
Abstract
Inferior vena cava (IVC) tumor thrombus in renal cell carcinoma is a rare entity that suggests heightened biologic behavior and a surgical challenge during the course of treatment. Tumor thrombus can extend from the renal vein to the right atrium. This cephalad extension is classified by four different levels. These levels determine which surgical approach is used, whether a thoracoabdominal incision is needed, and whether a patient needs to be placed in circulatory arrest. Complete surgical resection of the tumor is potentially the only curative treatment, although it supposes a challenge because of operative difficulty and the potential for massive bleeding or tumor pulmonary thromboembolism. IVC tumor thrombus presents with a few differentials that need to be assessed, including bland thrombus, primary IVC leiomyosarcoma, hepatocellular carcinoma, adrenal cortical carcinoma, primary lung carcinoma, and Wilms tumor. The importance of diagnosing IVC tumor thrombus secondary to renal cell carcinoma is demonstrated as well as a sonographic protocol for assessing IVC tumor thrombus.
Tumor thrombus is defined as intravascular metastases with thrombotic elements. It is a rare complication of cancers mainly seen in cases of renal cell carcinoma (RCC). The American Cancer Society estimates that about 63,990 new cases of kidney cancer (40,610 in men and 23,380 in women) will occur in 2017; about 14,400 people (9,470 men and 4,930 women) will die from this disease. 1 RCC can invade through the renal vein into the inferior vena cava (IVC) and can then extend intraluminally, with tumor thrombus formation occurring in 5% to 15% of all cases, whereas the tumor may extend up to the right cardiac chambers in 1% of cases. 2 Given the poor prognosis if these patients are untreated, the diagnosis of RCC with tumor thrombus invasion into the IVC necessitates expedient evaluation, preoperative optimization, and rapid coordination of a multidisciplinary team to prepare patients for surgical treatment. The incidence of perioperative complications depends on the cephalad extension of the IVC tumor thrombus. It is imperative that tumor thrombus is differentiated from bland thrombus. Bland thrombus is thrombus without neoplastic characteristics. Bland thrombus develops as a result of venous congestion and can be resolved after thrombolytic and anticoagulant therapy.
Case Report
A man in his fifth decade presented to the sonography department for evaluation of the IVC and the right renal vein. A renal sonogram was ordered as a follow-up to a recent computed tomography (CT) study, which showed echogenic material in the right renal vein and the IVC. The patient’s clinical history included RCC, congestive heart failure, stroke, severe protein-calorie malnutrition, hypertension, heart disease, coronary artery disease, tobacco use, arthritis, and anemia. He presented with macrohematuria, flank pain, and severe bilateral lower extremity edema. The sonographic examination was performed using a Philips iU-22 ultrasound system (Philips Ultrasound, Andover, MA) with a 5-1 MHz curved-array transducer. The left kidney (10.49 × 5.72 × 3.76 cm) revealed no abnormalities. The right kidney appeared to be enlarged (12.51 × 9.35 × 8.6 cm) and diffusely inhomogeneous with a possible mass within the renal vein (Figure 1). Gray-scale imaging demonstrated the IVC filled with echogenic material at the level of renal veins. The right renal vein appeared distended and filled with echogenic material (Figure 2). There was no evidence of extension of echogenic material into the left renal vein. Color Doppler showed absence of flow within the right renal vein (Figure 3). The echogenic material within the IVC and right renal vein was consistent with intraluminal thrombus. The IVC thrombus measured 8 × 4.97 × 2.8 cm (Figures 4 and 5). Color Doppler imaging revealed internal vascularity within the thrombus (Figure 6). The sonogram documented the thrombus within the IVC extending approximately 6 cm below the right atrium (Figure 7). The interpreting physician reported that there may have been some bland thrombus between the tumor thrombus and the right atrium within the IVC.
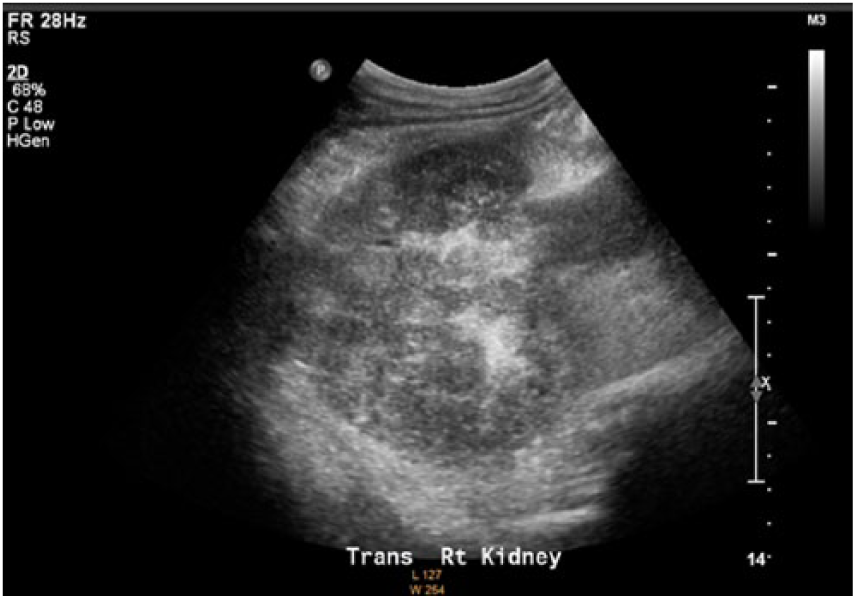
Transverse gray-scale image demonstrating heterogeneity of the right kidney with renal vein thrombus.
