
Abstract
Various modalities of diagnostic imaging have been proven to be adequate in the characterization and diagnosis of ovarian neoplasms. This case study investigates a unique form of mucinous borderline ovarian tumor consisting of both intestinal and Müllerian types. Borderline tumors are considered an intermediate form of neoplasm between the benign and malignant form. Shortly after sonographic and magnetic resonance imaging, the large tumor was removed and the patient was determined to have an excellent prognosis. The utilization of sonography in diagnosing this tumor is discussed, demonstrating the significance of the technology.
Mucinous borderline ovarian tumors (MBOTs) are a form of ovarian neoplasm that consists of both benign characteristics of a cystadenoma and malignant components of a cystadenocarcinoma. Currently, there are three accepted, synonymous terms that describe MBOTs: borderline, low malignant potential, and atypical proliferation. 1 Therefore, this type of tumor is classified as an intermediate phase between benign and malignant. Mucinous borderline ovarian tumors account for approximately 30% to 50% of ovarian epithelial borderline tumors and are estimated to make up 10% of mucinous ovarian tumors.2,3 Mucinous borderline tumors are typically unilateral, but in about 5% of reported cases, they have been bilateral. 4 There are two forms of MBOTs depending on the type of epithelium from which it originated. The most common is the intestinal-type MBOT (I-MBOT) and, less commonly, the endocervical-type MBOT, also known as Müllerian type (M-MBOT) or seromucinous type.2,5
Sonography, magnetic resonance imaging (MRI), and computed tomography (CT) are all modalities used to evaluate MBOTs. For lesions indeterminate on sonography, MRI increases the specificity of imaging evaluation, thus decreasing benign resections, whereas CT is useful in the diagnosis and management planning of more advanced cancers. 6 The case reported below illustrates a patient with a mucinous borderline ovarian tumor and the diagnostic imaging tests used in the detection and diagnosis of the pathology. Sonography and MRI were key in this patient’s diagnosis and treatment, in which sonographically the tumor was evaluated locally, and large-scale assessment was done with MRI.
Case Report
A woman in her late teens presented to the emergency room with complaints of abdominal and pelvic pain. Upon the initial physical examination, she was found to have a protruding abdomen and appeared as if she could be pregnant, possibly in her late second to third trimester. Initially, a transabdominal pelvic sonogram was ordered. The patient stated she was not, nor had she ever been, sexually active; therefore, a pregnancy test was not done and an endovaginal sonographic examination was not included. Blood testing for markers such as CA125 or CA19-9 also was not done during the initial workup and evaluation. A curvilinear transducer with a center frequency of 4 MHz was used for this study on a GE Logiq E9 machine (GE Healthcare, Piscataway, New Jersey).
The sonogram revealed a very large mass inhabiting the entire pelvis and extending approximately 2 cm above the umbilicus. The origin of the mass was unable to be identified due to the sheer size of the mass obscuring pelvic organs. Because of its size, the entire lesion could not be adequately measured on a single sonographic image. Approximations of the mass’ dimensions were taken at midline measuring 20.38 cm long, 16.37 cm anterior-posterior (AP), and 20.75 cm wide (Figures 1 and 2). The uterus and ovaries could not be documented properly because of the prominent mass. No free fluid was identified. The mass was complex, consisting of both cystic and solid components, and particular attention was paid to imaging and analyzing these separate components. As the mass shared characteristics of both benign and malignant categories, it was initially treated as malignant until surgically and pathologically proven otherwise.
