
Abstract
Traditional peripheral arterial waveforms have been inconsistently defined and classified. This investigation compares waveform categorization scores from two comparable groups of sonography participants. Group 1 interpreted continuous-wave (CW) and pulsed-wave (PW) Doppler waveforms based on standard text definitions. Group 2 performed the same task following 10 minutes of detailed waveform characterization instructions with accompanying illustrations. Each group comprised 157 participants with an equal number of students, registered sonographers, and physicians. Significant differences were noted between groups 1 and 2 for 60% of CW waveforms and 33% of PW waveforms (P < .05). In group 2, American Registry for Diagnostic Sonography (ARDMS)–registered sonographers had significantly higher CW scores than students and physicians (P < .0001); registered vascular technologists and multispecialty ARDMS-certified sonographers had significantly higher PW scores than students, Registered Diagnostic Medical Sonographer (RDMS)–certified sonographers, and physicians (P = .0086 and P = .0295, respectively). This study emphasizes the contribution of sonographers in arterial Doppler waveform categorization and underscores the need for standardization and education.
Doppler instruments used in combination with a recording device provide a graphic representation of blood flow through arterial vessels. Doppler waveform analysis is fundamental to the evaluation of peripheral arterial disease and is traditionally defined as either normal or abnormal.1–4 Normal peripheral arterial waveforms at rest are multiphasic, with high forward flow during systole, flow reversal in early diastole, and usually a smaller forward flow component in late diastole. The loss of diastolic flow reversal is a widely accepted characteristic for differentiating normal from diseased peripheral arteries.1–4
One of the first concepts taught to sonography students when learning Doppler analysis of peripheral arterial disease is waveform characterization and the utilization of triphasic, biphasic, and monophasic waveform terminology. Although these traditional waveform descriptors have been in use for more than four decades, surveys and a literature review indicate major inconsistencies regarding waveform definitions and categorization.5,6 The purpose of this investigation is to evaluate whether arterial waveform classification using traditional waveform descriptors improves following detailed instructions and accompanying illustrations.
Methods
Thirty Doppler waveforms (15 continuous wave [CW] and 15 pulsed wave [PW]) were obtained from previous noninvasive peripheral arterial evaluations. The CW and PW waveform groups consisted of 10 high-resistive, multiphasic waveforms with diastolic flow reversal; 4 low-resistive waveforms with pandiastolic forward flow and varying levels of peripheral (outflow) resistance; and 2 “other” waveforms—a CW common femoral artery waveform with significant venous interference and a PW waveform within the neck of a femoral artery pseudoaneurysm.
From February 2007 through September 2009, group 1 or group 2 waveform presentations were presented at multiple sonography symposiums and educational conferences. Participants were verbally recruited from audience members of local, regional, and national sonography symposiums held in the Midwest and eastern United States and requested to defer completing an answer sheet if they had previously participated in either of the two waveform presentations elsewhere. The answer sheet contained check-off locations for interpreting all 30 waveforms as well as the following demographic data:
Highest educational degree
Medical or sonography-related certification(s)
Number of years of sonography experience
Participants were divided into two primary groups; each primary group comprised the following five subgroups:
Student—sonography students; little or no clinical sonography experience
Registered Vascular Technologist (RVT)—American Registry for Diagnostic Sonography (ARDMS), registered vascular technologists
Registered Diagnostic Medical Sonographer (RDMS)—ARDMS-registered diagnostic medical sonographers
Multispecialty ARDMS—RVT, RDMS, or Registered Diagnostic Cardiac Sonographer (RDCS)
Physician—doctor of medicine (MD) or doctor of osteopathic medicine (DO)
An equal distribution of student, physician, and certified sonographers was contained within both groups. Participants were reminded that they could only be involved and interpret one (group 1 or group 2) waveform presentation survey.
