
Abstract
Objective:
The aim of this prospective study was to assess the frequency and clinical significance of incidental findings on upper gastrointestinal endoscopic ultrasonography (EUS).
Methods:
Patients referred for upper gastrointestinal EUS were consecutively enrolled into this prospective study. Any coincidental abnormality found during standard EUS was considered an incidental finding. Significant incidental findings were defined as abnormalities that required further medical, surgical, or endoscopic intervention, including surveillance.
Results:
In 552 patients who underwent EUS, 41 incidental findings were detected in 39 patients (7.1%). Twenty-one abnormalities had clinical significance. The frequency of incidental findings increased significantly with increasing age (P = .001). The most frequent incidental findings were gallstones, subepithelial lesions, and pancreatic lesions.
Conclusions:
Incidental findings on EUS are not uncommon in clinical practice and might be a clue to a significant pathology. The appropriate extent of evaluation of incidental findings noted during a standard EUS procedure warrants further research yet to be defined.
Introduction
The issue of reporting and managing incidental findings (IFs) is a growing problem, given the current advances in imaging technologies. When there is an unexpected finding on diagnostic imaging, the clinician faces the challenge to prove that the lesion is indeed harmless. In such cases, the relevance of the abnormal finding must be determined and the impact on the patient considered. It must be decided whether the abnormality is a simple, normal variation or clinically serious. Often, other tests are required to determine the exact nature of an incidentally found mass to determine whether, for example, it is a tumor or not. The relative medical benefit versus burden of disclosing such potentially important IFs is difficult to determine. 1
Our current knowledge about IFs is limited primarily to magnetic resonance (MR) imaging and computed tomography (CT). 2 Published studies suggest that 9%–15% of abnormalities found during abdominal sonography are incidental and unsuspected. 1
Endoscopic ultrasonography (EUS) has now become an established diagnostic procedure in a variety of common gastrointestinal (GI) disorders and is an important tool in clinical practice. Although there is extensive literature on the appropriate workup for some specific incidental findings, there are no clinical guidelines for the evaluation of incidental findings of the GI tract on EUS because of the sparse scientific data. We are reporting a prospective study of the occurrence and clinical importance of incidental findings on EUS of patients referred to our tertiary center hospital.
Methods
From May 2008 to May 2009, 552 consecutive patients referred to the gastrointestinal endoscopy department of Shariati Hospital (a university hospital center in Tehran) were eligible for inclusion in this prospective study. An incidental finding was defined as a finding concerning an individual patient that did not have any association with pretest clinical data, that was not detected on any previous imaging studies, that had potential clinical importance, that was not associated with the indication for the endoscopy, and that was discovered in the course of conducting a routine EUS. A significant finding was defined as any abnormality that required further medical, surgical, or endoscopic intervention, including surveillance.
The study was approved by the institutional review board of the Digestive Diseases Research Institute of Tehran University of Medical Sciences, according to the principles of the Declaration of Helsinki. Informed consent was obtained according to the guidelines of the institute. We reported every incidental finding to our patients. All subjects with abnormal findings were individually counseled about the problem, and they received detailed information on the nature of the apparent abnormality and medical advice for further management.
The endosonographer reviewed all medical records of patients before the EUS procedure to look for any abnormalities found before the EUS procedure. All EUS studies were performed by an expert endosonographer by using a radial EUS instrument (EG-3630UR, PENTAX Optical Co Ltd, Tokyo, Japan). A standard EUS procedure was defined and performed for all patients, regardless of the primary indication. Transduodenal, transgastric, and transesophageal sonographic evaluations were performed for detection of abnormalities in the pancreatobiliary system, paraluminal and intramural lesions including lymphadenopathies, ascites, and lesions in the left liver lobe. When a lesion requiring tissue diagnosis was found, an EUS-guided fine needle aspiration (FNA) using a convex array echoendoscope (Pentax EG-3830 UT) was performed. All FNAs were done using a 22-gauge needle (Echotip; Wilson-Cook, Winston-Salem, NC). Recorded data included patients’ age, sex, complaints, results of any previous laboratory workup and imaging studies, primary indications for EUS, and any incidental findings, including their location, size, and origin.