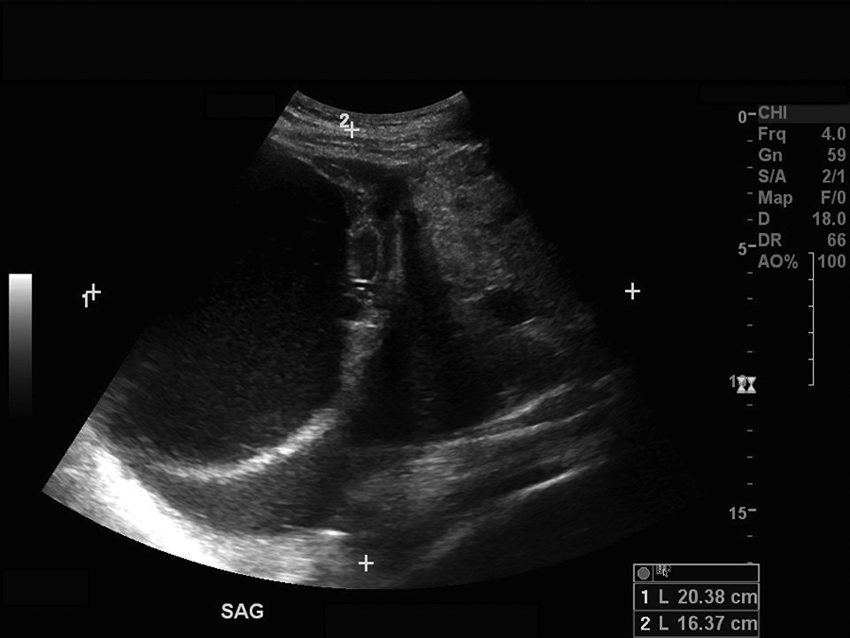
Sonogram demonstrating the midline approximation of the pelvic mass in a sagittal plane.
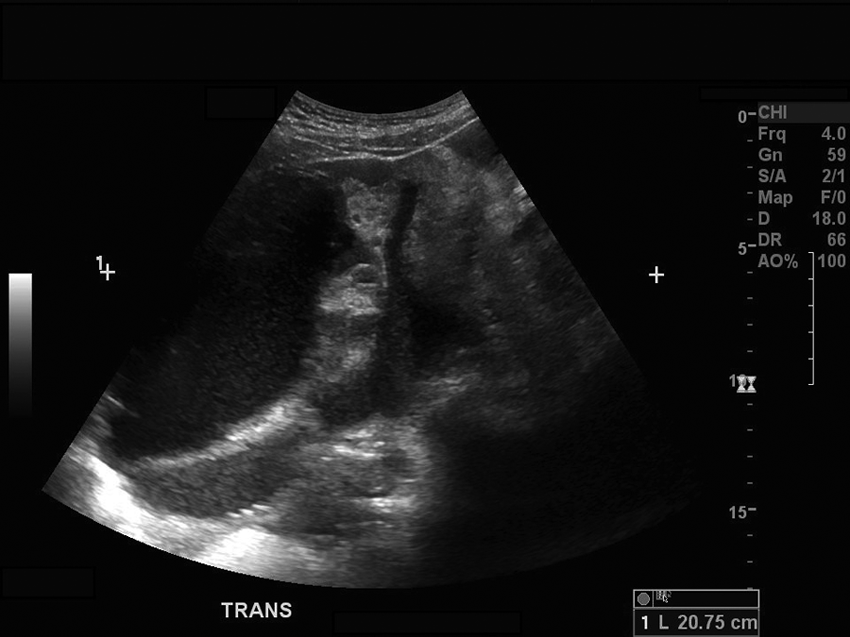
Sonogram demonstrating the midline approximation of the pelvic mass in a transverse plane.
Two predominate areas of the pelvic mass were clearly imaged on the sonographic examination. The superior portion of the mass appeared as cystic and fluid filled. The superior aspect of the mass exemplified the classic characteristics of a cystic, benign lesion, including an anechoic lumen, well-defined borders, and posterior acoustic enhancement. The cystic lesion was measured in sagittal and transverse planes at 12.93 cm long, 9.24 cm AP, and 13.82 cm wide (Figures 3 and 4). Upon evaluation with color Doppler imaging, the cystic portion of the mass demonstrated little to no vascularity surrounding or within the structures (Figure 5).
