
Abstract
Pancreatic tuberculosis is an extremely rare condition. Its non-specific clinical and radiological findings resemble pancreatic malignancy. Here, we report a case of pancreatic tuberculosis that presented with abdominal pain and dyspeptic symptoms for 2 months and was misdiagnosed as a pancreatic cystic neoplasm. Abdominal magnetic resonance imaging showed a well-demarcated exophytic lesion with multiple T2 high signals small cystic areas in the anterior superior part of the head of the pancreas measuring 23 × 20 × 28 mm. This patient has undergone laparotomy and excision of the pancreatic mass. Histological examination revealed granulomatous inflammation of a lymph node with caseation, which was pathognomonic of tuberculosis. She was treated for tuberculosis for 6 months and has become symptom free. The diagnosis of pancreatic tuberculosis could be misleading and should be considered when dealing with pancreatic masses in countries with high incidence.
Introduction
Peripancreatic or pancreatic tuberculosis (TB) is a rare diagnosis, and the radiological findings may mimic a pancreatic neoplasm. 1 The rarity of peripancreatic Tb and the sinister nature of pancreatic neoplasms, often lead to misdiagnosis of TB as pancreatic malignancy or neoplasm. Furthermore, the diagnosis is often reached retrospectively following laparotomy for suspected pancreatic tumours. 2 Peripancreatic TB may present with a spectrum of specific or non-specific symptoms such as abdominal discomfort or pain, jaundice, constitutional symptoms, iron-deficiency anaemia, acute/chronic pancreatitis, pancreatic abscess, secondary diabetes, massive gastrointestinal bleeding, splenic vein thrombosis and a pancreatic tumours in imaging. 1 Due to the malignant potential of intraductal papillary mucinous neoplasm and mucinous cystic neoplasm, early resection in fit patients is recommended. 3 Pancreatic TB often presents in younger patients compared to pancreatic neoplasms, which are common in older patients. 4 We report a case of misdiagnosis of peripancreatic TB as a cystic neoplasm of the head of the pancreas.
Case
A 33-year-old female presented with vague upper abdominal pain and dyspeptic symptoms for 2 months. She was otherwise well with no fever, constitutional symptoms, loss of appetite or loss of weight and was normoglycaemic. Her previous medical and surgical histories were unremarkable. She had no known allergies and her drug and psychosocial history was unremarkable. Her basic biochemistry, including liver enzymes were within normal limits. Her erythrocyte sedimentation rate was 13 mm in the first hour. She was investigated with a gastroduodenoscopy and an abdominal ultrasonography as her symptoms did not resolve with a trial of proton pump inhibitors. Her abdominal ultrasonography revealed a rounded 2.5 × 2.4 cm lesion in the head of the pancreas with low echogenic areas.
Magnetic resonance imaging scans revealed a well-demarcated exophytic lesion with multiple T2 high signals and small cystic areas in the anterior superior part of the head of the pancreas measuring 23 × 20 × 28 mm (Figure 1). Following a multidisciplinary team discussion, a decision was made to perform a laparotomy followed by enucleation of the lesion, or Whipple procedure. The diagnosis was a pancreatic cystic neoplasm. An endoscopic ultrasound was not performed due to nonavailability. The CA 19-9 was within normal limits.

Computed tomography (a) magnetic resonance imaging (b) scans showing a well-demarcated exophytic lesion in the anterior superior part of the head of the pancreas measuring 23 × 20 × 28 mm.
She underwent a midline laparotomy and was found to have a well-defined exophytic firm to hard mass attached by a stalk to the upper border of the pancreatic head to the left of the hepatoduodenal ligament. The hepatic artery was densely adherent to the posterior surface of the mass. The mass was excised with a cuff of pancreatic tissue while carefully preserving the hepatic artery. Frozen section was not performed due to nonavailability in our institution. The postoperative period was uneventful.
The histology revealed granulomatous inflammation of a lymph node with caseation which was pathognomonic of tuberculosis (Figure 2). Unfortunately, specimen for TB culture was not sent as the diagnosis of TB was not suspected during surgery. Even though Zeihl–Neelsen staining was not performed on the specimen, TB PCR was performed in aspirated fluid of the surgical specimen, and it was positive. Chest X-ray was done following the diagnosis but was normal. She was started on category 1 anti-tuberculosis therapy, that is, quadruple anti-microbial therapy for 2 months followed by dual therapy with rifampicin and isoniazid for 4 months according to the local guidelines of management of extra-pulmonary TB. 5 At a follow up of 6 months, she was asymptomatic and further imaging was not performed.
