
Abstract
This study aims to investigate and compare the effects of six-week oral vitamin C supplementation on blood velocities, intima-media thickness, and cross-sectional diameter (CSD) of the common carotid artery of sickle cell anemia (SCA) and non–sickle cell anemia (NSCA) subjects using sonography. Results showed that the CSD and end-diastolic velocity were significantly higher (P < .002 and P < .001, respectively) in the SCA subjects than in the NSCA subjects in the presupplementation phase. Calculated resistivity index (RI) was significantly lower in the SCA subjects (P < .003). Vitamin C supplementation had a slight effect on all the measured parameters in the NSCA subjects but caused a significant increase in peak systolic velocity (PSV) (P < .02) and RI (P < .01) in SCA. A comparison of change in each measured variable between the groups showed significant differences. Oral supplementation with vitamin C should be encouraged in patients with SCA as prophylaxis against endothelial damage, thereby preventing vaso-occlusive crises and their associated morbidity.
Various studies have been carried out on the interaction between sickle red cells and vascular endothelium, with researchers demonstrating that almost all major adhesion pathways are involved in this interaction.1–3 Carotid endothelial damage results in plaque formation, which, when detected subclinically, enables early intervention, thereby preventing stenosis, infarction, and stroke. 4 On average, 11% of patients with sickle cell anemia (SCA) will develop a clinically apparent stroke by age 20 years and 24% by age 45 years. 5 The first episode usually occurs between ages 2 and 15 years. 6
In patients with SCA, the baseline levels of vitamin C have been shown to be depressed. 7 Ascorbic acid consumption has been shown to decrease the arterial blood pressure, forearm vascular resistance, and number of irreversibly sickled cells but increases forearm blood flow, hemoglobin concentration, and packed cell volume in adults suffering from SCA.8,9 Vitamin C restores the nitric oxide (NO) production and replenishes intracellular antioxidants, 10 which tonically enhances large artery compliance. 11 In disease states, restoration of NO activity leads to improvement in endothelium-dependent vasodilatation, thereby protecting such patients from ischemia.12–14 This study compares the effects of vitamin C supplementation on blood velocities, intima-media thickness (IMT), and cross-sectional diameter (CSD) of the common carotid arteries of SCA patients with those of non–sickle cell anemia (NSCA) subjects.
Materials and Method
A random selection of 20 NSCA students of the College of Medicine, University of Lagos, with genotype HbAA, as noted in their medical records on admission into the university, was recruited as controls for this prospective study. They were nonsmokers and nonalcoholics, and they were not on any drug therapy at least six months to the time of the study. In addition, 10 patients diagnosed with SCA registered with the adult Sickle Cell Clinic of the Lagos University Teaching Hospital were also recruited for the study. Both groups comprised young adults aged 16 to 25 years. Exclusion criteria included a history of conditions such as diabetes or hypertension. Informed consent was obtained from every volunteer used.
A digital blood pressure monitor (model 6016, American Diagnostic Corporation [ADC], Hauppauge, New York) was used to obtain the blood pressure and pulse rate. Each subject sat quietly for five minutes before the measurement, without talking, with legs uncrossed and the arm supported at heart level. Measurements were repeated three times, and the average of the three measures was recorded. All subjects were weighed using the same weighing scale. Height was measured in all volunteers with a tape rule fixed to the wall.
Examination of the right common, internal, and external carotid arteries was performed in the longitudinal and transverse planes by one observer (O.A.O.), using a duplex sonographic scanner (Aloka ProSound SSD-3500; Aloka, Wallingford, Connecticut) with a high-frequency (5–10 MHz), linear-array transducer. All examinations were performed with the subjects in the supine position with the chin extended and their head slightly turned away from the side being examined. A 20- to 30-degree lateral to medial transducer angle was also applied, in order to use the sternocleidomastoid muscle as an acoustic window. 15 Right-sided measures were used for convenience. 16 The external CSD (interadventitial distance) and the IMT of the posterior wall of the right common carotid artery (CCA) were measured in the longitudinal plane on frozen enlarged gray-scale images. IMT was defined as a low-level echo gray band that did not project into the arterial lumen and was measured during end diastole as the distance from the leading edge to the second echogenic line of the far walls of the CCA. 17 It was measured 1.0 cm proximal to the carotid arterial bifurcation using manually placed electronic calipers. An average of three readings obtained was documented.