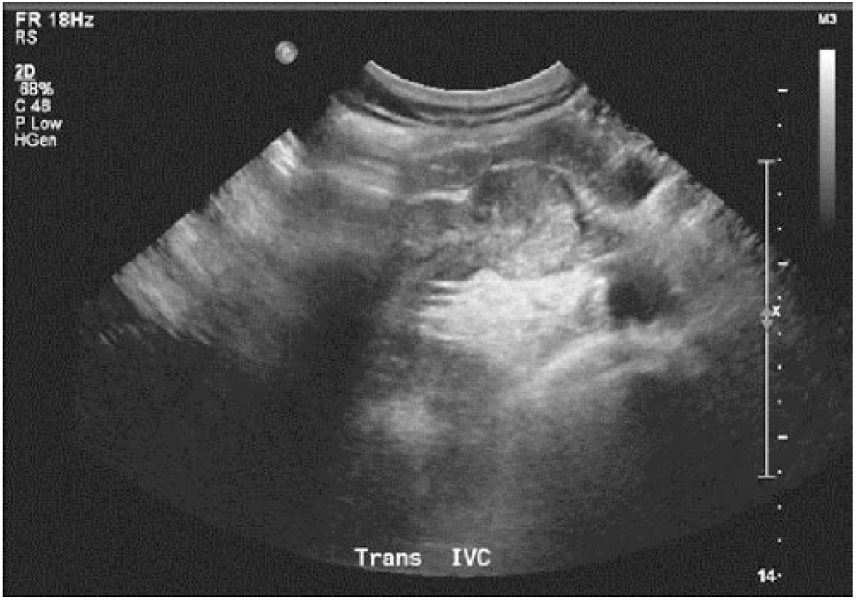
Transverse gray-scale image demonstrating the inferior vena cava filled with thrombus. The thrombus extends from the right renal vein, which is distended.
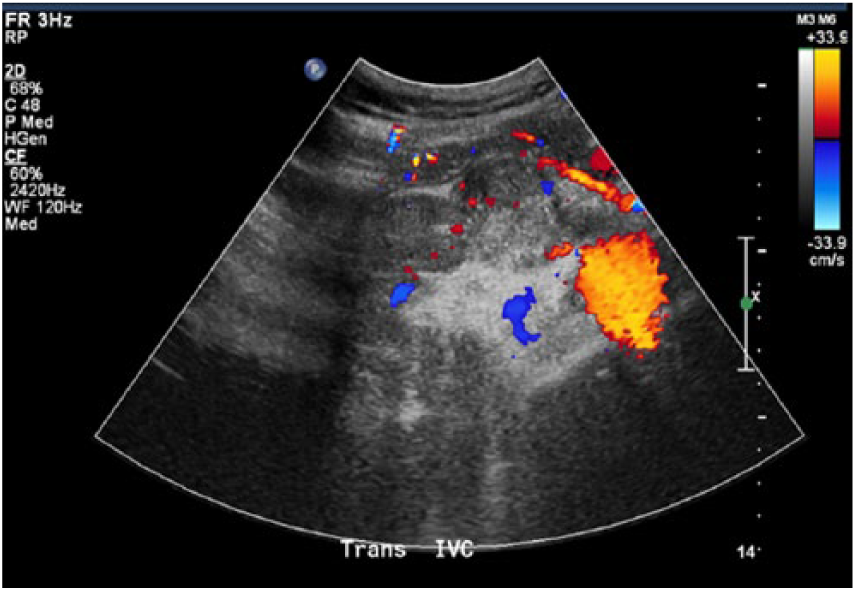
Transverse image of the inferior vena cava at the level of renal veins with color Doppler demonstrating the absence of flow in the right renal vein.
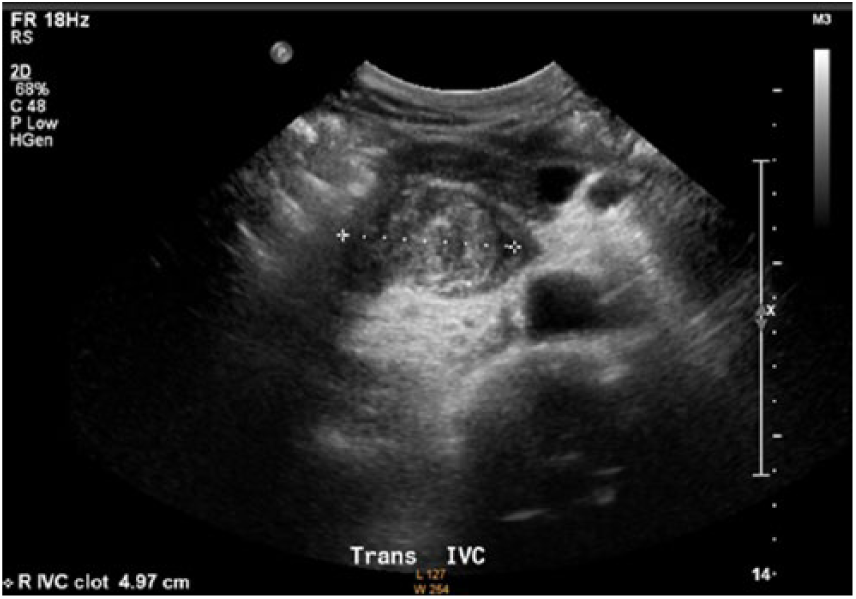
Transverse gray-scale image of inferior vena cava thrombus with measurement.
