
Abstract
Conjoined twins are a rare anomaly. The classification of twinning that accounts for the majority of conjoined twins is thoraco-omphalopagus. This report discusses a case of female thoraco-omphalopagus twins who share a single cardiac system.
Medical professionals have been fascinated with conjoined twins for decades. They are a rare multiple-gestation anomaly that affects 1 in every 200 monozygotic twin gestations. Historically, there is a predominant sex of females, with a ratio of 3:1. 1 Management of this complex twinning depends on the time of diagnosis and where the fusion of anatomy is located. The case presented in this report is of thoraco-omphalopagus twins with a single cardiac system. This case is of particular appeal because of the complexity and rare incidences involving thoraco-omphalopagus twins with one heart are reported.
Case Report
A gravida 3, para 2, patient in her early thirties presented at the ultrasound outpatient department for a routine anatomical survey. According to her last menstrual date, her gestational age was 18 weeks and three days. Upon ex-amination by a Siemens Antares ultrasound machine and a convex sequenced array, two female fetuses conjoined at the heart were revealed (Fig 1 & 2). Normal separation appeared to be present of the head, spine (Fig 3), legs, and bladder (Fig 4). A single placenta was located anteriorly with two umbilical cord insertions. The abnormal heart was visualized demonstrating fusion of the great cardiac vessels Confirmation of this connection was further supported by the use of color doppler imaging (Fig. 5). Based on the findings, the diagnosis was made of thoraco-omophalopagus conjoined twins with a single heart measuring 19 weeks and 3 days gestation.

Thoraco-omphalopagus twins.

Conjoined twins with two separate spines.

Two stomachs visualized.
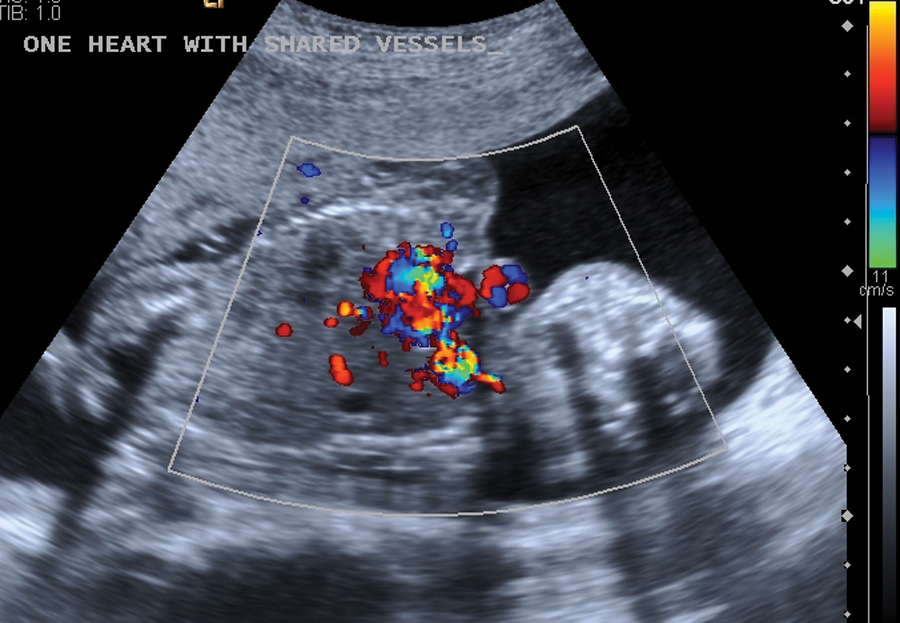
Color Doppler demonstrating fusion of the great cardiac vessels.

The four-chamber view of the fused heart.