Group 1 participants were instructed to classify each of the CW and PW waveforms within a 15-second time frame using one of the following traditional waveform descriptors:
Triphasic: three phases—systolic forward flow, flow reversal, and a second forward flow component
Biphasic: two phases—one forward flow and one reverse component
Monophasic: single phase—forward flow with no reverse flow component
Other
The first three descriptors are similar to those recommended by the Society for Vascular Ultrasound (SVU) 7 ; the fourth was used to categorize waveforms with morphology that was not considered triphasic, biphasic, or monophasic or considered unknown.
Group 2 participants were given an identical answer sheet, demographic instructions, CW and PW waveform presentation, and 15-second interpretation time constraint. However, prior to initiating the interpretation presentation, they were also given 10 minutes of waveform classification instructions, including accompanying illustrations directed at clarifying the following waveform descriptions:
Triphasic: three phases—systolic forward flow, early diastolic flow reversal, and late diastolic forward flow
Biphasic: (1) high resistive—systolic forward flow with diastolic flow reversal and (2) low resistive—sharp systolic acceleration/deceleration with pandiastolic forward flow
Participants were told that waveforms they considered biphasic, whether high or low resistive, should only be interpreted as biphasic.
Monophasic: one phase—systolic forward flow, no flow reversal, suggesting significant obstruction proximally
“Other”: waveforms with morphology that was not considered triphasic, biphasic, or monophasic or considered unknown
Correct responses were based on waveform descriptors used in the originating noninvasive evaluation. Physicians and sonographers with 16 or more years of sonography experience were designated as reference comparisons for the certification and experience analyses, respectively. A certification subgroup analysis was performed on four low-resistive waveforms with pandiastolic flow: CW 21, CW 25, PW 12, and PW 28 (Figure 1).
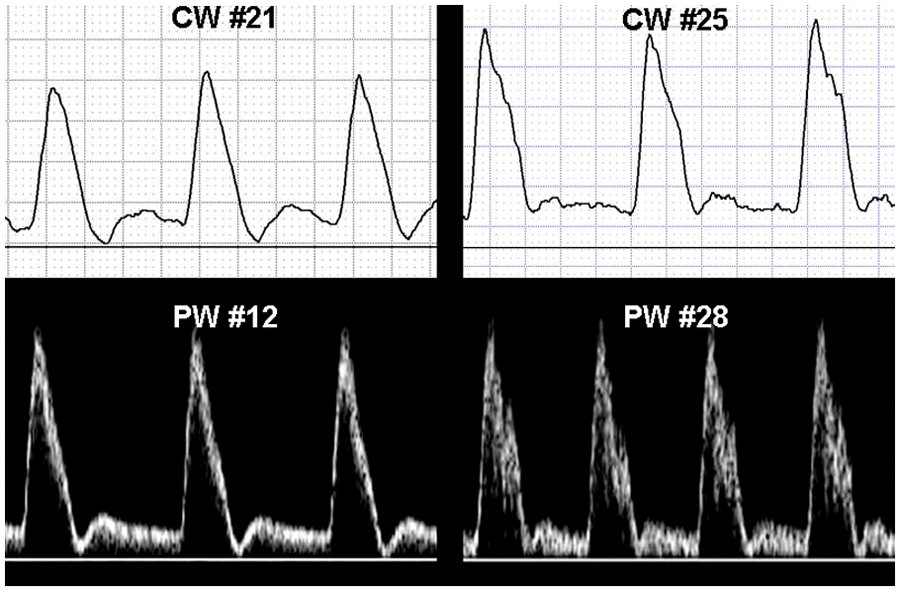
Four low-resistive waveforms with pandiastolic flow were used as part of a subgroup analysis.
SAS version 9.1 statistical software (SAS Institute, Cary, North Carolina) was used to perform analysis of variance (ANOVA) t test and chi-square analyses. For group 1 and group 2 scores by certification and sonography experience, a P value less than .05 was used to define statistical significance; less than .01 was used to define statistical significance for the low-resistive waveform subgroup analyses.