Subsequently, a sample volume of 3 mm was placed on the point of the highest velocity acceleration of the right common carotid as determined by the color-aliasing artifact, with 45° as the angle of insonation to increase accuracy and reproducibility. 18 The peak systolic velocity (PSV), end-diastolic velocity (EDV), and resistivity index (RI) of the right common carotid and internal carotid arteries were measured at these points, which were at least about 1 cm away from the carotid bulb. PSV was recorded as the highest point on the waveform. EDV was measured at a point just before the onset of the next waveform.
All subjects were placed on daily oral supplementation with 300 mg of vitamin C (Mopson Pharmaceuticals, Lagos, Nigeria). This dosage was used because the optimal daily dose of vitamin C ranges between 200 and 400 mg per day. 19 After six weeks, a repeat examination was performed. The subjects were advised not to smoke, drink alcohol, use aspirin, or take any vitamin supplements during the six-week period.
Data Analysis
The pulse pressure (PP) was calculated as systolic blood pressure (SBP) minus the diastolic blood pressure (DBP), whereas the mean arterial blood pressure (MABP) was calculated using the following formula: MAP = DP + 1/3 PP. Body mass index (BMI) was subsequently calculated 20 as weight in kilograms/height in (meters) 2 . The RI, which estimates the degree of resistance to flow in a vessel, was calculated using the formula of Sanders and Winter 15 :

Data collected were analyzed using SPSS software PASW Statistics 17.0.2 (SPSS, Inc, an IBM Company, Chicago, Illinois). Analysis of variance (ANOVA) was used to compare differences between the groups before and after vitamin C supplementation. Statistical significance was accepted when P < .05. Data are presented as mean ± SEM.
Results
The SCA subjects showed significantly lower mean height and weight compared with the NSCA subjects (P < .01 and P < .05, respectively). They also had significantly decreased hemoglobin values and packed cell volume (P < .001, respectively) compared with the NSCA group (Table 1). No differences were seen in the blood pressure measurements (Table 2). Table 3 shows that before vitamin C supplementation, EDV in the common carotid artery was significantly higher in the SCA subjects than in the NSCA subjects (P < .001). However, RI was significantly lower in SCA subjects (P < .01). In the SCA subjects, vitamin C supplementation increased the PSV and RI of the CCA (P < .05 and P < .01, respectively). Postsupplementation, the EDV of the CCA still remained significantly higher in the SCA subjects compared with the NSCA subjects (P < .001). The CSD of the common carotid artery was significantly higher in the SCA subjects than in the NSCA subjects (P < .01). In the SCA subjects, vitamin C supplementation significantly reduced CSD (P < .01) but not in the NSCA group. There were significant differences when the mean changes in CSD, IMT, PSV, EDV, and RI in both groups were compared (Table 4).
