
Abstract
Vascular sonography combined with other modalities has established the diagnosis of Takayasu arteritis. This case presents an East Indian woman who presented with right upper extremity pain, coldness, and numbness. Sonography remained the basis of intervention evaluation.
Takayasu arteritis (TA) is rare inflammation of the artery walls (arteritis) of the aortic arch, great vessels, and their large and medium-sized branches that carry oxygenated blood from the heart to the upper body. This report describes the presentation, multimodality diagnosis, treatment, and follow-up of TA in an East Indian woman in her late 30s. This case serves to raise awareness among medical professionals about TA recognition and testing.
Case Report
The patient presented to the emergency department (ED) with right forearm paresthesia and numb, painful, cold right fingers that worsened over the previous week. Contrast angiography showed right subclavian artery occlusion and multiple lesions in the arteries of the upper extremities, neck, and great vessels, raising suspicion of TA.
Patient History
The patient was taking Synthroid for preexisting hypothyroidism and reported taking an antiplatet (Plavix), anticoagulant (aspirin), and a steroid (methylprednisone) at the ED for prophylactic treatment of blood clots and to reduce the suspected arteritis.
Physical Examination and Assessment
Vital signs were within normal limits, except for mildly low body temperature of 97.1°F. Brachial pressure was 118/60 mm Hg on the left and 112/52 mm Hg on the right. Pulses were nonpalpable in both wrists. No bruits were noted.
Sonographic Findings
Carotid Duplex
Carotid duplex taken at a cardiovascular surgeon’s office the following day investigated the lesions and found nonatherosclerotic circumferential thickening of artery walls, as well as color-flow disturbance in the common carotid arteries (CCAs) (Figure 1).
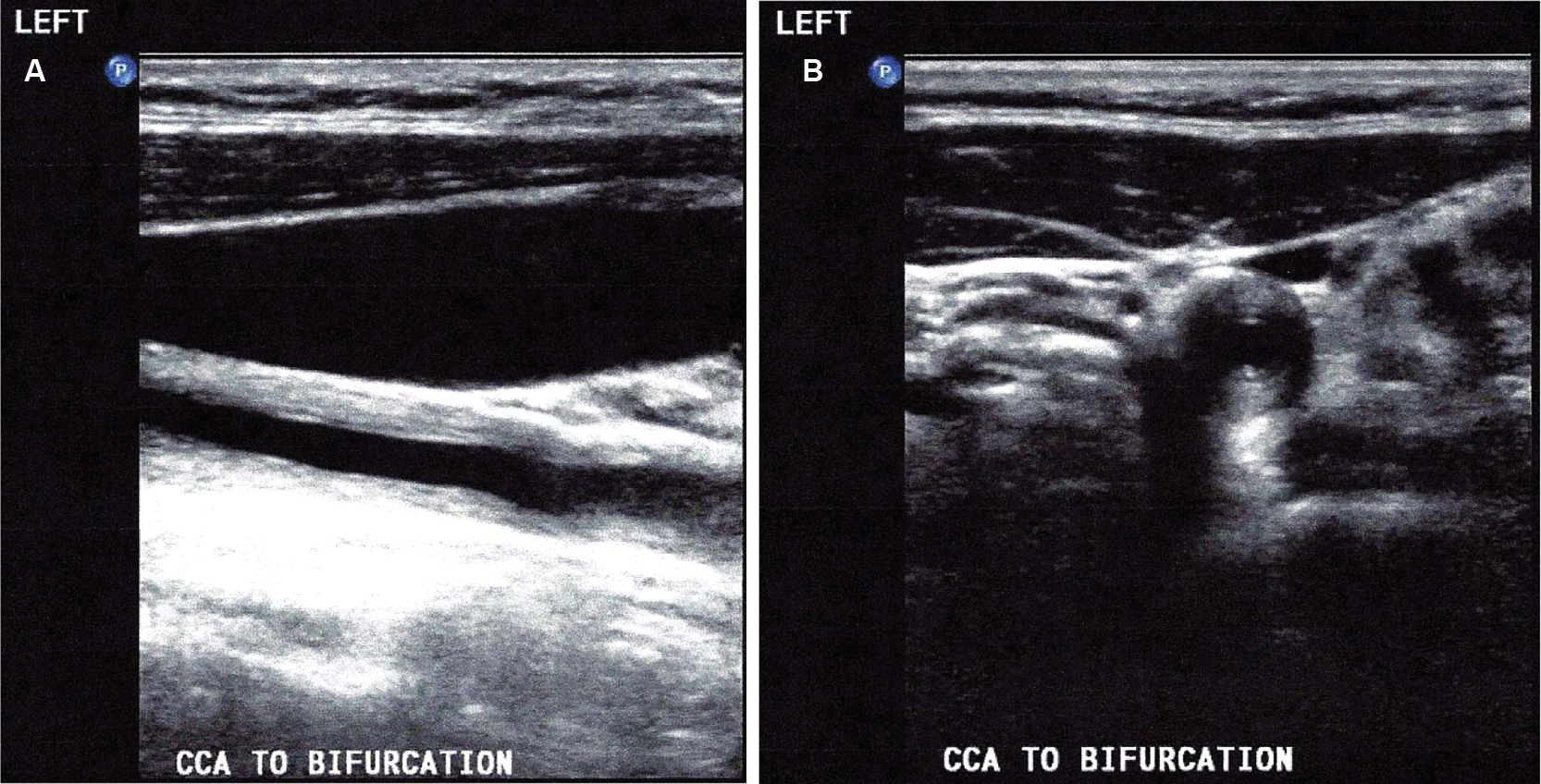
Carotid duplex demonstrates common carotid artery (CCA) circumferential thickening in the longitudinal view (left) and transverse view (right).