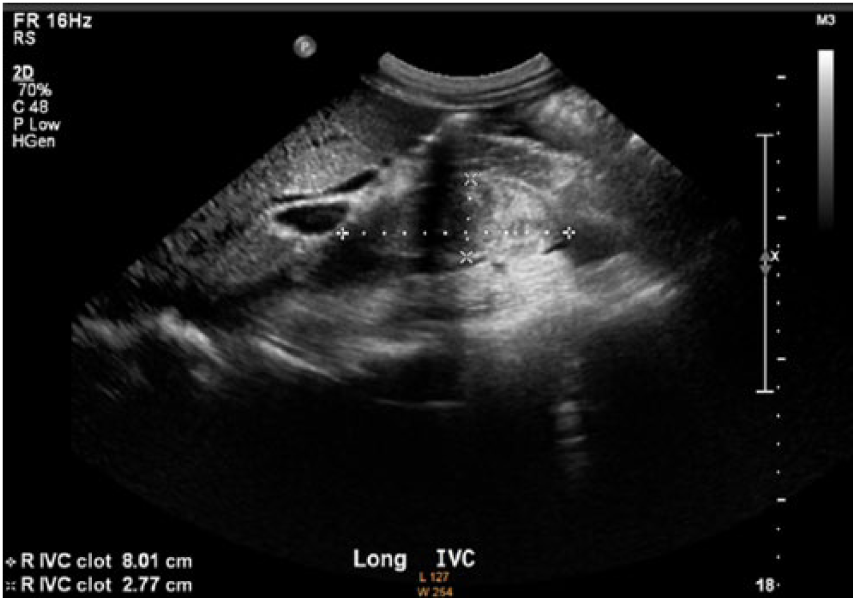
Longitudinal gray-scale image of inferior vena cava thrombus with length and anterior-posterior measurements.
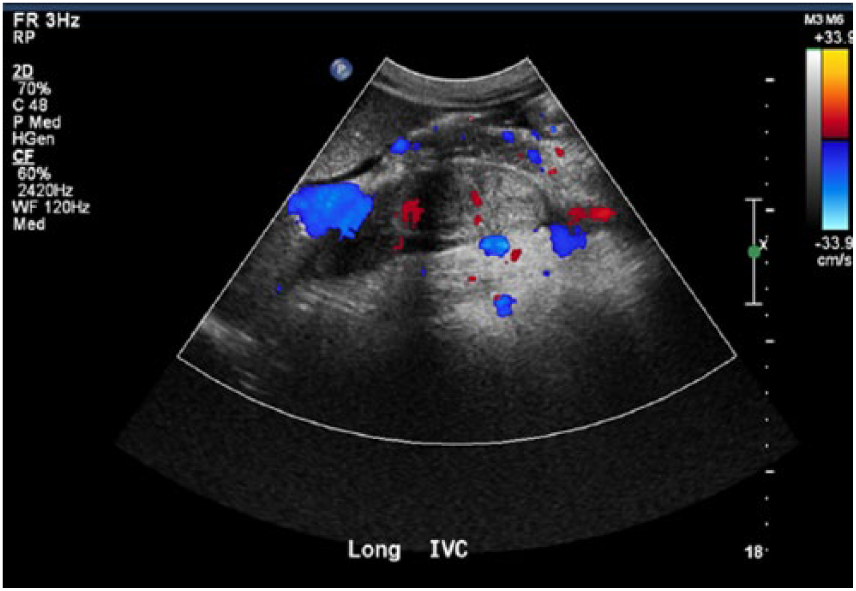
Longitudinal image of thrombus within inferior vena cava. Color Doppler reveals internal vascularity.