Incidental findings were categorized as:
Significant: Any IF that required prompt medical follow-up and further investigation, had an impact on the medical treatment, or required image-guided tissue sampling or operative treatment. These tissues included indeterminate masses in solid organs, enlarged lymph nodes and pancreatic cysts that required further diagnostic or therapeutic intervention.
Nonsignificant: Any IF not requiring additional investigation and treatment, such as gallstones.
To ensure provision of appropriate follow-up management, every patient was informed about the importance of the IF. To determine the final diagnosis, patients were contacted to see whether any follow-up examinations or procedures (eg, laboratory testing, repeat imaging, or interventions) were subsequently performed. In those patients with highly significant findings, the responsible physician was contacted directly, and details of the investigations and treatments relevant to each abnormality were requested.
Quantitative, continuous variables were evaluated using the mean ± standard deviation. Qualitative variables were expressed as percentages. The independent samples t test was used to compare the mean age of patients with and without IFs. A value of P < .05 was considered statistically significant.
Results
During the study period, 552 consecutive patients (52.5% male) underwent EUS examination. The age of participants was 53.2 ± 16.6 years (range 16–87 y). Forty-one IFs were found in 39 (7.1%) study subjects, 20 (51.3%) males and 19 (48.7%) females. Subjects with an IF were significantly older than those without IF (59.7 ± 16.0 vs 52.6 ± 16.5, P = .001). In the 39 patients with IFs, 27 were older than 50 years. Table 1 summarizes the results of 21 significant IFs. The most frequent nonsignificant IF was gallbladder stones (n = 18); none of these patients had abdominal symptoms.