Results
There were 314 participants, with 157 in each primary group (groups 1 and 2). Each primary group had the following subgroup composition:
29 Students
37 RVT sonographers
26 RDMS sonographers
39 Multispecialty ARDMS sonographers
26 Physicians
Twenty-nine participants were excluded: 12 who could not be categorized into one of the five participant subgroups and 17 who failed to complete all assigned waveform interpretations.
No significant group 1 and group 2 differences were noted for educational degree, medical or sonography certification, and number of years of sonography experience (P = .0832).
Group Analysis
The designated “correct” CW and PW waveform responses based from previous noninvasive peripheral arterial evaluations and the total number of triphasic, biphasic, monophasic, and “other” responses by all participants are presented in Figure 2. Significant differences were noted between group 1 and group 2 for 60% (9/15) of CW waveforms and 33% (5/15) of PW waveforms (P < .05).
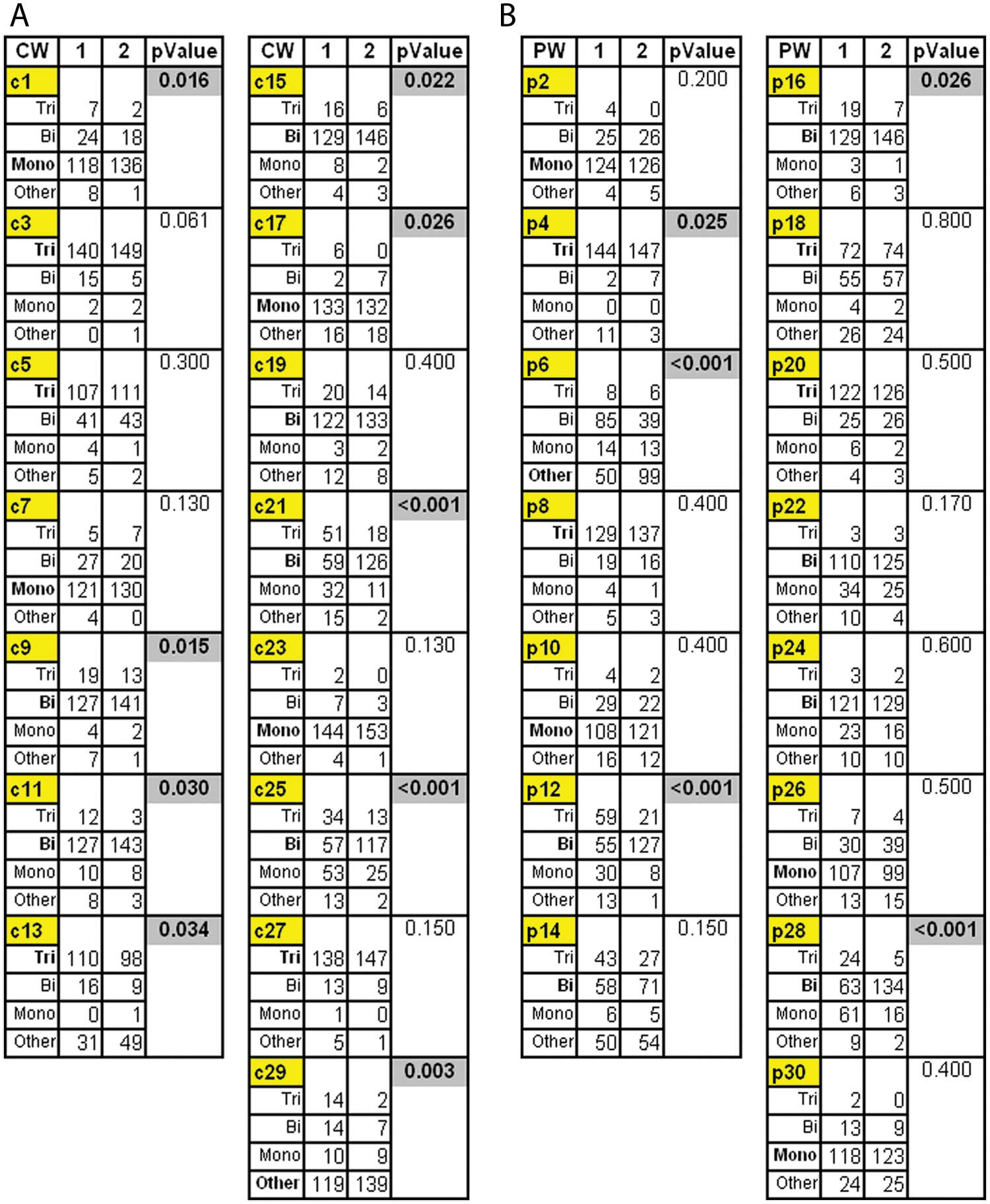
(A) Participant responses to continuous-wave and (B) pulsed-wave Doppler waveforms demonstrate difference in response by group. Correct answer is in bold.
