
Abstract
Fetal intra-abdominal umbilical vein varix (FIUVV) is an uncommon finding with poorly understood clinical significance. Numerous fetal complications are associated with this anomaly. This case report demonstrates FIUVV in which thrombus develops leading to early induction of labor for successful delivery. The literature regarding FIUVV is reviewed and discussed with implications for sonographic follow-up during pregnancy and patient management.
Fetal intra-abdominal umbilical vein varix (FIUVV) is defined as an umbilical vein that is at least 50% wider than the nondilated portion or dilation of 9 mm or greater. 1 FIUVV is an uncommon abnormality with poorly understood clinical significance. Only 200 cases have been reported in the past 20 years. A study from Fung et al 1 indicated that additional sonographic abnormalities were detected in 31.9% of fetuses with a 13% prenatal loss rate. There is an association of fetal malformations, fetal death, and chromosomal abnormalities; however, more recent studies indicate good fetal outcomes with isolated FIUVV. 2 A comprehensive study by Mankuta et al. 2 identified 28 cases of FIUVV out of 65,000 births over a 15-year period, with a prevalence of 1 case per 2300 births, and estimated that FIUVV represents 4% of umbilical cord abnormalities. 3
FIUVV thrombus or clot is an extremely rare entity and requires close observation and management. Thrombus can block fetal venous circulation and cause sudden fetal death.2,4 This case follows one FIUVV thrombus through diagnosis, management, and successful delivery.
Case Report
A woman in her early 20s, gravida 1, para 0, presented for her initial sonogram at 19 weeks. The sonogram was normal other than a moderately echogenic bowel (Figure 1). The patient was referred to maternal fetal medicine, which confirmed the echogenic bowel, and an infectious etiology was suggested based on lab titers. The patient had negative herpes simplex type 1 and two IgG titers but an equivocal herpes simplex IgM. Repeat herpes simplex IgM subsequently was positive. Amniocentesis demonstrated normal chromosomes and no intra-amniotic infection. The patient was started on acyclovir, serial growth scans were recommended, and the patient returned to our care. The patient’s 33-week growth scan demonstrated an approximate 1-cm FIUVV adjacent to the fetal bladder (Figures 2 and 3). Twice-weekly Doppler and biophysical profiles scans were initiated to search for thrombus or signs of fetal compromise. At 35 weeks, thrombus was detected within the varix (Figures 4 and 5).
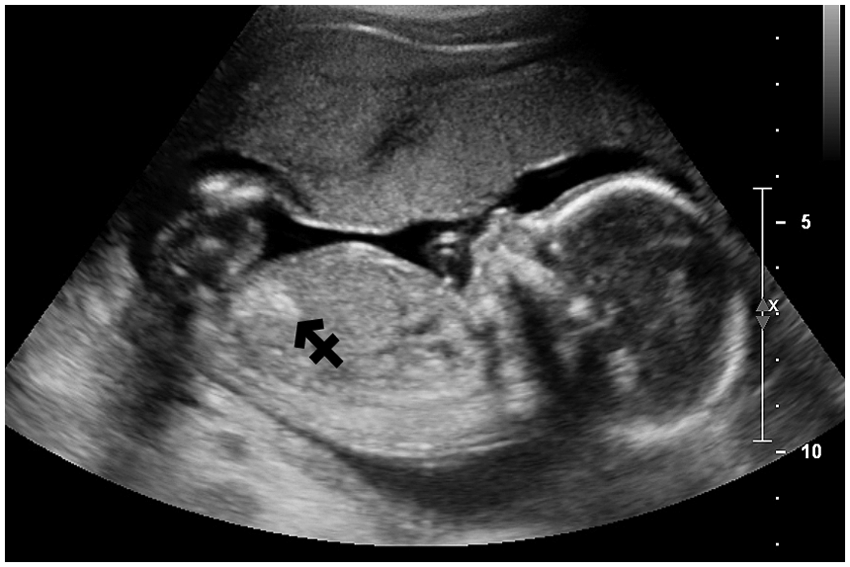
Initial 19-week fetal sonogram showing echogenic bowel (arrow).