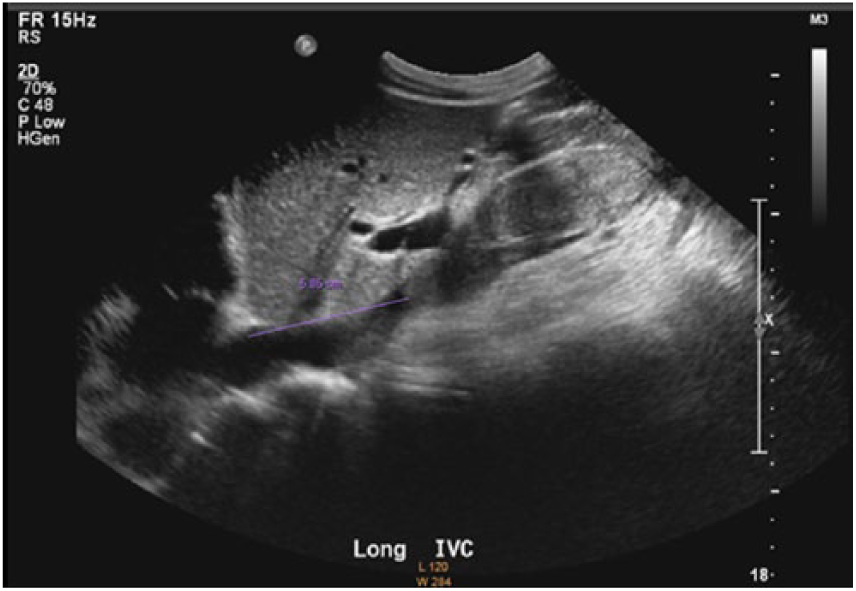
Longitudinal gray-scale sonographic image of inferior vena cava thrombus, which lies approximately 6 cm inferior to right atrium.
The patient was diagnosed with IVC tumor thrombus secondary to RCC. He underwent several surgeries, which included radical nephrectomy and thrombectomy. No further information is available because the patient is deceased.
Discussion
Tumor thrombus is a collective term for intravascular metastatic tumor deposit with thrombotic elements. Tumor thrombus is a rare complication of solid cancers, mainly seen in cases of RCC, Wilms tumor, testicular carcinoma, adrenal cortical carcinoma, and hepatocellular carcinoma. 3 RCC is the eighth most common malignancy affecting adults and accounts for between 3% and 4% of new cancer cases in the United States. 4 It is the seventh most common cancer in men and the ninth most common in women. 4 The disease has a 5:1 male predominance. 5 Clinical symptomatology may be quite nonspecific (e.g., anorexia, fatigue, weight loss, or fever of unknown origin). 6 Certain genetic conditions are associated with an increased incidence of RCC, including von Hippel-Lindau disease, hereditary papillary renal cancer, and, possibly, tuberous sclerosis. 7 Other suggested risk factors include cigarette smoking; obesity; diuretic use; exposure to petroleum products, chlorinated solvents, cadmium, lead, asbestos, and ionizing radiation; high-protein diets; hypertension; kidney transplantation; and HIV infection. 8 Histologic subtypes according to the Heidelberg classification include clear cell adenocarcinoma (80%), papillary (15%), chromophobe (5%), collecting duct (1%), and unclassified (4%).9–11
Extension of tumor into the renal veins has been reported in 20% to 35% of patients, and into the IVC in 4% to 10% of patients. 12 IVC thrombus is more common from right-side tumors because of the shorter renal vein on the right.13,14 Most patients with an IVC tumor thrombus are symptomatic at the time of presentation. Local tumor growth may cause symptoms such as flank pain and hematuria, and symptoms of fatigue, weight loss, or a paraneoplastic syndrome can be constitutional in nature. Paraneoplastic syndromes are rare disorders that are triggered by an altered immune system in response to a neoplasm. They are defined as clinical syndromes involving nonmetastatic systemic effects that accompany malignant disease. The symptoms may be endocrine, neuromuscular or musculoskeletal, cardiovascular, cutaneous, hematologic, gastrointestinal, renal, or miscellaneous in nature. The thrombus-related occlusion of the IVC may result in lower extremity edema, new onset of a varicocele, or, in the case of thrombus dislodgement, pulmonary embolus. On the other hand, symptoms directly attributable to the tumor thrombus may be absent even in the presence of total IVC occlusion, because venous collateralization occurs through the azygos and lumbar systems. 15
A number of classification systems are used for the macroscopic vascular involvement in RCC such as the Union Internationale Contre le Cancer and the American Joint Committee for Cancer Staging and End Results Reporting TNM staging classification as well as the Neves and Zincke system. The Mayo classification (Figure 8 and Table 1) 16 is commonly used and consists of four categories based on the extension of the thrombus. 17 Level I thrombus is limited to the renal vein or less than 2 cm within the IVC. Level II thrombus extends more than 2 cm within the IVC above the confluence of the renal vein and IVC but is still below the hepatic veins. Thrombus involving the intrahepatic IVC is level III. Level IV thrombus extends above the diaphragm or into the right atrium. The surgical approach strategy is based on the proper assessment of the level of the venous extension.