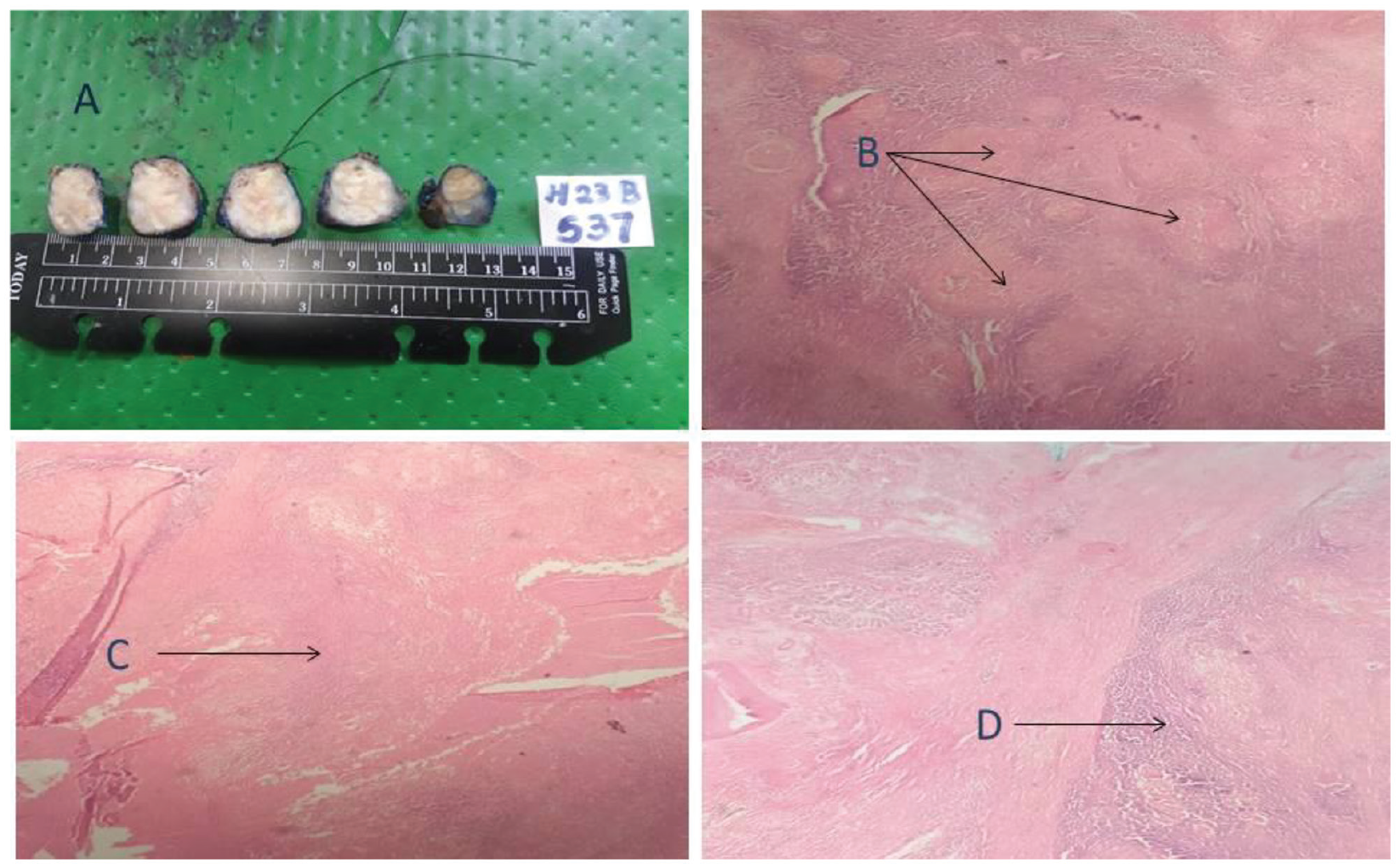
Surgical specimen and histopathological features of pancreatic tuberculosis.
Discussion
Incidence of tuberculosis in Sri Lanka in the last decade is around 3000–4000 cases per year. 5 Isolated pancreatic or peripancreatic tuberculosis is a very rare condition. 6 Considering the pathogenesis, pancreas is comparatively resistant to infection by bacteria due to its enzymes. 7
Xia et al. described 16 cases from China and suggested the following characteristics of pancreatic TB: ‘(1) mostly occurs in young people, especially female; (2) have a past history of TB, or come from endemic zone of active tuberculosis; (3) often present with epigastric pain, fever and weight loss; (4) ultrasound and CT scan show pancreatic mass and peripancreatic nodules’. 7 The lesions in the pancreatic cystic neoplasms mimic the radiological characteristics of pancreatic TB. 8 Pancreatic TB can be diffuse or local. If focal, it presents as a well-demarcated mass located in the pancreatic head, showing heterogeneous enhancement. Diffuse involvement is characterized by pancreatic enlargement with narrowing of the main pancreatic duct and heterogeneous enhancement. 9 Pancreatic cystic neoplasms show heterogenous in attenuation and internal septations. 10
Image-guided tissue sampling (Endoscopic ultrasound-EUS or CT) and pathological and microbiological examination is more reliable in diagnosing pancreatic tuberculosis. 11 In tissue examination, the presence of caseous granulomatous lesions. Typical epithelioid and gigantocellular granuloma is found in 60% of cases and rarely, caseous necrosis is seen. 12 Non-invasive approach of EUS with fine needle aspiration and TB PCR is used currently to evaluate patients with cystic neoplasms suspected to have TB.13,14 Pancreatic tuberculosis is a curable condition with multi-drug anti-tuberculous chemotherapy (streptomycin, rifampin, isoniazid, pyrazinamide and ethambutol), which is given for 6–12 months. 5 Response to treatment can be assessed symptomatically and radiologically. In our patient, the treatment was effective and the patient was asymptomatic at 6 months. Whipple’s pancreaticoduodenectomy was done in many reported studies for pancreatic tuberculosis because the most common presentation is pancreatic mass, which is difficult to differentiate from pancreatic cancer. 15 Performing intraoperative frozen section in a patient suspected of TB prevents radical resections. 16
Conclusion
Pancreatic tuberculosis is an extremely uncommon condition which is clinically and radiologically challenging to diagnose due to its mimicry with pancreatic cancer, and it can occur even in immune-competent patients. High degree of suspicion should be kept in mind when interpreting the radiological investigations especially in countries with high incidence of TB.
Footnotes
Acknowledgements
None declared.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed written consent
Written informed consent was obtained from the patient for anonymized information and accompanying images to be published in this article.