Frequency of Significant Incidental Findings on Upper Gastrointestinal Endoscopic Ultrasonography (N = 21)
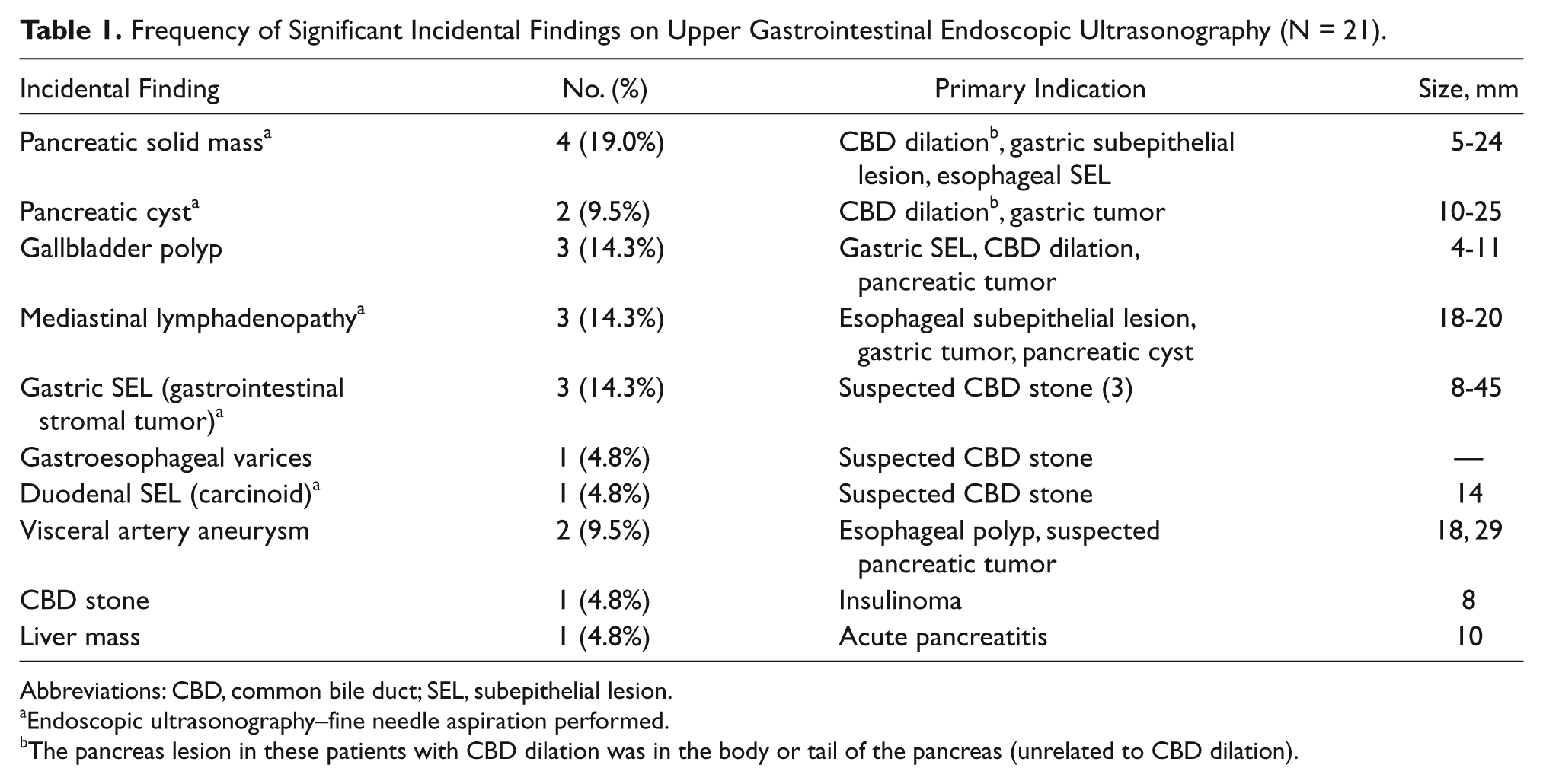
Abbreviations: CBD, common bile duct; SEL, subepithelial lesion.
Endoscopic ultrasonography–fine needle aspiration performed.
The pancreas lesion in these patients with CBD dilation was in the body or tail of the pancreas (unrelated to CBD dilation).
Pancreatic solid lesions were found in four patients, and all of them underwent EUS-FNA. A final diagnosis of resectable pancreatic cancer was made in one patient, and focal pancreatitis (these patients were followed for at least 12 months) was diagnosed in three (Figure 1A). Other significant IFs included: subepithelial lesions (four patients, Figure 1B); pancreatic cystic lesions in two patients (one pseudocyst and one patient with intraductal papillary mucinous neoplasm); a common bile duct (CBD) stone in one patient (Figure 1C) who underwent endoscopic retrograde cholangiopancreatography and stone extraction; two visceral artery aneurysms (one in the celiac artery and the other in the splenic artery, both ultimately confirmed by CT angiography); three large, bulky mediastinal lymphadenopathies (one patient with tuberculosis, one patient with sarcoidosis, and a third patient with non-Hodgkin’s lymphoma confirmed by CT/EUS-guided FNA); gallbladder polyps in three patients (one with adenomyomatosis and two others who did not undergo surgery); gastroesophageal varices (one patient, Figure 1D); and a liver mass in one patient, which was diagnosed as an atypical hemangioma. Overall, 21 (51.2%) abnormalities had clinical significance. Nonsignificant IFs were: gallbladder stones in 18 patients (42.9%), opium-induced CBD dilation in one patient, and a duodenal subepithelial lesion (duplication cyst) in one other patient.
