
Abstract
Simulation training in sonography has been shown be an effective method of teaching and assessing user competency in image acquisition/interpretation and performance of procedures. Gallbladder simulation models that are currently commercially available are entire torso section phantoms, are generally expensive to obtain, and require maintenance. We have developed a sonographic gallbladder simulation model constructed using readily available and inexpensive materials. Models were created of normal gallbladder anatomy as well as various gallbladder pathologies such as cholelithiasis, biliary sludge, and thickening of the gallbladder wall. This model can be used to train users both to obtain and interpret sonographic images of the gallbladder.
Biliary tract disorders constitute a relatively common cause of presentation to the emergency department (ED). It is estimated that 20% of women and 8% of men have gallstones, resulting in approximately 500,000 operations annually. 1 Acute cholecystitis is the end point of a spectrum of disease that begins with asymptomatic cholelithiasis and biliary colic. In more than 90% of patients, acute cholecystitis occurs when gallstones cause an obstruction of the cystic duct, which in turn causes the gallbladder to become inflamed. With inflammation, the gallbladder becomes enlarged, tense, and reddened, with the possibility of a bacterial superinfection developing. 2 Emergent diagnosis of acute cholecystitis is imperative because without prompt treatment, patients may develop serious complications such as gangrenous, emphysematous, or perforated cholecystitis, resulting in the development of abscess or generalized peritonitis. 3
Sonography is the most commonly used initial imaging modality for the diagnosis of biliary disease. It is readily available, noninvasive, inexpensive, and accurate and does not expose the patient to radiation. Use of other methods for diagnosis, including hepatobiliary scintigraphy and computerized tomography (CT) of the abdomen, is limited due to availability, cost, use of ionizing radiation, and decreased sensitivity for detection of gallstones (75% with CT). 4 These studies are generally reserved for diagnostic dilemmas, subacute manifestations, or evaluation of complications. 4 Sonography has a sensitivity of 98% for the detection of gallstones. 5 It has a 90% to 95% sensitivity and a 78% to 80% specificity for the detection of cholecystitis. 6 Diagnosis of cholecystitis is accomplished by radiologically identifying markers of gallbladder inflammation, such as thickening of the gallbladder wall (3 mm or greater), presence of pericholecystic fluid, or positive sonographic Murphy’s sign (direct tenderness when the probe is pressed against the gallbladder). In a study involving 497 patients with suspected cholecystitis, the positive predictive value of the presence of gallstones with a positive sonographic Murphy’s sign was 92% and of the presence of gallstones with gallbladder wall thickening was 95%. 3 Because of the unpredictable timing, patients can be sent to the radiology suite for a timely sonographic assessment. However, because of the unpredictable timing of patient presentations, sonographers are not always available to perform radiology department studies. Sonography in the ED setting can also add to patient convenience and reduce emergency department length of stay. 7 Thus, emergency department physicians are increasingly being relied upon to make bedside diagnoses to determine the disposition of patients and the need for emergent surgical consultations. Due to this, they are increasingly being trained in the use of sonography. 8
Simulation Training
Simulation training in sonography has been shown be an effective method of teaching and assessing user competency in image acquisition/interpretation and performance of procedures. It allows for practice without harm to patients, standardization of education for trainees, and a flexible learning environment. 9 Several studies using simulation training have shown improved user performance, resulting in improved patient safety and quality of care.10,11 In a study comparing the effectiveness of using a sonographic simulator with using normal human models when teaching novice users the skills of obtaining and interpreting images for the Focused Assessment with Sonography for Trauma (FAST) examination, there was no difference between skill acquisition in the two groups. This suggests that the skills learned during simulation training can be directly applied to human models. 12 Gallbladder simulation models that are currently commercially available are torso section phantoms that represent a section of the upper abdomen with simulated ribs, liver, kidneys, gallbladder, and aorta. 13 They are intended for use during the initial stages of sonographer training and are generally expensive to obtain and require maintenance.
Gallbladder Model
Given the importance of simulation training and the lack of easily obtainable and inexpensive phantoms specific to the gallbladder on the commercial market, we have developed a sonographic gallbladder simulation model. With readily available and inexpensive materials, we were able to easily create models of normal gallbladder anatomy as well as various gallbladder pathologies such as cholelithiasis, biliary sludge, and thickening of the gallbladder wall. This model can be used to train users to obtain and interpret sonographic images of the gallbladder (Figure 1). The procedures for creating the phantom are listed in the appendix.

An operator imaging the gallbladder phantom with a phased array probe.