Of the CW waveforms with nonsignificant changes, 67% (4/6) were defined as triphasic or biphasic and demonstrated diastolic flow reversal; 60% (6/10) of PW waveforms with nonsignificant changes were defined as triphasic or biphasic and displayed diastolic flow reversal.
Detailed group 2 waveform instructions with accompanying illustrations also resulted in a decrease in incorrect responses within all waveform classification categories: triphasic, 134% (362 to 155); biphasic, 22% (442 to 362); monophasic, 105% (312 to 152); and other, 30% (333 to 256).
Certification Analysis
Analysis of CW and PW scores by certification is presented in Figure 3. Waveform scores were significantly dissimilar based on certification. With physicians as the designated reference standard, group 2 had significantly higher CW and PW waveform scores than group 1 (P < .0001 and P = .0157, respectively).
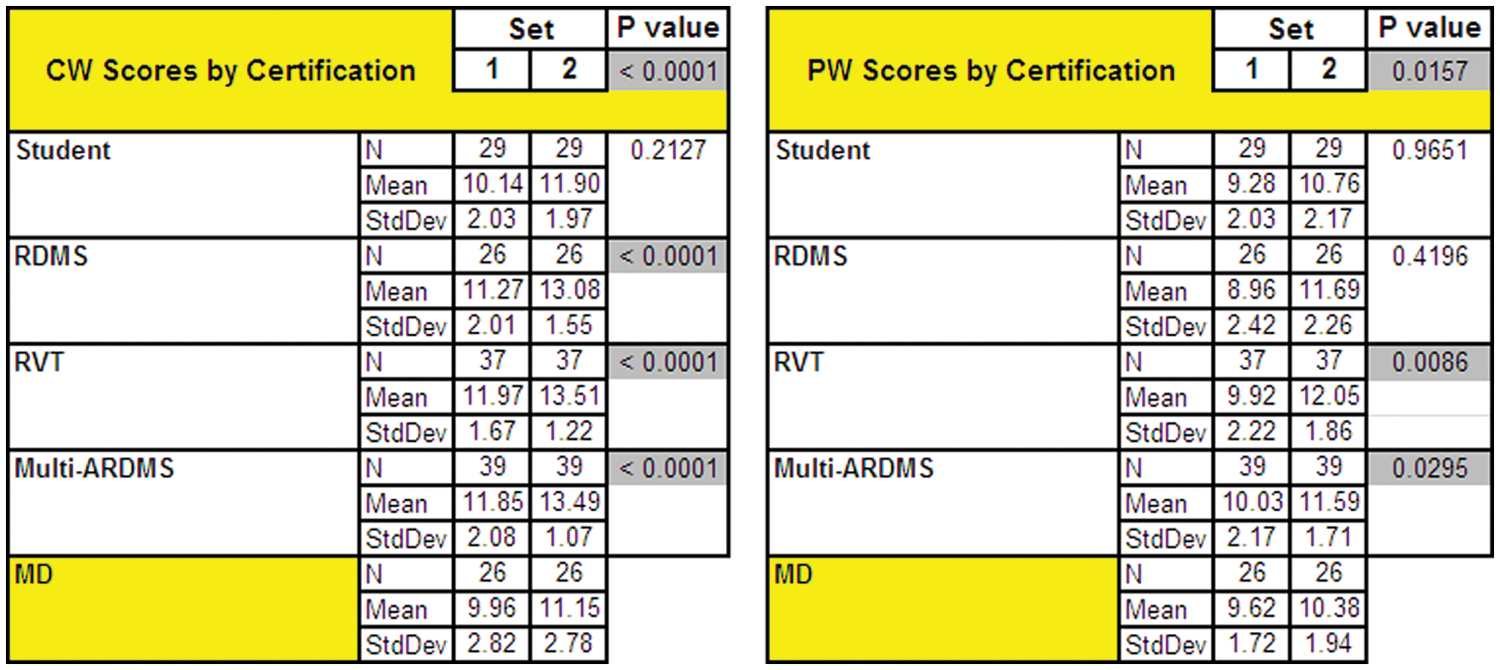
Analyzing waveform scores by certification demonstrates significant differences between groups.