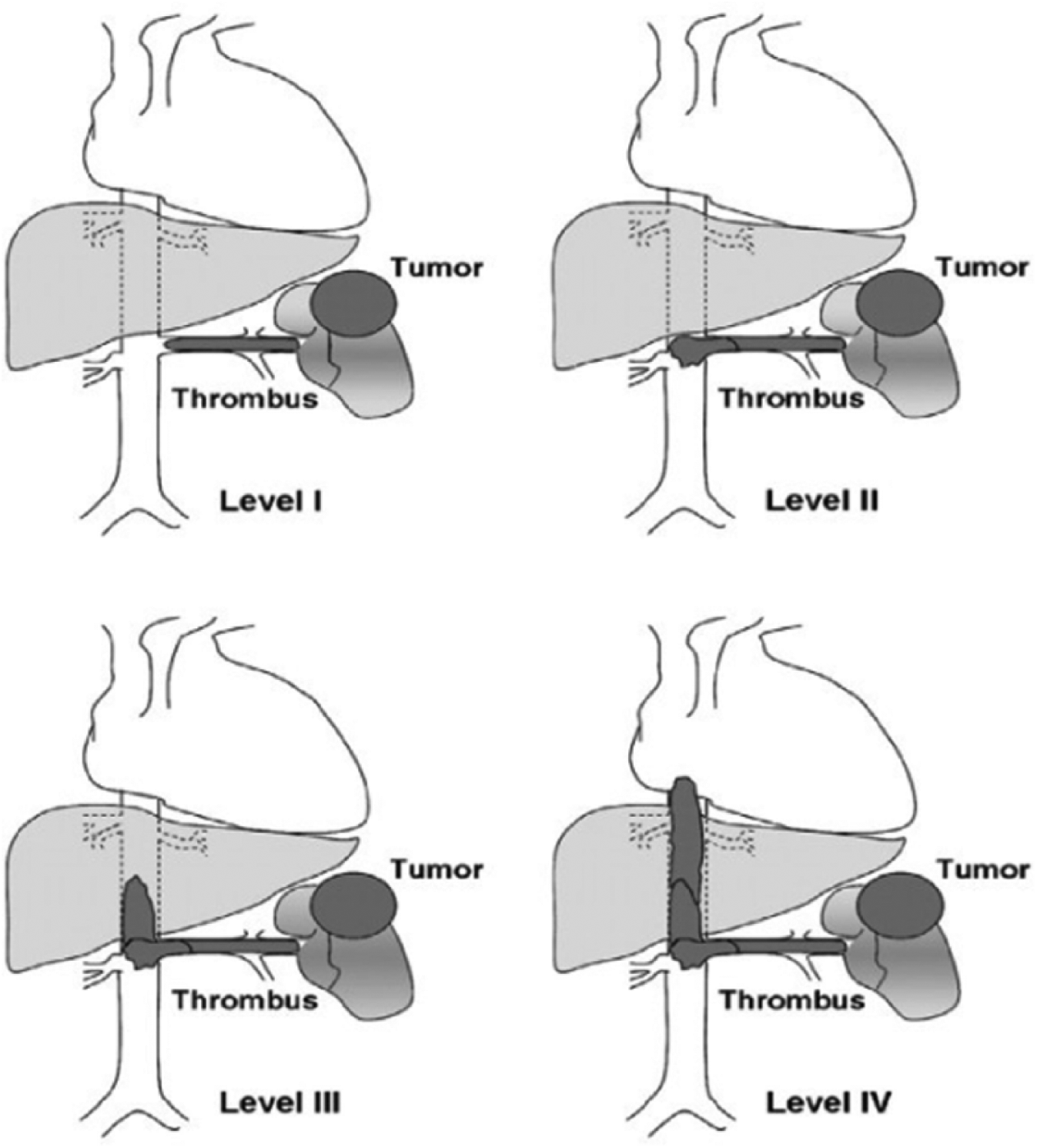
The Mayo classification of macroscopic venous invasion in renal cell carcinoma.
Mayo Classification of Macroscopic Venous Invasion in Renal Cell Carcinoma.
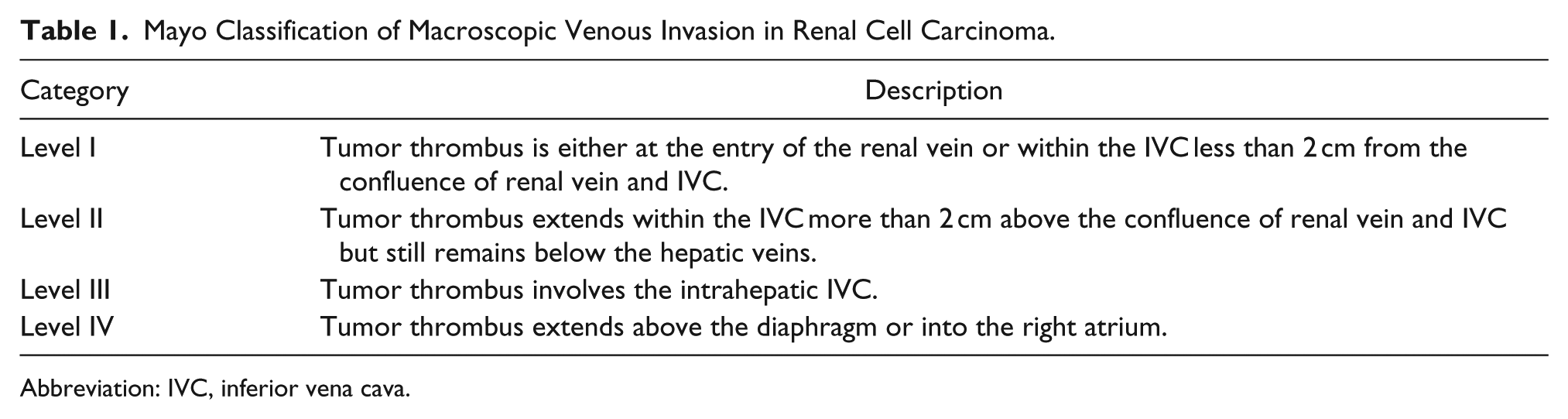
Abbreviation: IVC, inferior vena cava.
