images, the researcher assumed in this assessment that the level of significance (α) is .05 and that the true sample proportion of acceptable ultrasound images lies between .94 and .98. With a sample size of 15, the projected margin of error was between 6.7% and 11.2%, which was considered acceptable by the investigator for a pilot study of feasibility. For the eight acoustic windows tested, each category determined was individually analyzed by percentage. A combination of all the factors was averaged to give an overall mean for each potential window. It was determined by the researcher prior to conducting the study that any overall mean above 85% would be considered an acceptable window and method for visualization of the tongue suitable for potential future diagnostic evaluation.
Results
The five windows and methods determined by this study as acceptable included directly on the tongue, directly on the tongue with a probe cover, submental approach with water held in the mouth, on the neck without water, and on the neck with water held in the mouth (Table 1). The approach for the transducer placed directly on the tongue gave sufficient images of the tongue; however, placement directly on the tongue with the probe cover utilized subjectively gave far better quality and visualization of more detail of the tongue. Even though the first approach was deemed acceptable, it would not be preferred to the probe cover on the basis of image quality and lack of protection against infectious control in the clinical settings.
Individual Analysis of Potential Windows and Methods to Visualize the Tongue
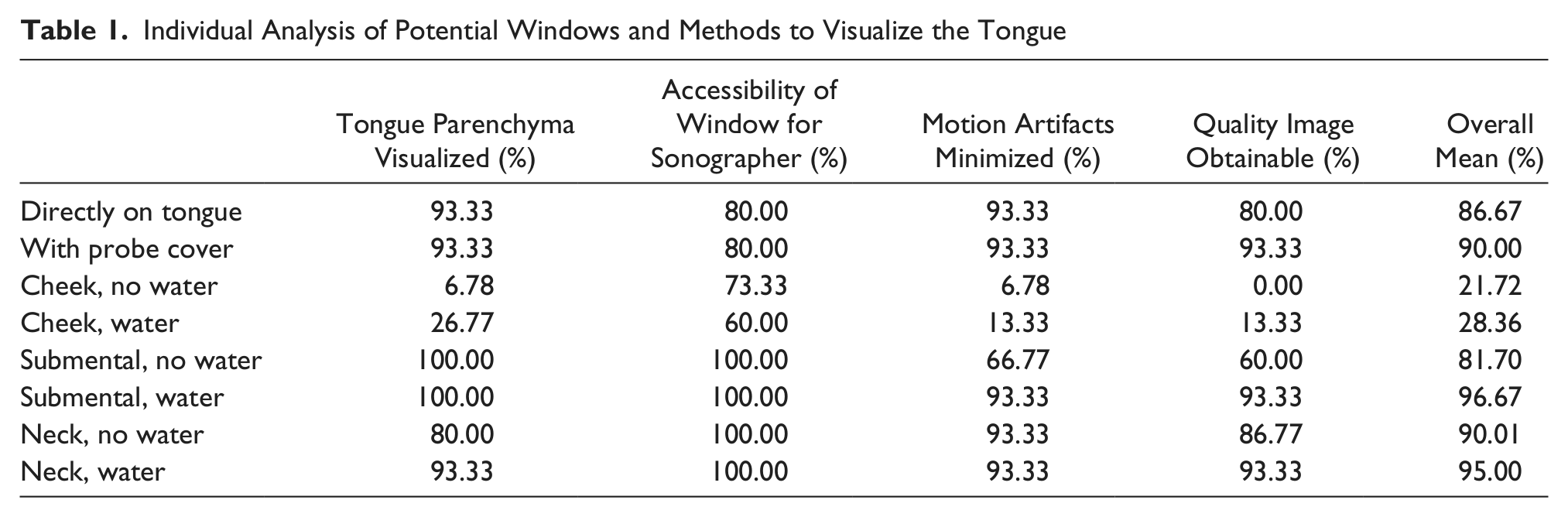
Visualization of the tongue through the buccal area, without water, was determined to be an unacceptable approach. Using this window without water, only one volunteer’s tongue was visualized, image quality was significantly degraded, and the positioning of the volunteer’s mouth was awkward for some. Water held in the mouth did resolve these issues to some extent, with four tongues identified; however, the improvement in tongue visualization and image quality was not increased enough to be considered an acceptable method to use sonography as a diagnostic tool.