Group 2 (RDMS, RVT, and multi-ARDMS) had significantly higher CW scores (P < .0001), and RVT and multispecialty ARDMS-certified sonographers had significantly higher PW scores (P = .0086 and P = .0295, respectively).
A certification subgroup analysis of low-resistive waveforms is presented in Figure 4. Group 2 scored significantly higher scores than group 1 for the following waveforms and certification categories:
CW 21: RVT, RDMS, and students (P < .01)
CW 25: Multi-ARDMS, RVT, and RDMS (P < .01)
PW 12: Multi-ARDMS, RVT, RDMS, and students (P < .01)
PW 28: Multi-ARDMS, RVT, RDMS, and students (P < .01)
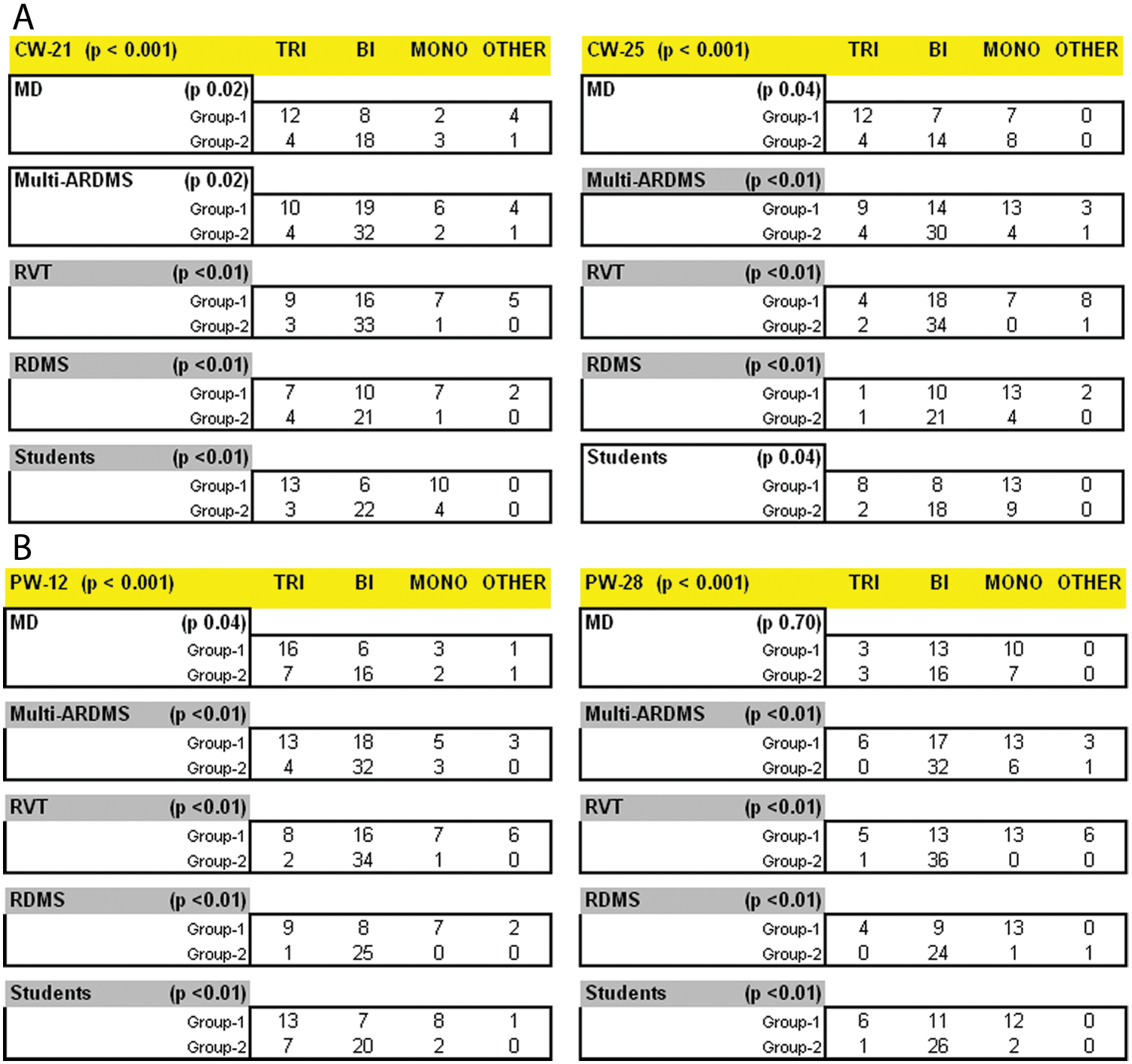
(A) Results of subgroup analysis of specific continuous-wave and (B) pulsed-wave Doppler waveforms stratified by certification.
Group 2 physician scores were not significantly higher than group 1 in this subgroup analysis.
Experience Analysis
Average number of years’ experience in the sonography profession was 11.1 years in group 1 (range, 0–32 years) and 11.4 years in group 2 (range, 0–37 years). Analysis of CW and PW scores by years of sonography experience is presented in Figure 5.
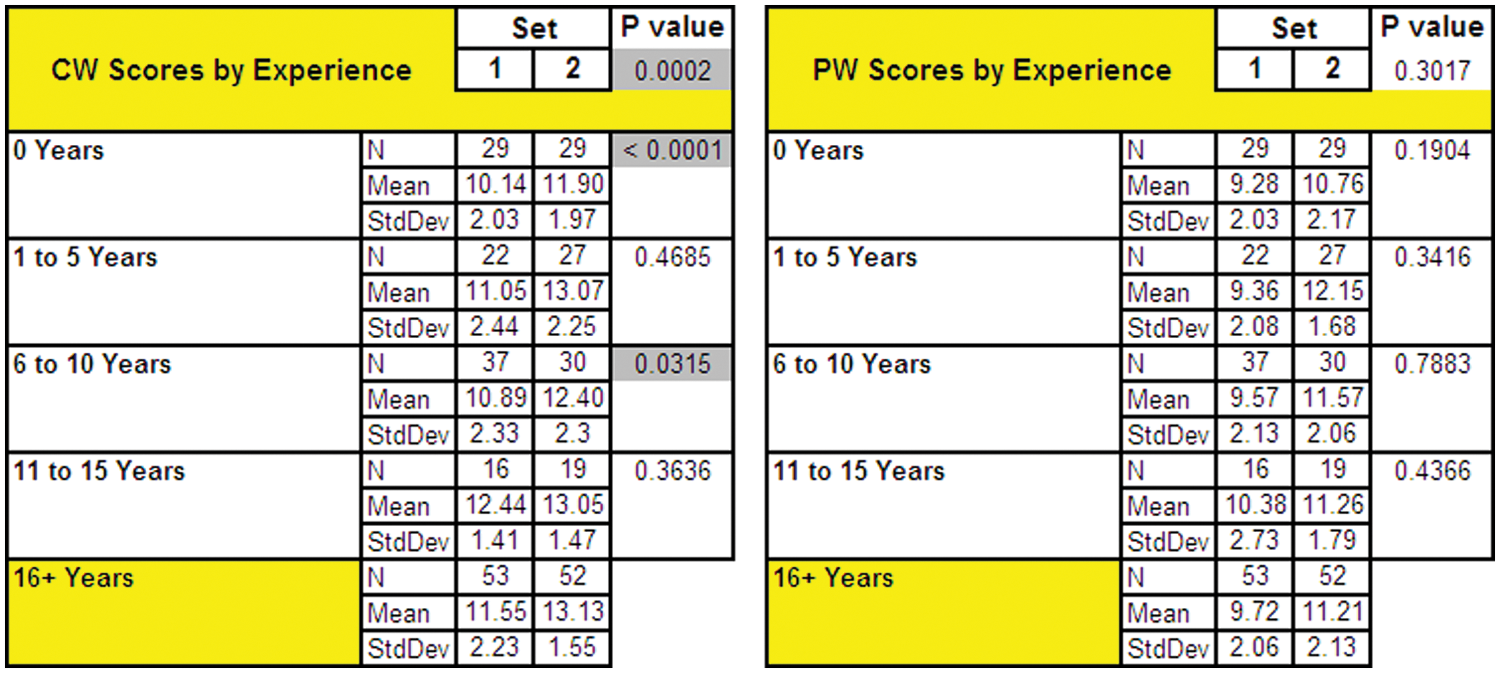
Continuous-wave Doppler waveform scores were affected by years of experience in the sonography profession; differences in scoring the pulsed-wave waveforms showed no significance.