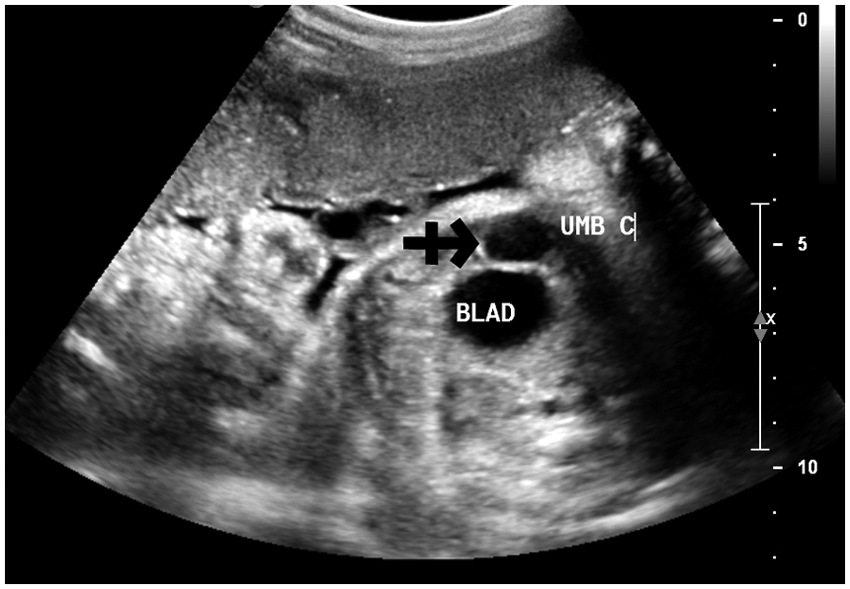
Follow-up 33-week fetal sonogram demonstrating a fetal intra-abdominal umbilical vein varix adjacent to the bladder (arrow).
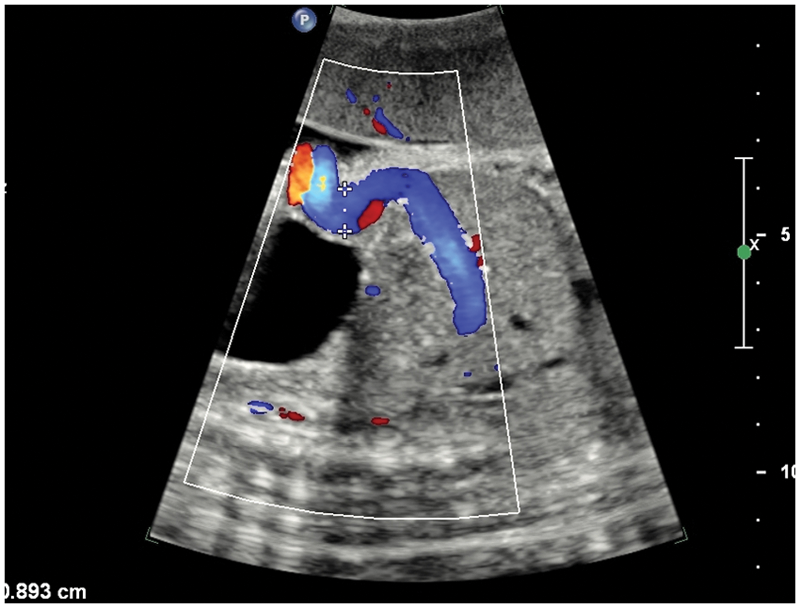
Follow-up 33-week fetal sonogram with color Doppler imaging of the fetal intra-abdominal umbilical vein varix, which measured approximately 9 mm.
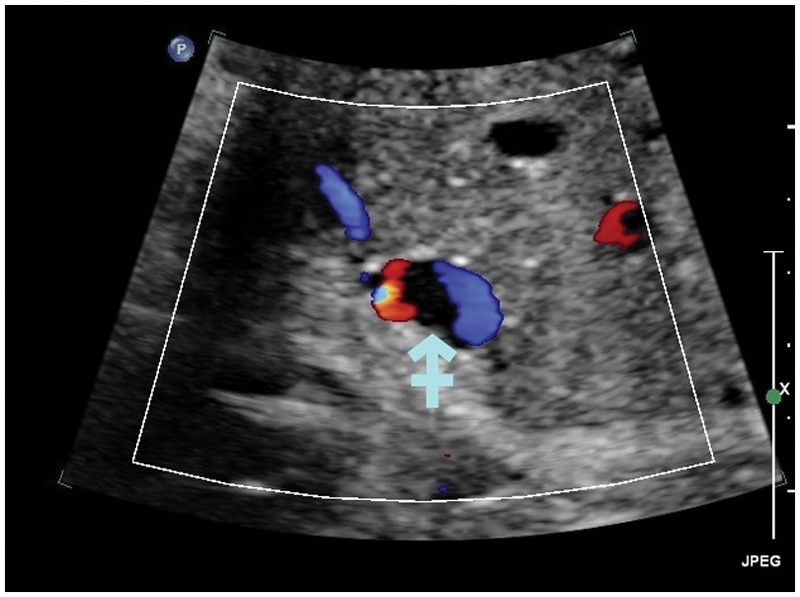
Fetal sonogram at 35 weeks with transverse color Doppler imaging demonstrating thrombus within the fetal intra-abdominal umbilical vein varix (arrow).
