
Abstract
A 43-year-old South Korean male presented to urgent care with pain free jaundice and weight loss. An abdominal ultrasound was ordered and demonstrated a 2.5 cm irregularly contoured ampullary mass that was obstructing the common bile duct (CBD). Endoscopic biopsy demonstrated ampullary villous adenoma with high grade dyspasia. Villous adenoma is a type of polyp typically found in the colon, but it is rarely seen at the ampulla of Vater. To our knowledge this is the first documented case found by transabdominal sonography.
Introduction
Villous adenoma is a type of polyp typically found in the colon. It is rarely seen at the ampulla of Vater.1–3 We present a case of a villous adenoma of the ampulla of Vater detected during transabdominal sonography.
Case Study
Abdominal sonography was ordered for a 43-year-old South Korean male presenting with symptoms of painless jaundice and weight loss. Sonography was performed utilizing an iu22 Phillips Medical ultrasound system, which showed severe intrahepatic ductal dilatation. The common bile duct (CBD) was dilated along the head of the pancreas. The CBD then tapered down to a point at the sphincter of Oddi terminating up against a 2.5 cm irregular contoured mass, which was seen to be partially obstructing and lying within the second part of the duodenum (Figures 1A, 1B). Incidental findings of the sonographic examination were two small solid liver lesions with “target” appearance. Computed tomography (CT) confirmed these findings the next day (Figures 2A, 2B, 2C). Directly following CT an esophagogastroduodenoscopy (EGD) was done with biopsy of the mass, which found villous adenoma with high grade dysplasia on the ampulla of Vater. At that time the patient refused any further medical intervention and returned to his native country.
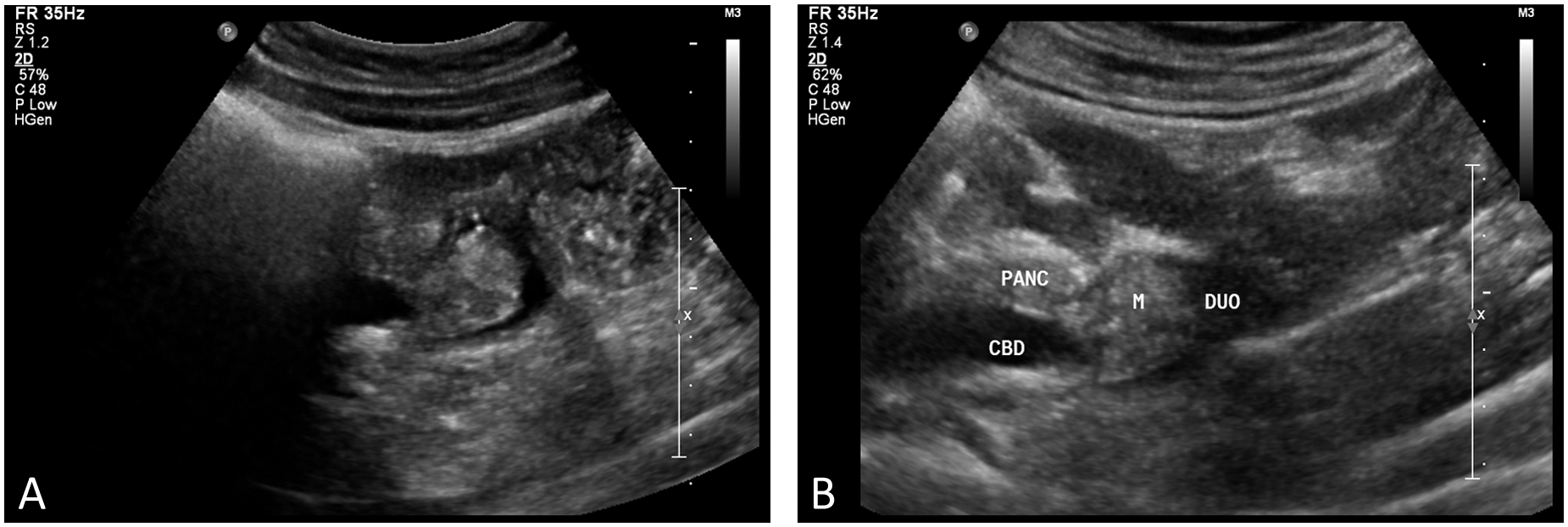
Sonograms of the dilated common bile duct (CBD) as it passes through the head of pancreas (PANC) and then tapers before it terminates at the mass (M) seen at the ampulla of Vater. The mass was seen to lay within the second part of the duodenum (DUO).

Computed tomographic (CT) cross-sectional image showing the distal descending duodenum and third part as it passes between the superior mesenteric artery and aorta. The mass is seen here within the duodenum just before it turns to the left.