With 16 or more years of experience as the designated reference standard, group 2 had higher CW Doppler waveform scores than group 1 (P = .0002); group 2 students and participants with 6 to 10 years’ experience had significantly higher scores than their group 1 counterparts (P < .0001 and P = .315, respectively). Years of sonography experience, however, had no significant impact on PW Doppler waveform scores (P = .3017).
Discussion
Accurate evaluation of Doppler waveforms is an essential component of recognizing peripheral arterial disease. Historically, three waveform descriptors—triphasic, biphasic, and monophasic— were developed for CW Doppler analysis of arterial blood flow in the upper and lower extremities. We have previously demonstrated that these terms have multiple meanings that are inconsistently applied within the sonography profession.5,6
This extended survey adds further support for the confusion surrounding waveform categorization and, more important, offers insight for addressing this issue. Sonography professionals who were provided specific waveform classification instructions with accompanying illustrations correctly matched previous arterial waveform interpretations at a significantly higher rate than a similar participant cohort who were provided standard text definitions without illustrations. Waveform education appears to be a key element for explaining the substantial improvements made by group 2.
Peripheral arterial waveform standardization, or rather the lack of it, is best explained historically. Triphasic has been most often defined as having three phases. This term, however, frequently has been referred to as multiphasic and also attributed to a waveform with two phases. 8 Biphasic is commonly described as having two phases, including diastolic flow reversal, yet a review of literature notes that this term is used about half the time and defined even less. 6
Normal waveform appearance can be altered if there is low impedance in the distal vascular bed (e.g., during reactive hyperemia or after exercise in patients without any evidence of arterial disease). In these instances, the waveform will display pandiastolic forward flow throughout diastole; waveforms with these characteristics have also been defined as biphasic.8,9 Waveforms without diastolic flow reversal and exhibiting pandiastolic forward flow have been used to classify aortoiliac disease. Paradoxically, they have also been referenced as sharp monophasic and used to help differentiate patients with significant superficial femoral artery (SFA) obstructions. 10 Biphasic, therefore, can be used to describe both a normal and an abnormal waveform.