Baseline Anthropometric and Hematologic Measurements in Non–Sickle Cell and Sickle Cell Subjects
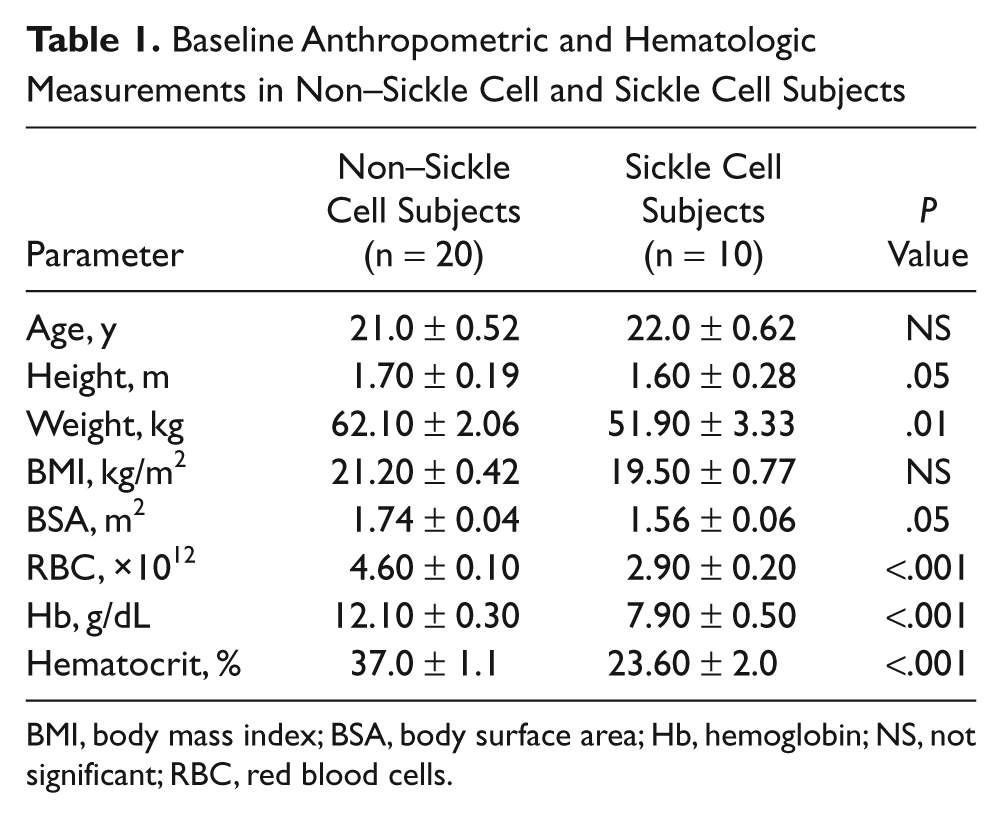
BMI, body mass index; BSA, body surface area; Hb, hemoglobin; NS, not significant; RBC, red blood cells.
Anthropometric and Blood Pressure Measurements in Non–Sickle Cell and Sickle Cell Subjects
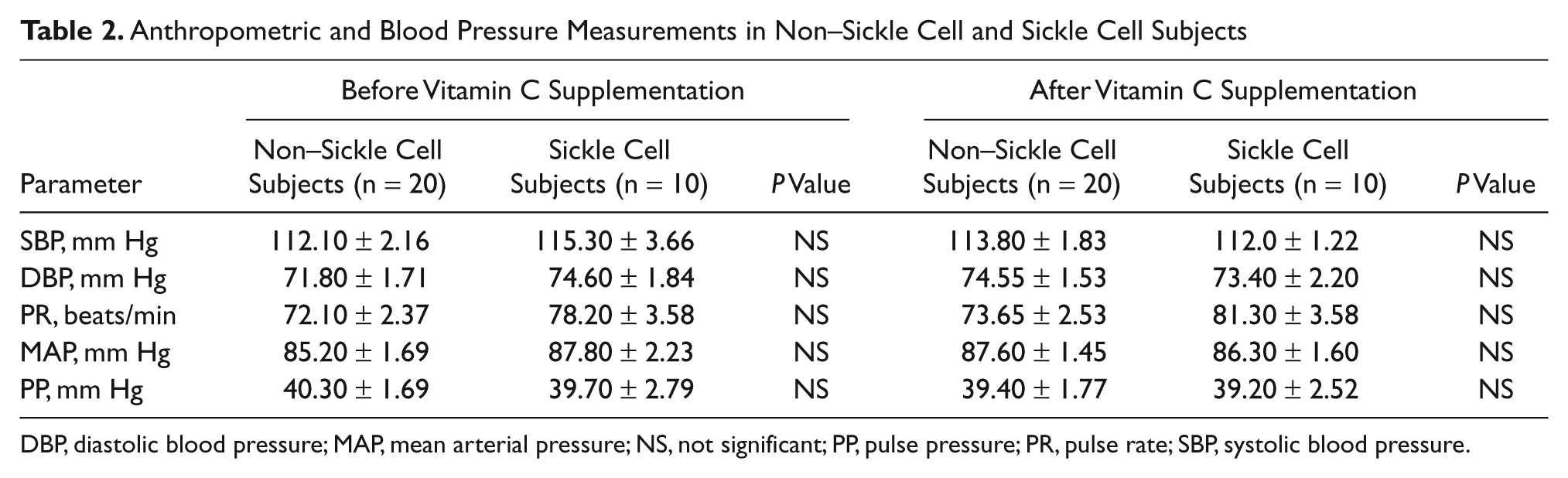
DBP, diastolic blood pressure; MAP, mean arterial pressure; NS, not significant; PP, pulse pressure; PR, pulse rate; SBP, systolic blood pressure.