Although complete removal of the extension of the tumor thrombus into the IVC does not affect patient prognosis, nonremoval has been associated with poor survival rates. 18 Therapy for advanced cases complicated with IVC tumor thrombus requires a multidisciplinary approach including many physicians such as a urologist, an oncologist, and multiple surgeons. The basic therapy for RCC complicated with IVC tumor thrombus is radical nephrectomy combined with tumor thrombectomy. Also, the resection and reconstruction of the IVC and metastasectomy may be necessary. The incidence of perioperative complications depends on the cephalic expansion of the IVC tumor thrombus. Level I and II thrombi are easily resectable, with low complication rates by laparotomy alone. Level III or IV thrombi can be resected with extensive hepatic mobilization or the use of cardiopulmonary bypass. However, cardiopulmonary bypass prolongs the length of the operation and may result in significant blood loss, ischemic lesions in the central nervous system and other organs, and postoperative coagulopathy. 19 Five-year survival rates following surgery have been reported to range from 32% to 64%. 20 Reported mortality rates for radical nephrectomy with concomitant IVC thrombectomy range between 5% and 12.5% for higher level thrombus, depending on patient comorbidities and tumor characteristics. 21
Traditionally, venacavography was the gold standard for detection of tumor thrombi. However, today it is rarely used because it is unable to demonstrate caval wall invasion by the neoplastic process and is not additive to sonography, CT, and magnetic resonance imaging (MRI). It also has the associated high risk of contrast-induced renal injury. Current CT techniques have reported sensitivities and specificities for detecting renal vein thrombus of 85% and 98%, respectively. 22 Color Doppler sonography has reported sensitivities and specificities for detecting thrombus in the renal veins of 75% and 96%, respectively, with 100% accuracy for detection of thrombus in the IVC. 23 MRI has similar reported sensitivity and specificity for detecting thrombus in the renal vein of 86% to 94% and 75% to 100%, respectively, as well as 100% accuracy for detecting IVC thrombus.24,25 Sonography has several advantages over other imaging techniques. It is able to present cross-sectional anatomy without radiation in a noninvasive fashion. It is relatively inexpensive compared with other studies and requires minimal patient preparation, producing minor patient discomfort. Sonography is able to delineate the details of a tumor thrombus, judge the presence of neoplastic vascularity, and find the evidence of tumor extension. However, sonography has its limitations. Its accuracy and sensitivity in detecting tumor thrombi and primary tumors strongly rely on the skills and experience of the sonographer, the position of the thrombus, and the patient’s health status. Artifactual shadows from bones and bowel can interfere with sonographic exploration, potentially even preventing imaging of the area in question. CT, MRI, and other imaging techniques can compensate for the shortcomings of sonography by providing images in areas that are difficult to assess with sonography.
A review of the current literature demonstrated no published protocol for sonographic evaluation of IVC tumor thrombus secondary to RCC. Therefore, sonographers should follow a standard renal or renal Doppler examination, depending on institutional protocol. This should include gray-scale, color Doppler, and pulse wave spectral Doppler evaluation, taking care to adjust gain and scale settings as needed and including all appropriate views, resistive indices, and velocity measurements. Also, a thorough investigation of the IVC must be performed and documented. When an IVC mass is evaluated, it is important to differentiate between bland thrombus and tumor thrombus because the treatment for both is radically different. A chart comparing normal, bland, and tumor thrombus sonographic findings can be found in Table 2. Bland thrombus is a major cause of obstruction of the IVC. 26 Often, because of the superior extension of idiopathic thrombophlebitis in the lower extremities or pelvis, bland thrombus can also be secondary to more generalized conditions such as dehydration, sepsis, localized inflammation, pelvic inflammatory disease, coagulopathy, congestive heart failure, immobility, trauma (direct or indirect), or severe exertion. Iatrogenic thrombosis may be due to surgery in the lower extremities or to direct caval manipulation. Conversely, there are studies that have recognized cancers as the cause of bland thrombus formation. Thrombosis was identified as a complication of cancer by Trousseau in 1865, and the combination of the two conditions is still often called Trousseau’s syndrome. Arterial and, more common, venous thrombosis is a frequent complication of cancer and sometimes a harbinger of occult cancer. Moreover, the use of new and aggressive therapy for cancer increases the risk of thrombosis. 27 Differentiation of a tumor thrombus from a bland thrombus is difficult simply on the basis of morphologic characteristics, as they are either homogeneous or heterogeneous and show all types of echogenicity. Both may or may not result in dilatation of the vascular lumen, so vessel dilatation does not improve specificity. 28 The presence of invasion of the vessel wall strongly suggests a tumor thrombus. 28 Tumor thrombus will appear continuous with the primary tumor. In contrast, a bland thrombus merely extends along the vascular lumen without invasive phenomena. By combining color Doppler flow imaging with pulsed wave Doppler imaging, the sonographer can discern the neoplastic vascularity of tumor thrombi to differentiate a tumor thrombus from a bland thrombus or judge the occlusion and degree of stenosis of the involved vessels. The relationship between a tumor thrombus and the involved vessels such as infiltration or adherence to the vascular wall can be displayed clearly. The “tracing” technique is crucial in exploring vessels. The sonographer must trace a tumor thrombus along the involved vessels to find the origin and extension. The sonographer positions one caliper at the most cephalad point of tumor thrombus and then manually draws, freehand, the boundary around the tumor thrombus, including the most caudal edge (Figure 9). Fully tracing out the thrombus is an important procedure because the findings will provide useful information for further workup and clinical treatment. 28 Another crucial step in evaluating IVC tumor thrombus is estimating the level of cephalad extension. The sonographer must document any involvement of renal veins, hepatic veins, and the right atrium.