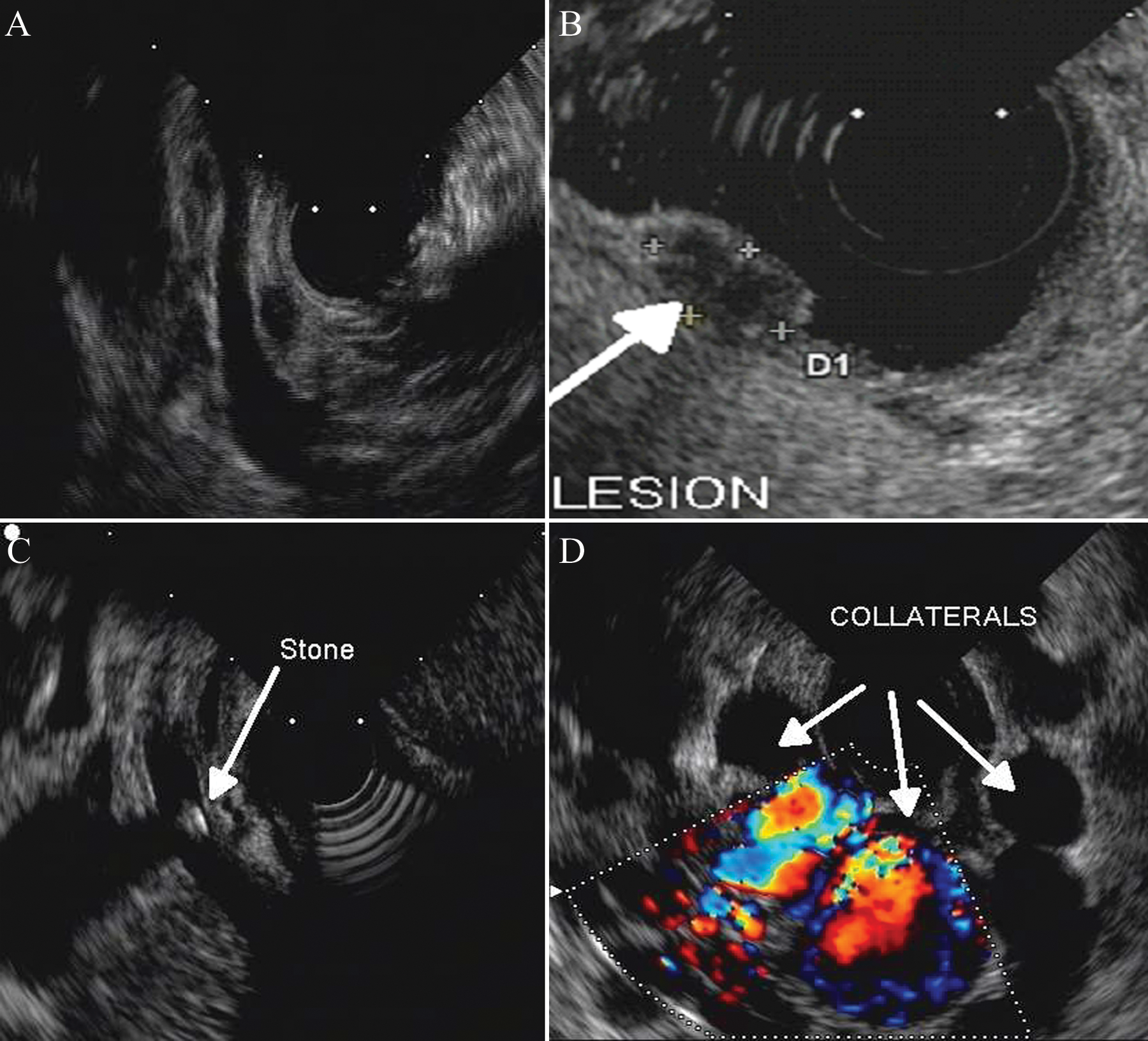
Examples of significant incidental findings: (A) A carcinoid tumor originating from the lamina propria layer of the duodenum (arrow); (B) A small 5 × 8mm tumor of the pancreas (arrow); (C) A small (3 mm) stone in the common bile duct, with posterior shadowing; (D) Collateral vessels associated with varicosities in the esophageal wall and para-esophageal region.
Discussion
In this study, the frequency of unexpected abnormalities was 7.1%, and over half of the detected lesions were considered clinically significant. The present study is one of the few complete investigations of IFs during EUS study. In a similar study by Vila et al, 3 the rate of incidental finding was higher than that of the present study, but a majority of these findings (such as thyroid nodules and thyroid cysts) were clinically irrelevant. They concluded that the rate of clinically significant findings is lower than the overall rate found in their study.
Previous studies of whole-body imaging using CT and MR and regional studies in healthy volunteers have documented higher rates of IFs in older populations in which the prevalence of a pathologic finding is likely to be higher. 2 Our study also indicates that the frequency of IFs on EUS is significantly higher in older subjects.
About 40% of all IFs were cholelithiasis in patients without biliary symptoms. It is estimated that only 20% of these patients will develop symptoms in their lifetime.4,5 In such cases, knowing the existence of the biliary lithiasis may facilitate the management of these patients. The importance of choledocholithiasis is obvious in early diagnosis and removal for prevention of serious complications, including biliary pancreatitis and cholangitis.