Comparison of Effects of Vitamin C Supplementation in the Right Common Carotid Artery
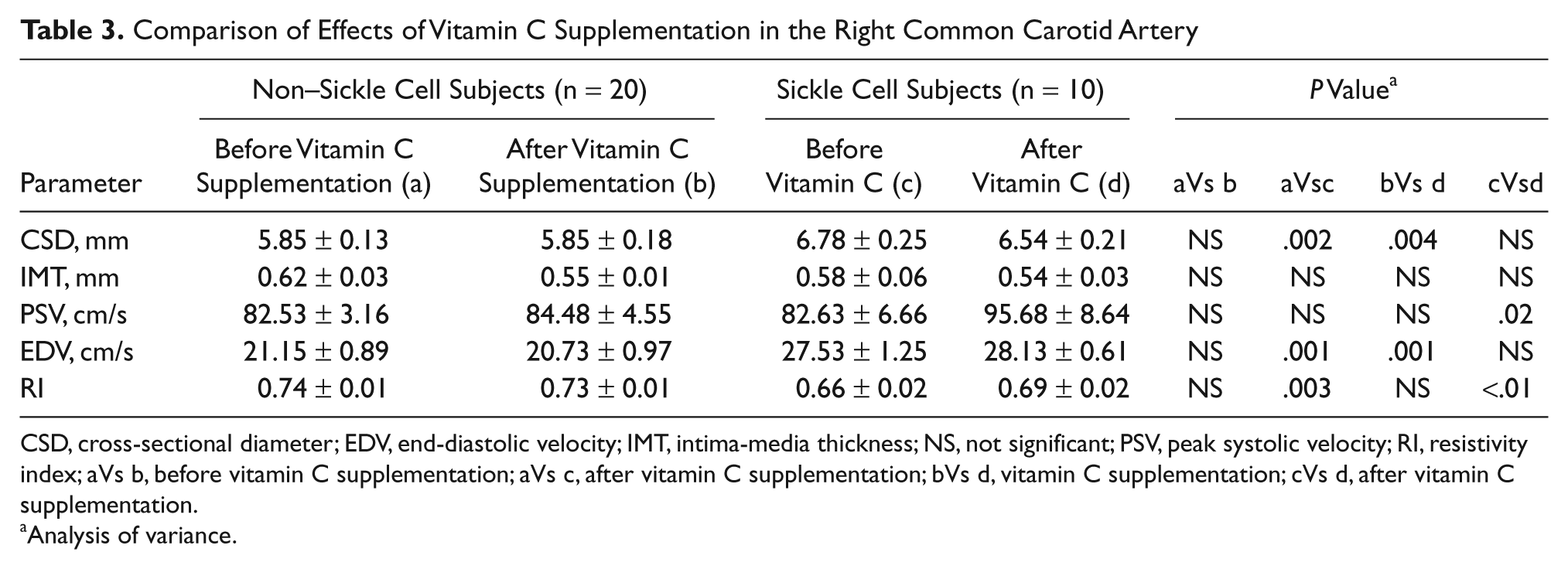
CSD, cross-sectional diameter; EDV, end-diastolic velocity; IMT, intima-media thickness; NS, not significant; PSV, peak systolic velocity; RI, resistivity index; aVs b, before vitamin C supplementation; aVs c, after vitamin C supplementation; bVs d, vitamin C supplementation; cVs d, after vitamin C supplementation.