On the right side, subclavian artery color-flow and Doppler signals distal to the vertebral artery were absent, indicating occlusion. The right internal carotid artery (ICA) and external carotid artery (ECA) were clear. Mid-ICA peak systolic velocity (PSV) of 78 cm/s was normal (less than 125 cm/s). Right vertebral artery flow was elevated at 133 cm/s (normal, 20–60 cm/s) but antegrade.
Left subclavian artery color-flow and Doppler signals were greatly disturbed. There was hypoechoic plaque in the proximal ICA. Although the mid-ICA PSV was normal at 81 cm/s, the left vertebral artery flow was retrograde.
Arterial Physiologic Data
Brachial systolic pressures taken at the surgeon’s office were 57 mm Hg on the right and 85 mm Hg on the left, which were very low compared to the normal 120 mm Hg, as well as to the patient’s systolic pressures upon initial examination in the ED (118 and 112 mm Hg, respectively). Contralateral pressure gradient between brachial arteries was 28 mm Hg, indicating diseased aortic and/or subclavian arteries. 1
The right digit/brachial index (DBI) was low at 0.72 (normal, 0.8 or greater), a strong indication that arterial occlusive disease was impeding distal flow. However, DBI of 1.11 on the left suggests absence of further significant obstructive disease in the brachial artery, forearm, or palmar arch. 1 Corresponding Doppler waveforms clearly illustrate arterial disease bilaterally, questioning the usefulness of DBI as a sole test for excluding upper extremity arterial occlusive disease.
Lower extremity arterial waveforms were all triphasic with no pressure discrepancies between ipsilateral or contralateral segments, demonstrating normal perfusion from the common femoral artery to the posterior tibial and dorsalis pedis arteries (Figure 2). Ankle-brachial indices (ABIs) of 1.91 on the right and 1.85 on the left correctly identify the absence of significant arterial occlusive disease in the lower extremities. However, calculations using such diminished brachial pressures can falsely indicate noncompressible vessels. Medial calcinosis can be ruled out by arterial duplex or arteriography.1,2

Arterial physiological study showing poor upper extremity perfusion (top) and normal lower extremity perfusion (bottom).
Hypertension is a common symptom of TA, but brachial pressures of TA patients can misrepresent low systemic pressure if a major upper arm artery is stenosed. 3 Lower extremity pressures were all greater than 170 mm Hg, demonstrating that core blood pressure is adequately supplying arteries unaffected by TA and that hypotension probably is not a cardiac or systemic problem. Rather, it is inaccurately represented by brachial artery pressures. The ankle pressures in fact appear to indicate the presence of hypertension in this patient.
Transcranial Doppler
Transcranial Doppler (TCD) was performed to evaluate cerebrovascular blood flow, as well as thromboembolic events, which are a common complication of TA. 4 With the exception of the reversed vertebral, TCD showed normal cerebrovascular flow.
Other Findings
Blood Analysis
Both C-reactive protein (CRP) concentration (4.78 mg/dL) and erythrocyte sedimentation rate (ESR) (55 mm/h), “the most reliable marker of [TA] disease activity,” were elevated.3 Institutional criteria cite a normal range as 0.00 to 1.00 mg/dL for CRP and 1 to 20 mm/h for ESR. These values indicate active vascular inflammation and support a diagnosis of TA. 3
Contrast Arteriogram
The contrast arteriogram was repeated and confirmed right subclavian artery occlusion and high-grade stenosis of the left subclavian artery.
The right vertebral artery was enlarged, equal in size to the ipsilateral CCA (Figure 3). The left vertebral could not be identified, probably because retrograde flow kept contrast dye from entering the artery. The arteriogram also showed extensive collateralization supplying the right arm, indicating chronic disease and accounting for the presence of arterial waveforms distal to the occluded subclavian obtained in the arterial physiological examination.