The submental approach without water held in the mouth was also found to be an unacceptable window for tongue visualization. Although every tongue was visualized on the volunteers with this approach and method, the motion of the tongue without water made satisfactory images difficult to achieve, and quality control of the images produced was difficult to maintain. The submental approach with water held in the mouth of the volunteer proved to be the most effective method tested in this study to visualize the tongue as it had excellent accessibility to tongue parenchyma externally and the water stabilized the tongue significantly, reducing motion artifacts and enhancing the quality of images produced. The water also acted as a coupling medium in which the sound waves could better propagate, reducing motion artifacts by 26.56% and increasing image quality by 33.33%.
To a lesser extent, this was also noted when the transducer was placed on the neck. When water was held in the mouth, it stabilized the tongue substantially compared to the respective approaches without water, and even brought the tongue “down” more into the image resulting in more tongue parenchyma identified. However, with the transducer on the neck, the water did not act as effectively as a coupling medium; nonetheless, the presence of water did increase the proportion of tongue parenchyma visualized by 13.33% and improved image quality by 6.56%.
Based on the calculated means, the best approach to visualize the tongue externally proved to be a submental approach with water held in the mouth, followed by the neck approach with water held in the mouth. Slightly inferior to these two approaches, but still quite acceptable, were the windows using the neck without water and probe placement directly on the tongue with a probe cover. Finally, probe placement directly on the tongue without a cover was considered acceptable by study definition, but would not be a preferred technique in clinical practice.
Discussion
This study focused on the area limited to the tongue, as it is the most common site of oral cancer. The most common type of cancer affecting the tongue is squamous cell carcinoma (SCC), accounting for an estimated 90% of malignant tongue pathology. 3 There are two main criteria to consider that must be evaluated when discussing tongue cancer: the thickness of the lesion and lymph node involvement. The thickness of the squamous cell carcinoma has been shown to correlate with the involvement of lymph nodes; as a rule, the thicker the cancer, the more likely there is lymph node involvement. 3 Also of note, SCC located near the base of the tongue correlates with later detection and lower survival rates compared to cancers on the oral portion of the tongue. 1 The base of the tongue is a more difficult site to evaluate than the oral portion, and new methods of diagnostic evaluation should be considered and researched to help reverse this trend.
As with any cancer, lymph node involvement is key in diagnosing and staging of the malignancy. Early diagnosis of stage I or II cancer is limited to a 4 cm lesion without diffuse spreading to adjacent parenchyma, cervical lymph nodes, or other organs. 1 Cancers that have spread to surrounding structures and lymph nodes would therefore be categorized as stage III or IV accordingly. It is possible for these localized tongue lesions to be identified prior to metastasis and lymph node involvement in early stages during regular dental or physical examinations using visualization and palpation. However, screening is not routinely done for tongue cancers and they can therefore progress unbeknownst to the patient. Too often by the time of recognition of the lesion, the prognosis has significantly worsened.
Sonographic techniques are not used currently as a standardized diagnostic tool for evaluation of this category of cancers. The literature suggests that the use of sonography as a diagnostic tool to evaluate tongue pathologies, particularly malignant lesions, is limited to only measuring lesion thickness and identification of a hypoechoic SCC lesion in comparison to surrounding tissue. 4 Additional applications of sonographic technology involving the tongue (as well as many other pathologies) involves fine needle aspirations (FNAs) and guided biopsies, although such utilization is widely variable in practice, and lymph node examination. 4 FNAs and biopsies have individual sets of risks that have the potential to further threaten the patient, and there is the additional possibility of FNAs and biopsy of benign lesions in patients with suspicious but nondefinitive pre-intervention findings. For suspected SCC of the tongue, there are more aggressive measures undertaken in diagnosis and treatment. The current accepted method of diagnosis involves varying degrees of glossectomy as well as neck dissections to remove possible metastatic lymph nodes, depending of the nature and severity of the lesion. 4 Removal of portions of the tongue, due to biopsy or glossectomy, and neck dissections can greatly impact the quality of life for the patient. For those patients who undergo any degree of glossectomy but ultimately are found to have benign disease, the procedure, although precautionary and justified, can negatively and needlessly affect their quality of life in terms of speech and mastication.