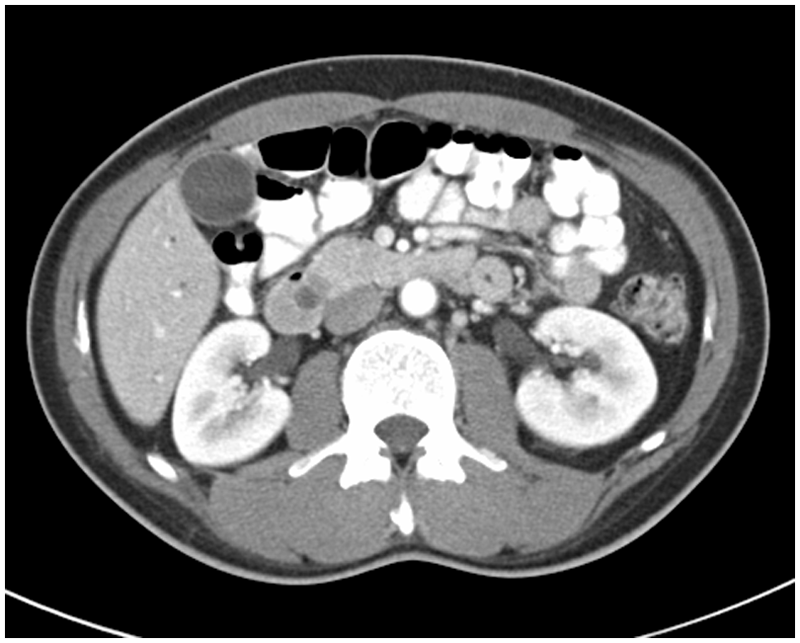
CT image shows the distal CBD terminating at the mass.
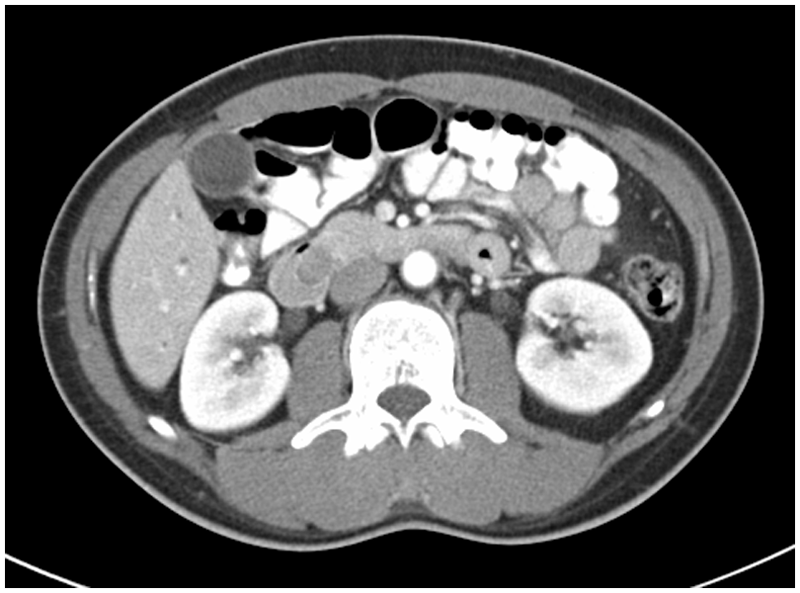
Additional CT image showing the mass in the descending duodenum.
Discussion
Villous adenoma is a type of polyp usually found in the colon. 3 Villous adenoma of the ampulla of Vater was first documented in 1928 by Golden. 1 Although rare, villous adenoma of the ampulla of Vater is typically found and diagnosed based on CT and EGD. It may also be suspected based on a filling defect found on plain film x-ray. Ampullary adenomas can occur randomly or in the context of genetic syndromes such as familial adenomatous polyposis (FAP). 4 Villous adenoma with high grade dysplasia is considered to be precancerous. Villous adenoma may become malignant, and lesions have been shown to contain malignant portions in approximately one third of patients. 2 Ampullary adenomas cannot always be distinguished from ampullary carcinomas, pancreatic carcinomas, or nonadenomatous polyps on the basis of endoscopic appearance alone. Suspicious ampullary lesions should be biopsied before an endoscopic resection is attempted. 4 Treatment for a benign villous adenoma is often local excision. For malignant villous adenoma a Whipple procedure is most often done, with a good prognosis if a complete excision can be done.1,2
There is no clear consensus on which ampullary adenomas should be under surveillance and which lesions should be removed endoscopically or surgically. Lesion size is a consideration as depending on the clinical picture, a small incidental ampullary adenoma may not require further evaluation or therapy. There are no definitive guidelines as to the size above which endoscopic removal of the ampullary adenoma should not be attempted. Many authors suggest open surgical removal of lesions over 4 to 5 cm. 4
As the advancement of ultrasound technology continues, Sonographers and radiologists will be able to see smaller lesions more clearly and reach a diagnosis more often. It is often no longer adequate to simply refer to the size of the CBD without commenting on the underlying etiology of any dilation seen. Sonography can also determine the vascularity of a mass that may signify the angiogenesis that is present in precancerous and cancerous lesions. Sonography is also able to define the characteristics of a mass and help determine its mobility. The Sonographer must always pursue these additional facts and go beyond older, traditional protocols to better define any pathology present. This pursuit is paramount to patient safety, management, and the planning of any interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.