Analysis of variance.
Comparison of Changes (Δ) in Measurements of the Right Common Carotid Artery in Non–Sickle Cell and Sickle Cell Subjects After Vitamin C Supplementation
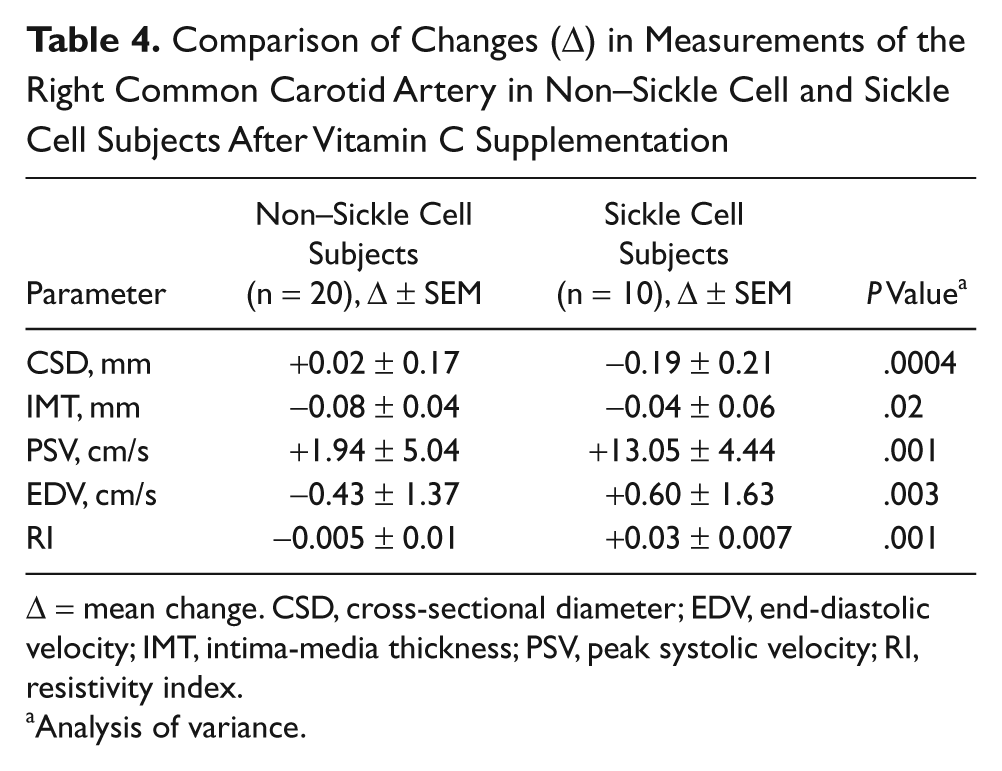
Δ = mean change. CSD, cross-sectional diameter; EDV, end-diastolic velocity; IMT, intima-media thickness; PSV, peak systolic velocity; RI, resistivity index.
Analysis of variance.
Vitamin C had a significantly greater effect on reducing the CSD in the SCA group (P < .001), but its effect of reducing the IMT was significantly greater in the NSCA group compared with the SCA group (P < .05). Vitamin C also had a significantly greater effect on increasing the PSV, EDV, and RI in the SCA group (P < .001, respectively).