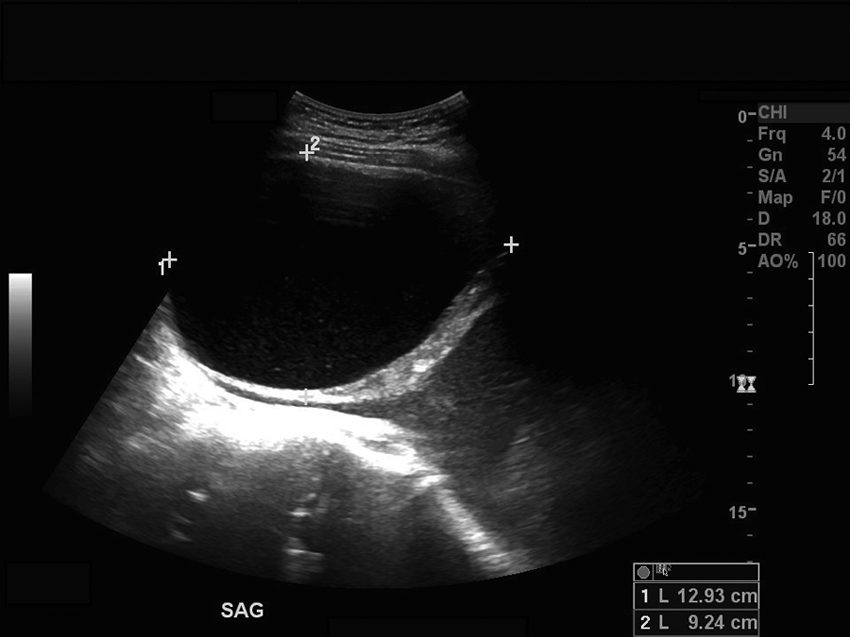
Sonogram demonstrating the superior, cystic component of the mass in a sagittal plane with measurements.
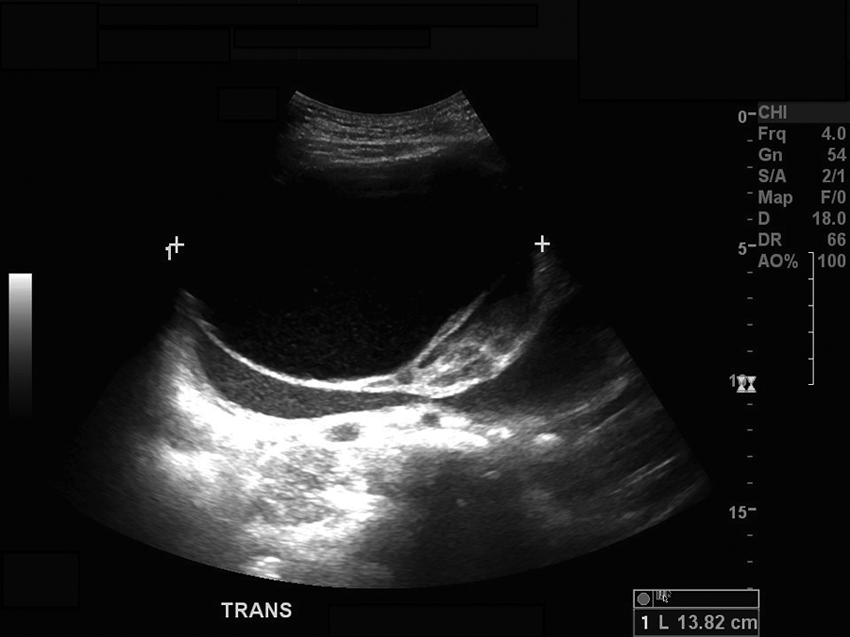
Sonogram demonstrating the superior, cystic component of the mass in a transverse plane with measurement.
Sonogram demonstrating the superior, cystic component of the mass with color showing little to no vascularity surrounding.