Sonography has been proven to be very good in soft tissue characterization throughout the body. Though not currently used in practice for oral examination, it has the potential to offer vital information that is not accessible via other methods, is comfortable for the patient, and does not involve harmful exposure to radiation. 6 This study identified five acceptable windows for the sonographic evaluation of the tongue, two of which appear to have particular promise. These are a submental approach with water held in the mouth, followed by the neck approach with water held in the mouth. The results indicated that the water not only acted as a medium for the ultrasound to propagate, it also acted as a medium for the volunteer to keep the tongue stabilized in the mouth and throat, which aided in better visualization and identification. Only slightly inferior to these two, and also clinically acceptable, would be direct probe placement on the tongue using a probe cover as an isolation barrier. One expected result based on initial observations was that the transducer placed directly on the tongue with a probe cover would be superior in quality to an approach on the neck; however, this was not supported by the data. If proper techniques could be standardized and applied to the soft tissue of the tongue, many patients could benefit from its advantages in aiding diagnosis of SCC and potentially lessen the chance of unnecessary FNAs, biopsy, or glossectomy. Further research on the characterization of SCC, including more detail on shape, echogenicity, perimeters, vascularity, and hemodynamics, could then be carried out to fully offer sonography’s attributes to patients as a viable diagnostic tool.
There are certainly some limitations to ultrasound as a technology that can hinder its use as a tool for diagnostic purposes in this application. These limitations include the large footprint of commercially available transducers, inability of patients to open their mouth sufficiently, and the gag reflex. 4 The current status of probes and examination techniques available for intraoral sonography are not sufficient for tissue characterization, but there is the potential for technology to miniaturize ultrasound probes. Intraoral sonography today is practiced even less than transcutaneous examination of the tongue, but the future is promising. 5 Inherent in the concept of the sonographic diagnosis of lesions of the tongue is the need to standardize the placement and orientation of the ultrasound probe. 5 When implemented, a standardized method of diagnostic visualization of the tongue could help decrease the need for or the extent of glossectomy, which in turn would dampen the negative impacts to quality of life.
This study represents the first attempt to create a standardized method of visualization to use sonography as a tool for the detection and diagnosis of lesions on the tongue. A fully developed protocol was not the intention of this study, but only to investigate potential external and universally accessible windows for viewing the tongue using ultrasound technology in the hopes of paving the groundwork for the future standardization of a protocol for diagnostic examinations. Although this study utilized a small sample size and is basic in design, the results and impacts of the information obtained can, with further research and development, potentially lead to invaluable methodology of tongue pathology evaluation.
Limitations to this study were not overlooked. A 14 MHz probe was chosen because it offered the highest frequency available at the time of the study. The musculoskeletal or UEA presettings were selected as generally available, typical superficial/small parts machine settings, though obviously such presettings can differ between machines and individual user preferences in any given clinical situation. Though a probe frequency of 14 MHz was sufficient in obtaining the images needed for the purpose of this study, a higher frequency should be tested in future studies to determine whether increased resolution of tissue features would be required for proper evaluation. The impact of variations in body habitus of the patient, particularly the neck, should also be considered for future study, as patients that have excessive fatty tissue or thicker musculature in the neck area would require lower frequency for penetration to tongue tissue with resultant loss of resolution and image quality. Finally, the only medium used in this study for the volunteer to hold in the mouth as a coupling agent and stabilizer was water. Other mediums, such as an oral stand-off pad, could be tested to determine any impact the type of medium would have on image quality and visualization of the tongue. Such a pad could be as simple as a small bag filled with coupling gel, which could be easily manipulated and moved throughout the oral cavity.
Application of the acoustic windows and methods investigated throughout this study could positively impact the care received by patients with squamous cell carcinoma and other pathologies of the tongue by lessening the complications and consequences of current diagnostic modalities and treatment plans. Sonographic identification and localization of lesions on the tongue via external routes prior to invasive procedures, whether near the oral portion or basal portion, could significantly alter the pathway of care. Once standardization and further investigation of this method is developed, earlier diagnosis of SCC should improve survival rates of these patients by detection of the lesion prior to metastatic spread and lymph node involvement. Additionally, sonography could be used in conjunction with other methods to better analyze the progression of pathology, develop treatment plans, and enhance ultrasound-guided procedures.
Conclusion
Based on the results of this study, external evaluation of the tongue using sonography would be noninvasive and easily repeatable, have reproducible results, and provide a relatively inexpensive diagnostic tool. Potential windows and methods were tested in this study that might serve as the steppingstones for developing a standard protocol for noninvasive evaluation of the tongue. Further research and technological developments are still needed to offer patients with pathologies of the tongue the full prospective advantages of ultrasound.
Footnotes
Acknowledgements
In memory of Rebekkah as she lost her battle with squamous cell carcinoma at the age of 31. She was my inspiration for this project. Everyday was a battle. Fly high. Sing loud. Early detection of this cancer was not available to her, however maybe in the future it can help others. The author would like to thank Civco for their support in providing the probe covers as materials for this research project. The author also sends appreciation to the institution’s Statistics Department and Diagnostic Medical Ultrasound staff for their assistance and analysis, revisions, and guidance.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.