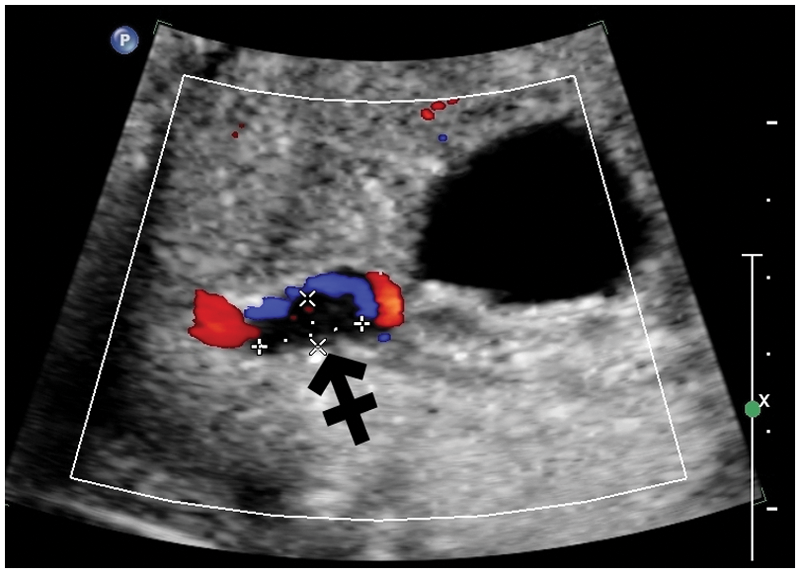
Sagittal color Doppler image of the thrombus seen in the fetal intra-abdominal umbilical vein varix at 35 weeks (arrow).
On the basis of the diagnosis of varix thrombus at 35 weeks and the potential for fetal complications from FIUVV thrombus, the patient underwent induction of labor. Continuous fetal monitoring was employed. The fetus developed repetitive variable heart decelerations, so a primary low transverse cesarean section was performed. A stable 2380-gram female with Apgar scores of 8 and 10 was delivered. There were no apparent signs of intrauterine growth restriction or infection.
Discussion
Diagnosis of FIUVV is defined by an umbilical vein that is at least 50% wider than the nondilated portion or dilation of 9 mm or greater. 1 Due to increasing awareness and improved imaging technology, the frequency of diagnosis has increased in the past several years. However, the diagnosis of FIUVV thrombus remains very rare and is made by evidence clot within the varix. Only a few cases have been documented worldwide. Diagnosis is suggested with the sonographic finding of an anechoic structure adjacent to the fetal urinary bladder. Color Doppler is performed to determine vascularity and search for thrombus, which is characterized by local flow disturbances or, in the case of complete thrombosis, an absence of flow.
The diameter of the typical intra-abdominal umbilical vein increases approximately linearly from 3 mm at 15 weeks to 8 mm at term. 5 Detection of FIUVV should prompt a thorough examination of the fetus to look for any additional sonographic anomalies, including a fetal survey and echocardiography.1,3 Close observation and regular surveillance, including Doppler examinations and biophysical profiles, are indicated when FIUVV is seen. Fetal hemolytic disease should be ruled out, and karyotyping should be considered if other anomalies are present.
There are considerable differences reported in fetal outcome in the published FIUVV studies.1,5,6 Recent studies show improved detection rates, likely due to equipment advancements and practitioner awareness. 2 Outcomes have been shown to be better when diagnosis of FIUVV occurs late in pregnancy.1,7 The authors surmise that improved outcomes are due to the presence of an isolated FIUVV, not complicated by other fetal abnormalities. Still, evaluation is necessary to rule out associated malformations and complications such as thrombus.
Clinical management of isolated FIUVV should follow standard established protocols, with good fetal outcomes expected. 2 Sonographic assessment, including careful Doppler evaluation, should be performed biweekly to search for thrombus and hydrops and to monitor varix size. 2 Delivery is recommended if thrombus is identified. This case reinforces the importance of careful and complete fetal evaluation on surveillance sonography.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.