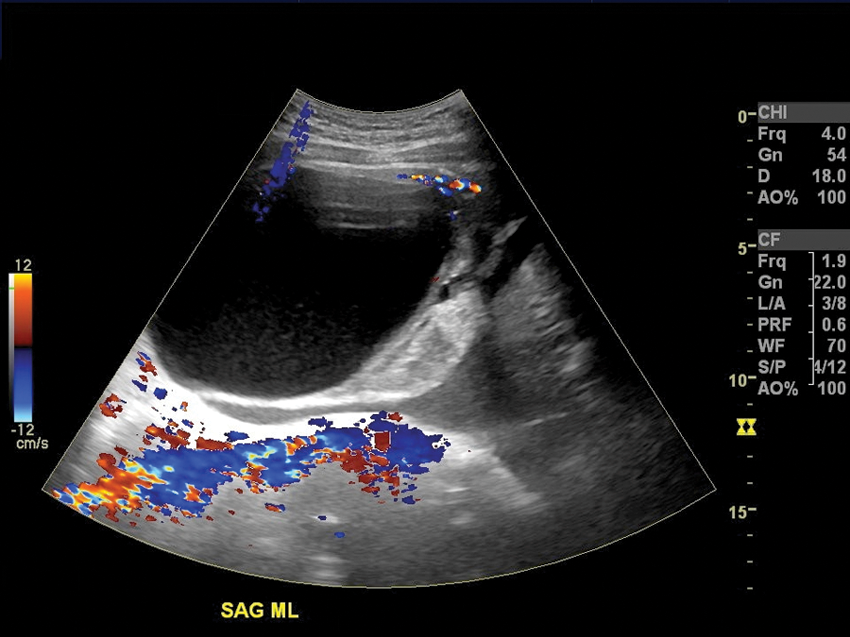
The inferior portion of the mass was shown to be complex and solid, more malignant in appearance on the sonogram. Measurements of the heterogeneous, solid component were again taken in sagittal and transverse planes at 15.20 cm long, 15.91 cm AP, and 18.12 cm wide, respectively (Figures 6 and 7). As with any lesion, color Doppler imaging was applied, which showed qualities similar to the superior aspect of the lesion, with little to no flow (Figure 8). Ovarian neoplasm was suspected and surgical intervention was recommended.
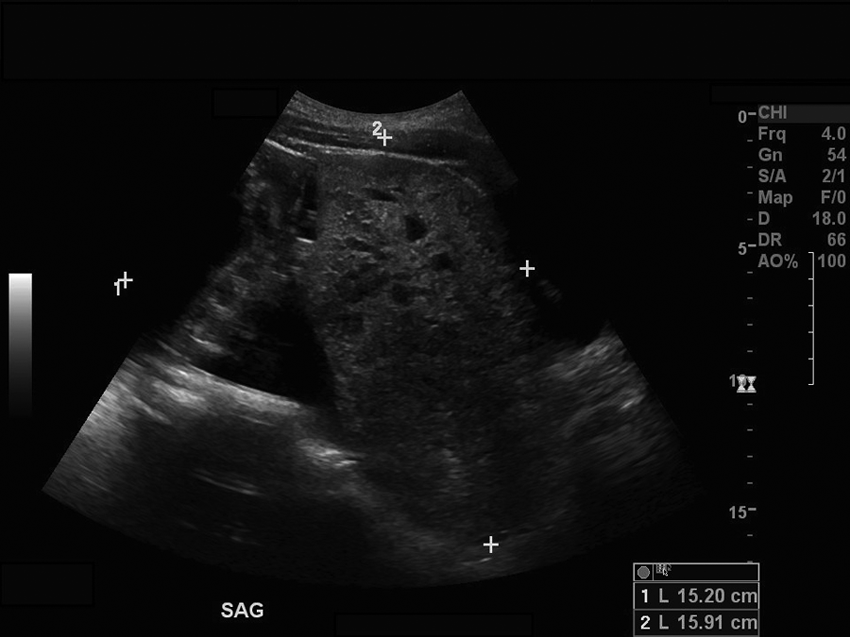
Sonogram demonstrating the inferior, heterogeneously solid component of the mass in a sagittal plane with measurements.
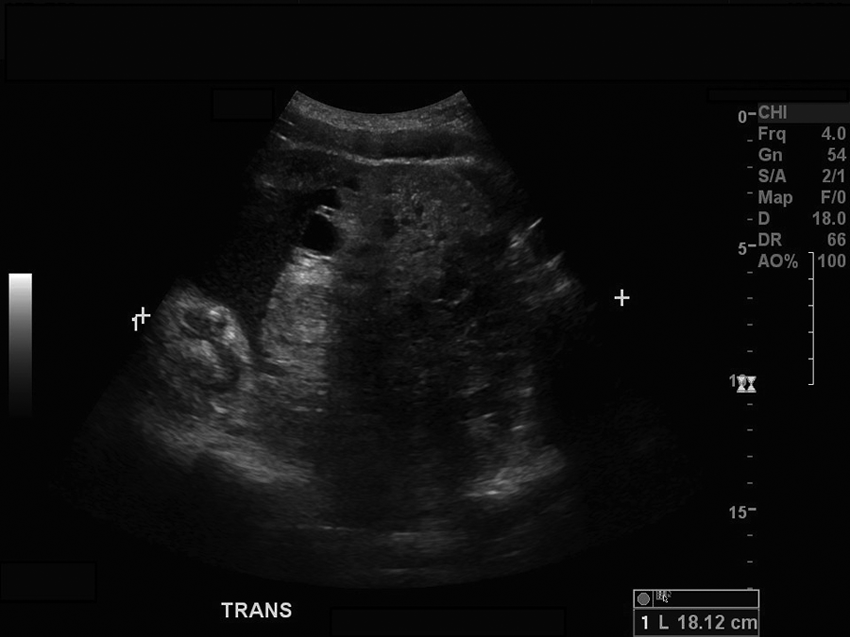
Sonogram demonstrating the inferior, heterogeneously solid component of the mass in a transverse plane with measurement.