Pancreatic cysts accounted for 4.5% of IFs. Over 1% of inpatients at any time in a major medical referral center may have a pancreatic cyst detectable by CT or MRI. Up to one quarter of all pancreases examined in an autopsy series harbored a pancreatic cyst, and up to 10% of pancreatic cystic lesions were neoplastic in origin.6,7 In a large study by Bose et al, 8 the majority of pancreatic cystic lesions were identified during interpretation of a CT scan performed for staging of a nonpancreatic malignancy. Forty-one patients from 350 cases underwent resection, of whom 38 (92.7%) had premalignant or malignant pathology. Those investigators found that most benign lesions could be reliably identified at the outset, with a very low risk of missed malignancy or progression to primary pancreatic cancer.
The present study was not designed to address the utility of EUS for either screening or follow-up of patients with malignancies. The prevalence of IFs on imaging studies depends, in part, on the resolution and region examined in any study, and in the case of EUS, findings are certainly operator dependent. In some situations, the operator cannot make a specific diagnosis based on the EUS image. The clinical significance of each IF may also be different. Although the detection of a significant IF (such as a cystic lesion in the pancreas) would be important in an otherwise healthy patient, it may not be of the same value in a patient with a much more severe condition (such as a patient with advanced gastric cancer). Although smaller in number, the majority of significant IFs found in this study were of significant clinical importance and required additional treatment or a substantial change in the management of the patient’s disease. Examples are aneurysms of visceral arteries that may go on to rupture with potentially catastrophic consequences, mediastinal lymphadenopathy caused by tuberculosis, lymphoma, and pancreatic malignancies.
An additional benefit for doing a complete upper EUS is the potential to shorten the learning curve of examiners by improving the procedure technique. The learning curve for EUS can be very long, and a great deal of hands-on training is required to achieve adequate diagnostic accuracy.9-11 Full, extensive examinations can improve the technical skills needed to explore the different organs as needed. During the course of the present study, the practical results of this strategy for hands-on training of our fellows was noted, although the design of our study did not allow us to quantify this result.
Unlike upper and lower gastrointestinal endoscopy that involves a predefined, standardized, and thorough evaluation of the gastrointestinal tract, there is no such definition of a standard EUS procedure. This strategy may be easier to conduct using a 360° radial scanner rather than the linear scanner. Many endosonographers may prefer to tailor the instrument to the primary indication of the EUS evaluation. Imaging of the esophagus, for instance, is rarely performed during an EUS examination for pancreatic lesions. The time required for such a standardized EUS procedure, costs, legal issues, and its impact on long-term outcome of patients has not been studied. Considering the absence of any clinical or screening tools for early detection of upper gastrointestinal and pancreatic cancers, it may make sense to look for such lesions when the EUS device is in place and the opportunity is there. The results of our study raise such questions, and we believe that several longitudinal studies are warranted before we can choose between a targeted EUS by primary indication and a standard, more comprehensive EUS strategy. The finding of these abnormalities also warrants complementary studies of decision making for management and treatment. The abnormalities found by EUS were not described in any of the patients’ symptoms or laboratory findings, raising management issues at the time of discovery. The overall prognosis and quality of life of patients with gastrointestinal neoplasms is expected to be better with earlier diagnosis (incidental discovery during EUS) and treatment.
This study was limited to a single clinical setting, and the findings need to be confirmed in further studies in other centers. The main limitation of this study is that it did not determine the outcome of patients. The specific aim of the present study was to find the frequency of IFs during a standardized, comprehensive EUS procedure that required further medical attention; the study was not designed to follow the patients, though one of the main questions raised should be the impact of these IFs on the long-term outcome of patients. Only large, longitudinal studies with a follow-up of at least several years can address this question.
In conclusion, by performing a complete upper EUS, it is possible to diagnose incidental lesions in 7.1% of patients. Over half of these lesions are clinically important and account for 3.8% of cases. Further advantages of this strategy are the shortening of the EUS learning curve and the increased technical skills of the examiner. However, the impact on overall patient care of EUS screening during routine examination of the gastrointestinal tract requires further studies with long-term follow-up.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.