The fused heart.
Both parents were counseled about the different options available for the pregnancy. The outcome of their decision was not available.
Discussion
Conjoined twins have an estimated frequency of 1 in every 50,000 live births. This number is misleading because as many as 60% die in utero, are stillborn or are terminated. Thus a more accurate occurrence would be 1 in every 250,000 gestations. 1
Although the exact etiology of such abnormalities is unknown, there are two embryologic theories that provide conceivable explanations. Heredity, maternal age and parity are unrelated to this random condition. Most commonly believe that conjoined twins arise from the incomplete division of the embryonic disk between the 12th and 15th day following fertilization (fissure theory). An alternative proposition is that the twins derive from a single ovum that completely divides into two discs and then reconnect due to the small vicinity in which they have to enlarge (fusion theory).1,2 This leads to the several different areas of anatomy that can be fused.
The complex malformations that develop with conjoined twins form several different types of unification. Those types are classified according to the most marked site of connection, along with the Greek suffix ‘pagus’ meaning fixed or fastened. Of these sites include thoracopagus (thorax), omphalopagus (abdomen), ischiopagus (pelvis), pyopagus (sacrum), or craniopagus (skull). Thoraco-omophalopagus twins appear the most often comprising a total of 70% of all conjoined twins. 3 This is significant because union of the thorax and abdomen is quite complex due to the tortuous paths formed during anastomoses of the fetal anatomy. Fusion of the heart is likely to result thus making the possibility of separating the twins difficult. A major factor in determining the feasibility of separation is the extent of unification and the time of diagnosis. 4 To better understand the importance of the degree of fusion, Seo et al has established classifications to describe five types of unification and their chances of separation. 5 (See Table 1).
Seo Classifications
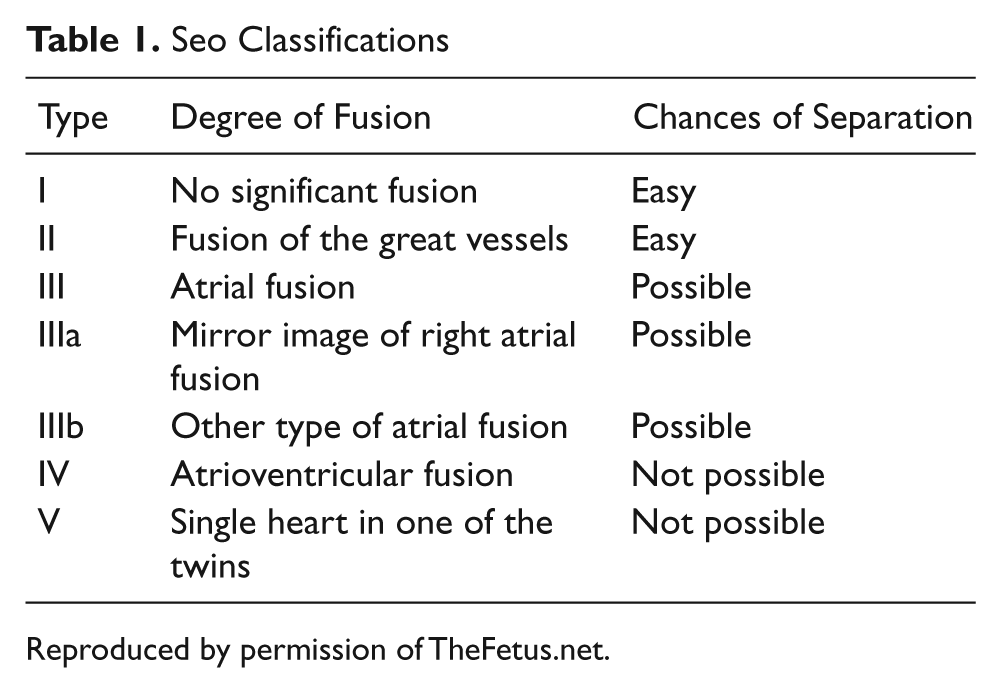
Reproduced by permission of TheFetus.net.
By using ultrasonography, prenatal diagnosis of conjoined twins is possible as early as 12 weeks gestation. 6 Due to the numerous variations in the types of conjoined twins, it is critical that the area of connection is properly identified as to determine the prognosis and plan of management. Detailed scanning and imaging should be performed on each fetus so that the shared major organs and connecting vasculature are accurately defined. Identifying the type and degree of fusion will aid in the possibility of intervention. An additional diagnostic imaging technique that is utilized to document fetal anomalies is magnetic resonance imaging (MRI). MRI can be used because it is provides dependable images that range in specific purposes such as when evaluating the heart and delineating soft tissues 7 ,8. This is imperative when evaluating conjoined anatomy. The technique may also be superior to ultrasonography in the case of oligohydraminos or maternal obesity. 7
Using such imaging modalities is essential in providing an early antenatal diagnosis that will help determine an anticipated survival of the twins, including a situation where an emergency separation at birth may be imperative. Computerized tomography and fetal echocardiography are also modalities of value 9. The delineation and identification of the configured anatomy should be found early as to allow plenty of time for planning a separation. This also helps prevent or minimize injury and harm to both the mother and twins. Such confirmation within the first and second trimester allows for adequate counseling to take place over the outcome and management of the pregnancy including a potential termination or appropriate planning for the time and mode of delivery.
Separation should always be considered for each case when it is attainable in the best interest of both infants. The surgery for separation is quite often extremely delicate and life threatening. When attempted, an experienced team with adequate resources is vital. In cases where there is intricate fusion of the heart or cerebrum, the chances of survival are doubtful 9. Mackenzie et al. described their experiences with 14 sets of prenatally diagnosed conjoined twins that were referred to their institution the Children’s Hospital of Philadelphia. Of those fourteen, ten were thoraco-omphalopagus. Complex fused cardiac systems were found in seven. The outcome of the pregnancies included three therapeutic abortions and seven planned cesareans. Survivors of these twins consisted only of the two sets of whom did not share a heart, thus demonstrating the prognosis for survival is usually very poor 10.
Conclusion
Although rare, conjoined twins occur often enough for sonographers to expect to encounter them during their careers, even if they do not work in a high-risk obstetric practice. Early diagnosis is necessary to prevent further complications and to optimize time in planning the management of the infants. The complexity of the fusion must be determined before any type of management of the pregnancy can be discussed with the affected families. Management may include options such as termination, elective cesarean, and immediate surgical separation after birth.
The case presented in this report demonstrates just one of the several forms of unification that can occur. It is quite significant because of the complex cardiac fusion. Patients can opt for a doctor to attempt surgical separation with conjoined twins but depending on the site of fusion, the surgery can range from being simple to very complicated. In the case of shared hearts, there should be careful consideration in the attempt of operative care. This decision can be supported by the use of prenatal ultrasonography which can accurately demonstrate the various connections between the atrial and ventricular chambers of the heart. The imaging modality has been found to be quite advantageous in this diagnosis. It is the first line used in diagnosis of this condition, so it is very important for sonographers to understand the various manifestations of conjoined twinning and their implications
Footnotes
Acknowledgements
The author thanks sonographers Karen Wright and Shagufta Jamil.
The author declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author received no financial support for the research and/or authorship of this article.