Protocol and Sonographic Appearance of Vascularity in Cases of Renal Cell Carcinoma.
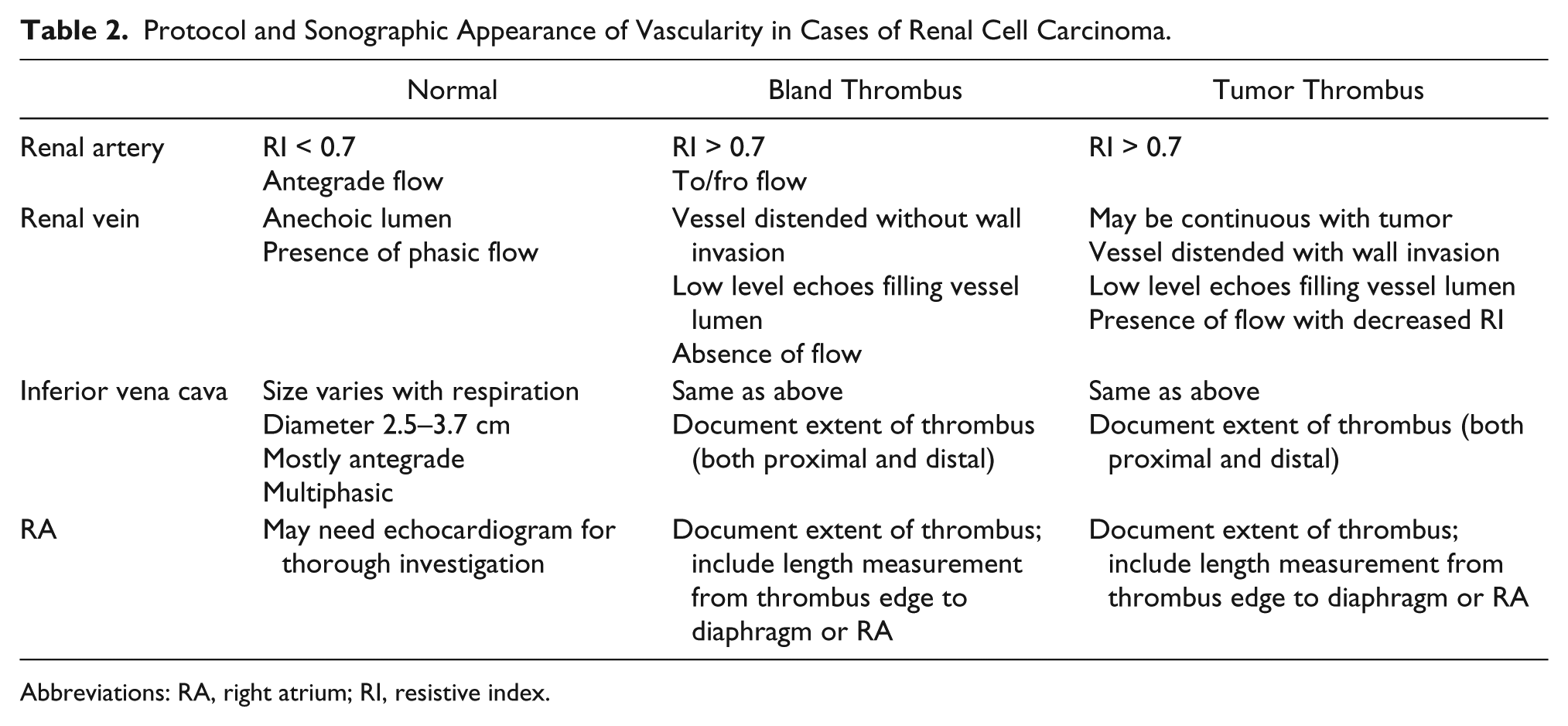
Abbreviations: RA, right atrium; RI, resistive index.