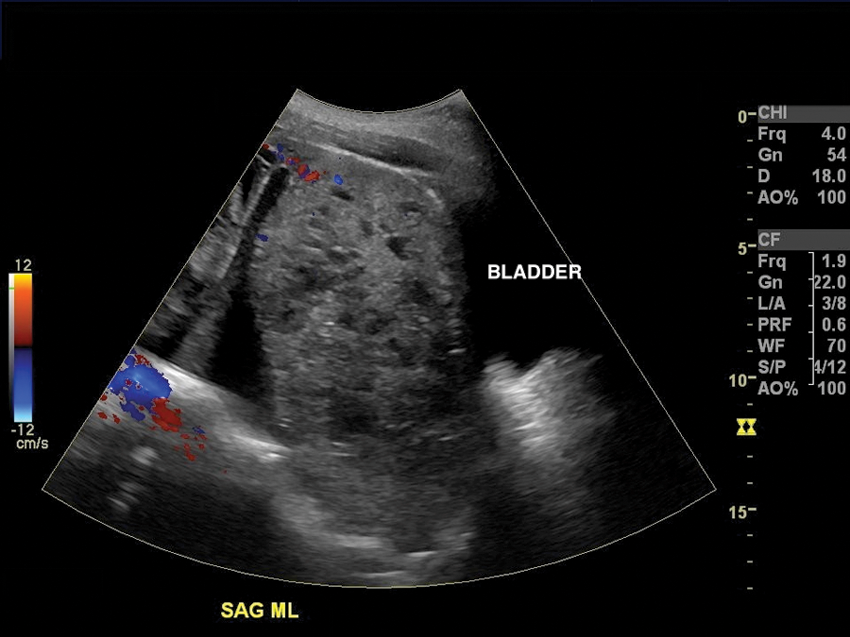
Sonogram demonstrating the inferior, heterogeneously solid component of the mass with color showing little to no vascularity surrounding or within.
Magnetic resonance imaging with and without gadolinium contrast was used five days later to supplement the findings of the sonogram. Whereas the sonogram was able to examine the two aspects of the lesion individually well, the MRI was able to offer a more global view of the lesion as a whole. In addition, findings of the MRI included right-sided hydronephrosis (Figure 9A), bowel displacement, bladder displacement, and an atrophic uterus, all felt to be secondary to compression by the mass.