Contrast angiogram comparing the enlarged right vertebral artery (A) to the right common carotid artery (B). Note also the absent (occluded) right subclavian artery.
Diagnosis and Treatment
Diagnosis
Key findings that led to a diagnosis of TA include nonatherosclerotic carotid artery wall thickening, impeded blood flow in the upper extremities with normal physiological arterial data in the lower extremities, elevated CRP and ESR, and arterial collateralization in the upper extremities.
Treatment
The patient began long-term steroid and immunosuppressant drug therapy.
Follow-up
Four Months
The patient reported reduction of symptoms. The only change, found by carotid duplex, was bidirectional rather than retrograde left vertebral artery flow. With exception of that vertebral finding, TCD showed normal cerebrovascular flow.
Seven Months
The patient reported no new symptoms. Brachial pulses were too diminished to obtain blood pressures, and carotid duplex showed reversion to retrograde flow in the left vertebral artery. Except for the left vertebral artery, TCD still showed normal cerebrovascular flow, and medications remained the same.
Discussion
History of TA
At the 1908 Japan Ophthalmological Society convention, Dr Mikito Takayasu described “wreaths” of collateral vessels around the pupils of a 21-year-old Japanese female patient that presumably developed in association with central vessel disease. After colleagues presented similar cases, they noticed that the patients also had nonpalpable wrist pulses—hence the name “pulseless disease.” Later autopsy of a TA patient revealed an inflamed aortic arch, generating another name, aortic arch syndrome. 5
Etiology and Incidence
TA has no known etiology but is believed to be a rare genetic autoimmune disorder 6 that typically targets young Japanese women. Although Japan reports 150 cases per year, 7 incidence in the United States is approximately 2.6 cases per million people per year. 8
Course of TA
TA has two stages: prepulseless (systemic) and pulseless (occlusive). Both can have intermittent inflammatory episodes, making TA difficult to diagnose and treat. Hypertension is usually the first sign, 9 but patients also commonly present with fever, malaise, and weight loss. 10
Aortic branch vessels occlude in the pulseless phase, leading to shortness of breath, dizziness, angina, vision deficits or blindness, and syncope. Clinical examination can identify bruits, nonpalpable wrist pulses, and high CRP and ESR levels. With imaging, thrombosis, stenosis, and aneurysms are often discovered. 10
Pulseless phase symptoms can reflect secondary diseases, such as renal artery stenosis, congestive heart failure, stroke, and aortic regurgitation. Heart failure is the most common cause of death. 11 There are five categories of TA based on the vessel segments that are affected. Type V, which includes the aortic arch, descending thoracic aorta, and abdominal aorta, is most common 9 (see Table 1).
Categories of Takayasu Arteritis 9

Chronic, calcified plaque is hyperechoic and heterogeneous, and it produces acoustic shadows. It attaches to the artery wall, causing the intimal to look uneven in some areas. With TA (in the absence of atherosclerosis), the intimal lining is smooth, but as the artery walls thicken, elasticity decreases over time.1,12
Treatment
There is no known cure for TA. Patients are typically prescribed antihypertensive medication and a corticosteroid regimen. Steroids not only have side effects difficult to tolerate but also induce remission in only about 60% of TA patients. 13 Those resistant to steroid treatment can take immunosuppressive drugs such as cyclophosphamide, methotrexate, and azathioprine to lessen symptoms. 1 However, no medications have been shown to affect the overall prognosis of TA. 10
Persistent and severe arteritis may be treated surgically with stents, grafts, bypasses (synthetic or native), and vessel transposition. A study performed at the University of Tokyo in 1989 tracked 30 TA patients for 10 or more years after surgical intervention. Data collected at the end of 10 years include the following: 56% of percutaneous angioplasty procedures were successful immediately, and about half of them were patent for at least one year. Bypass grafts had a 70% patency rate after 10 years. Autologous grafts were preferred to synthetic grafts; only 9% of patients with autologous grafts developed complications, whereas synthetic grafts had a complication rate of 30%. Reconstructed arteries had a 10-year success rate of 77%. 14
Prognosis
Six-year survival rates are 45% when comorbidities are involved. 15 An otherwise healthy patient may experience a five-year survival rate between 80% and 90%. 13
With such a small patient population, the medical community has limited references and has not presented a general prognosis for TA. 11 More research is needed to find the causes and cures.
Conclusion
Sonography can play an important role in investigating TA symptoms by detecting nonatherosclerotic wall thickening, poor distal perfusion, chronic collateralization, sole involvement of upper extremities, and cerebrovascular hemodynamic interruptions, among other signs, and is especially valuable in assisting physicians in tracking the effectiveness of TA treatments.
Footnotes
The author declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author received no financial support for the research and/or authorship of this article.