On the basis of a prior publication, 14 we created a gallbladder phantom using water, psyllium powder, unflavored gelatin, a latex glove, and olive oil. The psyllium powder scatters the sonographic beam, giving a sonographic image similar to human tissues. 15 The medium surrounding the gallbladder was made using previously described methods for creating phantom models,16,17 including the creation of the gel mold in thirds with the gallbladder floating in the middle layer. This was accomplished by first pouring a layer of gel mold into a glass loaf pan and allowing it to chill until firm in the refrigerator. Then, the second layer of the gel mold, into which the gallbladder model was placed, was poured onto the chilled first layer. After chilling the second layer until firm in the refrigerator, the third layer of the gel mold was made in the same fashion. The normal gallbladder was created by cutting off the index finger of a latex glove at the base and filling it with olive oil. The open end was tied in a knot, and the excess latex at the end was cut off. Cholelithiasis was simulated by adding a few small stones or whole peppercorns to the glove before the olive oil was added and the knot was tied (Figures 2 and 3). Biliary sludge was simulated by adding a small amount of sand or dirt to the glove before the olive oil was added (Figure 4). Simulation of a thickened gallbladder wall was accomplished by rolling the normal gallbladder model in olive oil and then rolling it in psyllium powder. After drying slightly, it was sprinkled again with psyllium powder to make a thick coating (Figure 5).
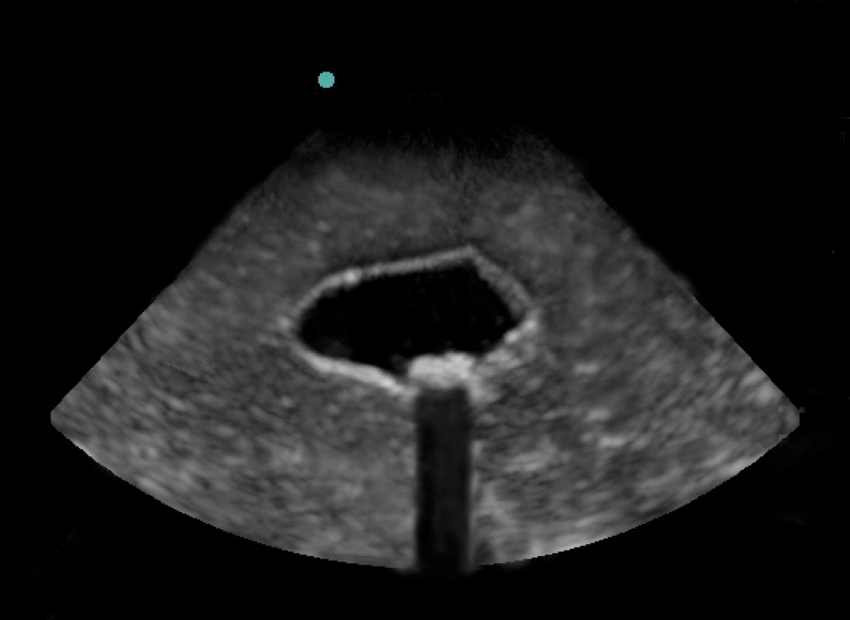
Small stones were added during preparation of the phantom to create the appearance of cholelithiasis with shadowing (long-axis view).
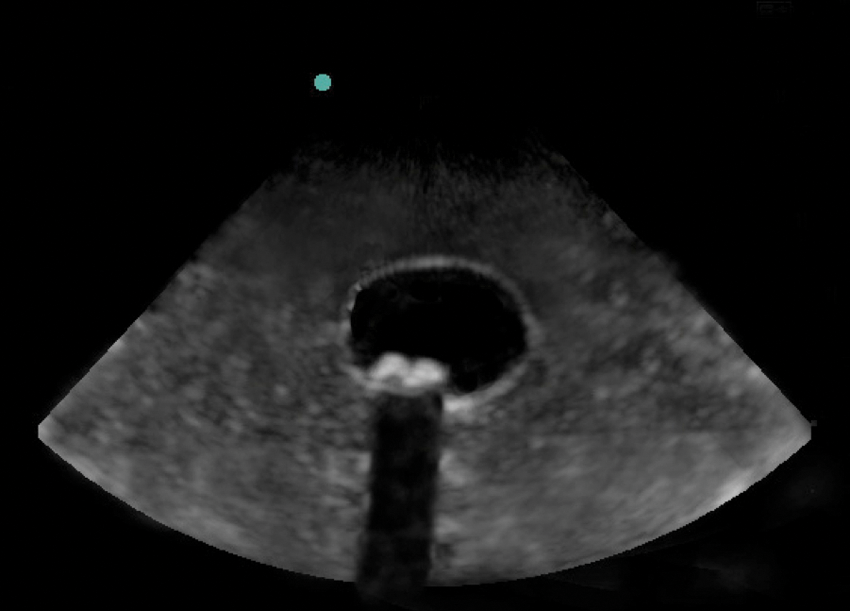
Short-axis view of the same phantom shown in Figure 2, mimicking cholelithiasis with shadowing.