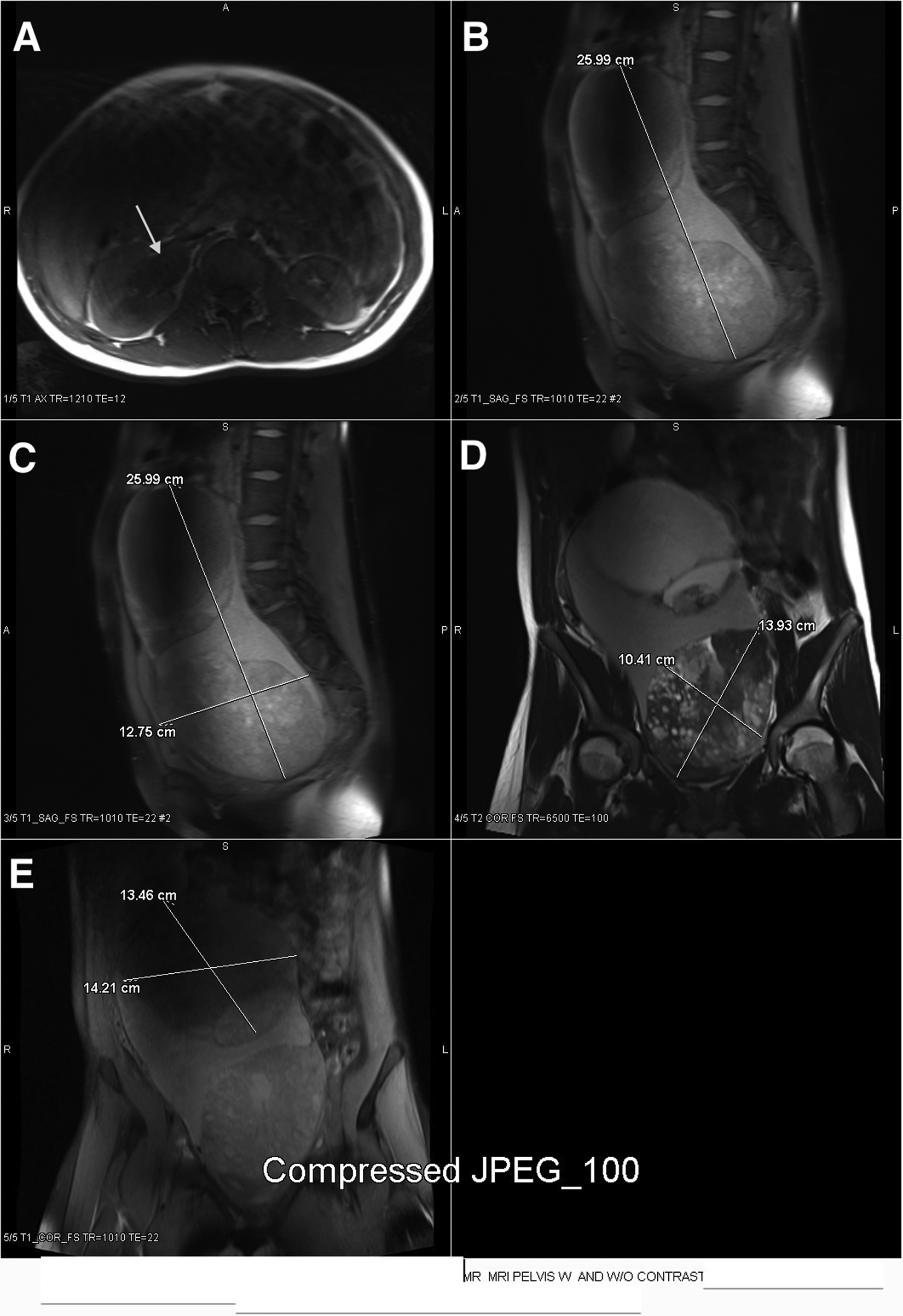
Magnetic resonance images depicting the bilobed, ovoid pelvic mass. As shown by the arrow, hydronephrosis of the right kidney due to compression of the ureter by the mass (A). Measurements of the entire pelvic mass from superior-to-inferior (B) and transverse (C). Measurements of the inferior, heterogeneously solid lobe of the pelvic mass (D). Measurements of the superior, cystic lobe of the pelvic mass (E).
The MRI results were comparable to the sonogram in that the lesion was classified as a bilobed, ovoid pelvic mass. In total, the mass measured 25.99 cm superior-to-inferior, 12.75 cm AP, and 15.5 cm transverse at the level of the iliac crests (Figure 9B,C). The inferior lobe measured 13.93 by 10.41 cm (Figure 9D). Images of the superior component of the lesion correlated with the previous examination, and it was again determined to be cystic in nature, measuring 13.46 cm superior-to-inferior and 14.21 cm transversely (Figure 9E). Postcontrast, the inferior portion of the mass proved again to be solid and complex with internal cystic changes. No free fluid was identified on MRI, also supporting the findings of the pelvic sonogram. The origin of the mass was identified and confirmed as right ovarian.