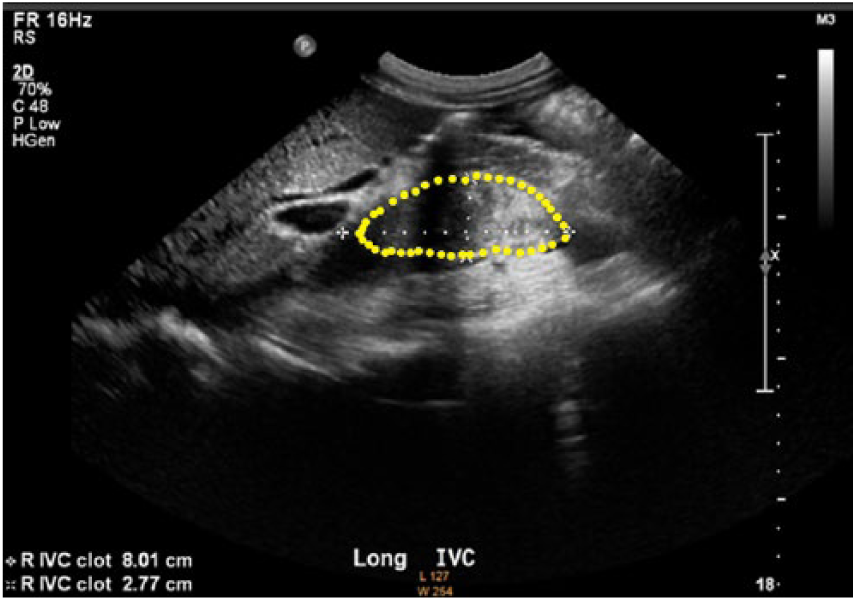
Example of tumor thrombus tracing.
Differential diagnoses include primary IVC leiomyosarcoma, hepatocellular carcinoma, adrenal cortical carcinoma, Wilms tumor, primary lung carcinoma, testicular carcinoma, and bland thrombus. Leiomyosarcoma is the most common primary malignancy involving the IVC. 29 It arises from the smooth muscle cells in the vessel wall. As of 2006, fewer than 300 cases had been reported in the medical literature. 30 Seventy-four percent of cases of IVC leiomyosarcoma occur in women, and women in their fourth through sixth decades are the most frequently affected. 31 Invasion into and thrombosis of the portal venous system are typical in patients with hepatocellular carcinoma, but invasion into hepatic veins and the IVC occurs in 4.0% to 5.9% of patients. 32 Right atrial involvement is also possible because of the right atrium’s proximity to the hepatic venous confluence. Occlusion of the IVC and hepatic veins may lead to Budd-Chiari syndrome, and patients may have the classic triad of ascites, abdominal pain, and hepatomegaly at presentation. Adrenal cortical carcinoma is a rare malignancy, with a reported prevalence of 0.5 to 2 cases per million persons. 33 Adrenal cortical carcinoma may develop at any age, but there is a bimodal age distribution during the first and the fourth to fifth decades of life. 33 Sixty-two percent of adrenal cortical carcinoma cases involve functional tumors and may lead to Cushing syndrome, virilization, or feminization. 33 Intravascular extension into the IVC may be seen in up to 30% of cases and is more common in right-side tumors and tumors that are larger than 9 cm. 34 Wilms tumor is the most common renal tumor in children and involves IVC invasion in 4% to 8% of cases. 35 Tumor thrombus is a rare complication of primary lung carcinoma. 3 Adrenal gland is one of the common sites of metastasis from primary lung cancer. 3 Adrenal metastases are usually unilateral. 3 Bilateral adrenal metastases are seen in 10% of all lung cancer patients. 3 The adrenal metastasis may lead to the formation of tumor thrombus in the adrenal vein, which may further extend to the IVC. Involvement of the IVC by a testicular tumor is a rare event. Two autopsy series of patients with testicular germ cell tumors have suggested IVC involvement in 3% and 11% of patients. 36 Dusaud et al. reviewed the CT scans of 650 patients with testicular cancer and found only four cases of IVC invasion among 397 patients with retroperitoneal disease. 36 The IVC involvement occurs because of the spread of the tumor by direct invasion of the spermatic vein and then of the vena cava. That explains why IVC invasion more frequently occurs with right-side tumors; it is because of the direct insertion of the right gonadal vein into the IVC. As stated previously, bland thrombus is the leading cause of IVC obstruction, which places the patient at high risk for pulmonary embolism. Risk factors for thrombus formation include a hypercoagulable state, malignancy, venous stasis, focal compression, and IVC filters. Bland thrombus in the IVC may be isolated but most often extends from pelvic and lower extremity deep vein thrombosis.
Conclusion
An unusual hallmark of RCC is the biological predisposition for vascular invasion with extension of tumor thrombus into the IVC. The natural history of untreated RCC with IVC tumor thrombus is poor. The level of tumor thrombus within the IVC determines which surgical approach to the primary tumor and thrombus is used, whether a thoracoabdominal incision is needed, and whether a patient needs to be placed in circulatory arrest. Therefore, it is imperative that sonographers first differentiate between tumor thrombus and bland thrombus. Neovascularity within the thrombus is specific to tumor thrombus. Second, sonographers must correctly detect the extent of any involvement of renal and hepatic veins, the IVC, and the right atrium.
Footnotes
Acknowledgements
The author acknowledges the help and support of Jeanette Rogerson, MS, RDMS, Pamela Crawford, RDMS, RVT, RT, and Lynn Schluns, BS, RDMS, RVT, in the preparation of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.