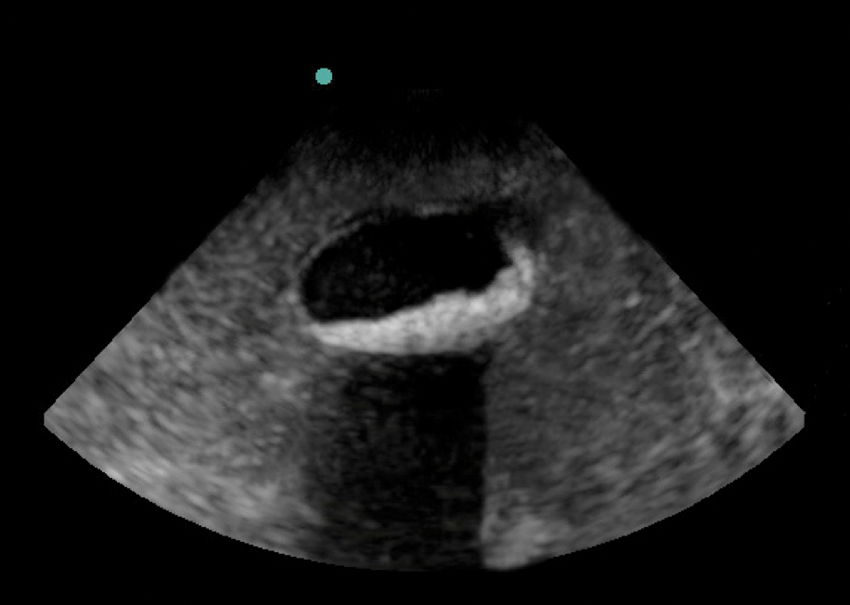
A small amount of sand was added during preparation of the phantom to create the appearance of biliary sludge with shadowing (long-axis view).
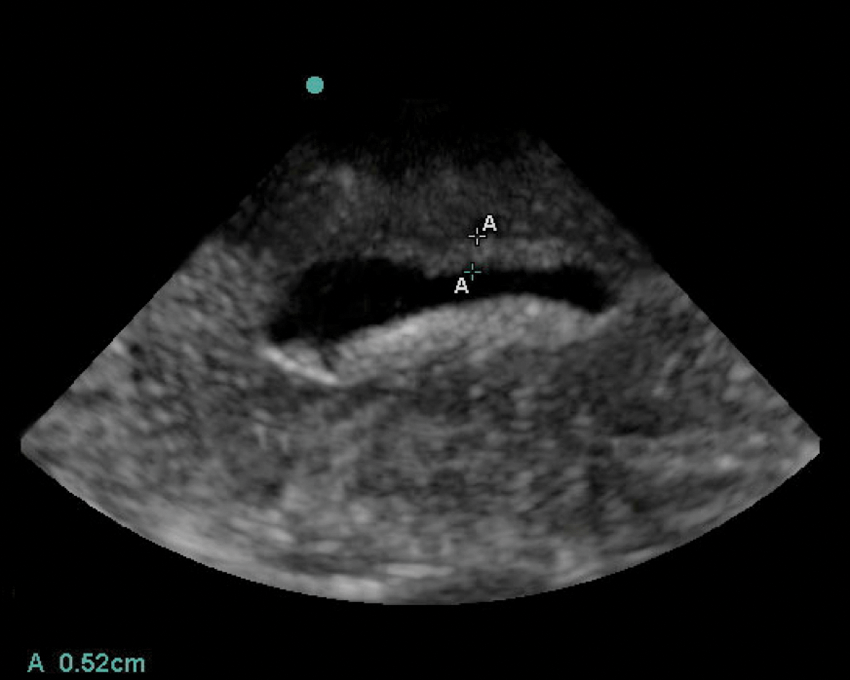
The normal gallbladder model was rolled in olive oil and then covered with psyllium powder to create the appearance of a thickened gallbladder wall measuring 5.2 mm (long-axis view).
The end product is a simulation model of biliary sonography that is inexpensive and easy to make. It provides realistic representations of both normal gallbladder anatomy and abnormal biliary conditions. The low cost and simplicity of creating this model make it an attainable and highly useful educational tool for attending physician, resident, sonography student, and medical student education.
Footnotes
Appendix: Procedure for Making the Gallbladder Models
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.