Following the sonogram and MRI, an exploratory laparoscopy was done with a right oophorectomy and pelvic washing. Surrounding organs and structures were noted to be unremarkable. However, after attempting to remove the right ovary containing the mass laparoscopically, a small rupture was noted in the capsule of the mass, which was seen to be releasing a dark green fluid outside the abdomen. The procedure was converted to an open laparotomy at that time for complete removal and to avoid further complications. At excision, the mass was approximately 21 cm in its greatest dimension. Once the ovary and mass were excised, the remaining pelvic organs were examined and determined to be free of pathology, hemostasis was achieved, and the atrophic uterus was repositioned into its normal place in the pelvis. On completion of the surgery, the patient was in stable condition and sent to recovery. Histopathologic analysis of the mass gave a diagnosis of a mucinous borderline tumor of both I-MBOT and M-MBOT types, without evidence of malignant cells or invasion. Subsequent to the removal of the mass, the patient’s symptoms, such as flank pain secondary to the hydronephrosis due to compression of the ureter, subsided shortly after surgery. Prognosis of the patient was considered excellent, and future fertility was preserved due to the unaffected left ovary. The patient did not require any further treatments with an uneventful recovery and discharge; however, it was recommended that the patient undergo future blood testing for malignant markers such as CA125 and CA19-9.
Discussion
Diagnostic imaging techniques were crucial in the evaluation, classification, and treatment for this patient. Sonographically, the mass showed both characteristics of a benign and malignant nature. Common benign characteristics on a sonogram include cystic appearance; posterior enhancement; round, smooth, and well-defined borders; and lack of blood flow. Malignant characteristics of a lesion on a sonogram typically are a complex, heterogeneous, or solid appearance; ill-defined borders; lack of posterior enhancement and/or shadowing; irregular shape; and increased vascularity. The superior portion of the MBOT in this case appeared benign with its cystic appearance and lack of blood flow. The inferior mass demonstrated both benign and malignant characteristics. The benign characteristics included lack of blood flow, whereas the complex appearance could be suggestive of malignancy. Sonographically, the size and position of the mass prevented adequate visualization of the other abdominal organs of interest. On MRI, the findings of the sonographic evaluation of the MBOT were supported and comparative. In addition, it was evident on the MRI as to why the patient was experiencing the symptoms due to the compression of the multiple abdominal organs.
Since MBOTs tend to arise during childbearing years, the management is important as it may significantly affect the patient’s ability to become pregnant in the future. Surgical treatment for borderline ovarian tumors resembles that for ovarian cancer. 7 Cystectomy has been shown to increase the chance of preserving fertility, but it is associated with a higher rate of recurrence than oophorectomy. 7 As with this case, a unilateral oophorectomy was performed, conserving the patient’s fertility and virtually eliminating the chance of recurrence. Survival rates of MBOTs caught early are estimated to be 98% to 99%. 5 A study of 900 cases reported that aggressive behavior is very rare and most likely attributed to inadequate sampling failing to detect invasion or the neoplasm was a metastatic lesion from an occult primary source elsewhere. 5 Imaging techniques, as with this particular case, are very helpful in excluding the latter.
The use of a variety of imaging techniques is also important for the exclusion of advanced pathological processes and other types of ovarian neoplasms with less favorable outcomes. Mucinous borderline ovarian tumors can occur in association with other benign or low-grade malignant tumors. Brenner tumors (transitional cell) are most commonly associated with MBOTs, as well as teratomas and Sertoli-Leydig cell tumors. 5 Metastatic evolution of the tumor is possible with MBOTs. On both sonographic and MRI images, the tumor in the case reported appeared isolated, and no free fluid suggesting malignant transformation was identified.
Conclusion
In conclusion, sonographic imaging alone would have been insufficient with respect to this case because the large size of the mass obscured pelvic and abdominal organs. The combination of sonographic and MRI imaging provided adequate evaluation, leading to the appropriate treatment plan for the patient. Sonographic examination, with the aid of MRI techniques, proved to be advantageous for the characterization, diagnosis, and prognosis in this case of a mucinous borderline ovarian tumor.
Footnotes
Acknowledgements
The author thanks Darla McQuitty, RT(R), RDMS; Emily Melville, RDMS; Breanna Wells, RDMS; Andrea Frazier, RT(R), RDMS; Kim Tippin, RT(R), RDMS; Shawnda Conner, RT(R); and Dr John Waddell for their assistance, leadership, and guidance.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.