Monophasic has traditionally been used to characterize waveforms with impaired systolic acceleration that suggests a significant obstruction proximal to the point of Doppler insonation. Sonography educators, however, also have used this term as a surrogate for the low impedance state found in normal patients following exercise.11–13
Triphasic is the most universally defined of the three classical waveform descriptors. Inherent to its definition is flow reversal during early diastole. However, more than a quarter of group 1 and nearly 20% of group 2 participants indicated by their categorization that flow reversal can occur above the zero flow baseline. Assuming triphasic is perceived without flow reversal and can be described as biphasic or monophasic, then a lack of waveform standards is undermining our understanding of basic Doppler principles.
Although the clinical impact of ambiguous waveform definitions is arguable, the potential for miscommunication is more probable than questionable. Monophasic is most often associated with an arterial obstruction. Even in normal patients without arterial disease, a preexercise triphasic waveform will become unidirectional with pandiastolic forward flow following an adequate period of exercise. If all waveforms with a unidirectional flow are labeled monophasic, there is the potential for confusing vasodilation and normal hyperemic responses with abnormal flow and significant arterial disease.
The analysis of classification scores based on sonography certification offers insight as to the consequences of a profession devoid of waveform standards. With the exception of students, sonographers had significantly higher waveform scores than did physicians. The lack of clinical maturity is a plausible explanation for the performance by students but contradicts the performance of physicians. If, however, waveform categorization is sonographer driven, then the interpretation responses by physicians is not so unexpected and might even be anticipated.
A number of publications appear to validate this supposition. In investigations of aortoiliac and femoropopliteal disease, waveform analyses have been assigned to a vascular technologist. 14 Over the past 20 years, other investigations corroborate this level of sonographer involvement.8,10,15 If sonographers are largely responsible for waveform categorization, then a lack of standards for waveform classification will have an even greater impact in the future.
The educational pathway of vascular sonographers has undergone enormous change over the past 20 years. In the past, sonography instruction was carried out primarily in the workplace, which may explain why more experienced sonographers in this study performed better in CW but not in PW waveform analysis. In today’s duplex sonography-dominated profession, physiological testing is the lesser used modality. In the second decade of the 21st century, the average vascular sonographer is more than 40 years old; most of these sonographers have three or more years of on-the-job (OJT) training.16,17 Today, OJT is no longer an option for obtaining ARDMS certification; the primary sonographer pathway is formal sonography training in approved degreed or certification programs. With a greater reliance on formal sonography education and less clinical experience, it is crucial that sonography definitions, protocols, and practices be standardized.
The lack of sonography standards could also affect patient care. Patients are commonly referred to sonography laboratories without a complete history and physical examination, resulting in an increasing number of inappropriate examinations. 18 Furthermore, a recommendation to the American College of Physicians proposes that sonography equipment should be integrated into primary care offices throughout the county. 19 Without standardization, if triphasic can be perceived without flow reversal and biphasic can be used interchangeably with monophasic, primary care physicians may be likely to inappropriately refer a patient for additional testing based on incorrect classification of a Doppler waveform.
In conclusion, this study reaffirms the subjectivity of waveform characterization and suggests that education and standardization could help minimize this dilemma. Consequences of indecisive action include confusion at the sonography education level, continued misunderstanding of basic Doppler principles, and an increased likelihood of inappropriate sonography testing. Dr Robert Barnes, a leading pioneer of vascular sonography and Doppler waveform analysis, once stated that standardization was crucial to the advancement of the sonography profession. Confusion in characterizing peripheral arterial blood flow is a glaring reminder of how we have failed to act on that challenge. This study and previous research suggest sonographers would be the prime beneficiary of standardization because they are at the forefront of waveform classification. A consensus panel was recommended to address this subject. 6 Representatives of the Society of Diagnostic Medical Sonography (SDMS) and SVU may offer the best chance for addressing and resolving this issue.
Footnotes
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author received no financial support for the research, authorship, and/or publication of this article.