Discussion
Subjects with sickle cell anemia were noted to have low mean height, weight, and BMI. They also had decreased hemoglobin values and packed cell volume. This has also been observed in previous studies.21,22 The average baseline blood pressure measurement in subjects with SCA in our study was similar to that of the control subjects. Blood pressures in SCA subjects have been shown to be similar or lower than those of NSCA subjects.22–24 It has been demonstrated that individuals with SCD have blood pressure levels that are significantly lower than in the general population. Blood pressure values that could be considered mildly hypertensive in healthy individuals put SCD patients at risk. 25 A nonstatistically significant decrease in the SBP and DBP in our sickle cell group was noted post–vitamin C supplementation. Other studies on SCA adults have shown significant lowering of blood pressure in this group of patients post–vitamin C intake. 15 The increased pulse rate (PR) observed in both groups after vitamin C administration has been attributed to the ability of vitamin C to increase NO bioavailability. 26
In the presupplementation phase, the CSD and EDV were significantly higher (P < .002 and P < .001, respectively) in the SCA subjects than in the control group matched for age and race (Table 3). These observations could be attributed to the higher cardiac output, which occurs secondary to anemia in this group. 23 Calculated RI was significantly lower in the SCA subjects (P < .003). This could be due to the higher baseline end-diastolic velocity seen in this group (Table 3). Our baseline IMT values of 0.62 ± 0.03 mm and 0.58 ± 0.61 mm in the NSCA and SCA groups, respectively, did not exceed the upper normal limit of 0.9 mm. 27 These values, however, were slightly higher than an age-matched study by Sass et al. 28 They obtained an average value of 0.49 mm from 193 healthy young adults between 10 and 24 years of age. Stein et al., 29 on the other hand, reported an average of 0.665 mm out of 519 controls in the 25- to 40-year age bracket. This was higher than what we observed. The lower baseline IMT observed in the SCA subjects when compared with the NSCA group may be due to the positive association between BMI and IMT. 30
The changes brought about by supplementation were more manifest in SCA than in NSCA subjects (Table 3). There was a significant increase in PSV of the SCA group postsupplementation. It is not clear why this happened. However, it has been shown that an increase in the viscosity of blood of SCA subjects may be due to the presence of irreversibly sickled cells. 31 Although not reported in this study, an earlier study had shown that vitamin C supplementation reduced irreversibly sickled cells. 8 Thus, a decrease in viscosity brought about by a reduction in irreversibly sickled cells following vitamin C supplementation may have contributed to the increase in blood flow velocity in accordance with Poiseuille’s law. 32
An increase was also observed in EDV in the SCA group post–vitamin C supplementation. This agrees with previous findings that vitamin C supplementation reduces forearm vascular resistance and increases forearm blood flow in patients with sickle cell disease. 9 This increased forward flow in diastole is expected because EDV is affected by the vascular resistance of the distal arterioles. 15 It has been shown that vitamin C enhances vasodilatation by restoring the plasma NO that had been depleted by the hemoglobin released during the process of hemolysis.23,33 Decreased plasma levels of NO may also activate adhesion molecules and potent vasoconstrictors. 34
In non–sickle cell subjects, there was a slight decrease in the RI of the CCA after vitamin C intake. This, however, was not the same in the sickle cell group, in which a significant increase in RI was observed (Table 3). The significant increase in RI observed in the SCA group could result from an increase in the PSV, as expected from the RI formula (equation (1)). 15 The formula shows that the RI will increase when there is a marked increase in PSV and just a slight increase in EDV because the large difference between the two velocities is the numerator in the equation. There was no significant change in the CSD of the control subjects following vitamin C consumption (Table 3). However, we noted a decrease in the IMT of both groups following oral ascorbic acid intake. This agrees with another study in elderly men. 35
The differences observed in mean changes of the CSD in both groups were statistically significant (Table 4). The significantly greater effect of vitamin C on reducing the CSD in SCA subjects (P < .001) could be due to the improvement in anemic status that occurs in these patients following an increase in hemoglobin concentration and packed cell volume postsupplementation, as noted by other studies. 22 However, the significantly greater effect of vitamin C in reducing the IMT in the NSCA group compared with the SCA group (P < .05) could possibly be due to the underlying endothelial dysfunction in SCA subjects. 23
From this study, it was observed that oral vitamin C supplementation produced a significant increase in PSV and RI in the CCA of SCA subjects, possibly by reducing the number of sickle red blood cells. A decrease was also seen in the CSD and IMT of the CCA in these subjects. Oral supplementation with vitamin C for a longer duration may result in more significant reduction in these parameters. This would encourage routine prescription of vitamin C to patients with sickle cell anemia as prophylaxis against endothelial damage, thereby preventing vaso-occlusive crises and its associated morbidity.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.