
Abstract
Objective:
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) affects the cardiovascular system by activating systemic inflammatory responses that cause vascular dysfunction. However, the long-term effects of SARS-CoV-2 on the cardiovascular system remain unclear. Therefore, this study aimed to compare the carotid intima-media thickness (cIMT) between patients who have recovered from Coronavirus disease-2019 (COVID-19) and healthy individuals to evaluate the feasibility of vascular complications in the postinfection phase of COVID-19.
Materials and Methods:
In this cross-sectional study, the cIMT was compared between 47 recovered patients with severe COVID-19 and 42 healthy individuals without a history of COVID-19 (controls) using Doppler sonography. Demographic and sonographic data were analyzed using SPSS version 26 statistical software.
Results:
A total of 47 young adults (30.8 ± 5.78 years, 7 men and 40 women) were evaluated 3 to 6 months after hospitalization for severe COVID-19, and were compared with 42 young healthy individuals (26.5 ± 5.85 years, 5 men and 37 women). The mean right and left cIMT were significantly lower in recovered COVID-19 patients than in healthy individuals (right cIMT: case group, 0.38 ± 05 mm vs control group, 0.40 ± 0.02 mm, P < .01; left cIMT: case group, 0.38 ± 0.05 mm vs control group, 0.40 ± 0.02, P < .01).
Conclusion:
A history of positive SARS-CoV-2 was associated with lower cIMT compared with controls. In this cohort, endothelial dysfunction may not have been the main driver of COVID-19 complications in recovered patients. However, more studies should be conducted on the relationship between cIMT and vascular complications.
Coronavirus disease-2019 (COVID-19), transmitted by severe acute respiratory distress syndrome coronavirus 2 (SARS-CoV-2), has caused millions of morbidities and mortalities worldwide and has been considered the greatest public health challenge in recent decades.1,2 Many studies have reported that SARS-CoV-2 infection is associated with a wide spectrum of cardiovascular diseases (CVD), such as myocarditis, stress cardiomyopathy, micro or macrovascular thrombosis, arrhythmias, acute coronary syndrome, and heart failure. 3 – 9 The main pathophysiological effects of SARS-CoV-2 on the vascular system are related to systemic inflammatory responses and cytokine release syndrome, both of which can induce viral adhesion to the angiotensin-converting enzyme-2 (ACE-2) receptor. This process leads to inflammatory cell infiltration, endothelial cell apoptosis, and microvascular thrombogenic effects; 10 – 12 thus, overexpression of cytokines in arteries is associated with intimal necrosis, endothelial denudation, and hypercoagulability. 13 Consequently, these changes can lead to arteriosclerosis even during the acute phase of infection.14,15 The work of Cristina-Oliveira et al 16 Riou et al 17 and Araújo et al 18 showed that hospitalization due to COVID-19 infection was associated with endothelial dysfunction, arterial stiffness, and changes in flow rates.
Carotid intima-media thickness (cIMT) is used as a reliable marker for early atherosclerosis and a strong predictor of future vascular events, such as myocardial infarction and cerebrovascular accident. 19 The cIMT, which is measured using gray-scale sonography, is a useful tool for CVD risk stratification. 20 Willeit et al 21 and Ren et al 22 reported that the extent of intervention effects on cIMT progression can predict the degree of CVD risk reduction and thrombotic events. Increased cIMT has been observed in patients with systemic arterial hypertension, diabetes mellitus, and obesity, 23 all of which have been attributed to COVID-19 complications.
Therefore, prolonged inflammatory processes can lead to vascular dysfunction, which may have additional implications on cardiovascular health. 14 Given the large number of patients with COVID-19, there is an urgent need to understand its long-term cardiovascular consequences that remain unclear. Therefore, this study aimed to evaluate the bilateral cIMT measurements between patients who have recovered from COVID-19 (case group) and healthy individuals with no history of COVID-19 (control group) to assess possible cardiovascular complications.
Materials and Methods
Study Population
This case-control study was conducted in two educational hospitals (Zahedan, Iran) in 2022. Written and oral informed consent was obtained from all participants. This study was reviewed and approved by the ethics committee and Institutional Review Board of the Zahedan University of Medical Sciences (REC.1401.303). This study adhered to the principles of the Declaration of Helsinki.
The case group included 20 to 40 patients who have recovered from COVID-19 (confirmed by real-time PCR testing) and were admitted to the intensive care unit. They were followed up for 3 to 6 months after discharge and were asymptomatic at the time of the study. The control group included 20 to 40 healthy individuals who, neither themselves nor their housemates, had no symptoms of respiratory infection, fever, myalgia, sore throat, or any systemic symptoms of COVID-19, since December 2019. The exclusion criteria for all subjects were smoking, alcohol consumption, obesity (body mass index greater than 30 kg/m2), a known history of CVD, hyperlipidemia, hypertension, diabetes mellitus, chronic kidney disease, thyroid disease, rheumatic diseases, and malignancies.
The sample size of the study was calculated according to the following formula based on the results of Szeghy et al24,25

where α = 0.05, ß = 0.2, d = 0.04, and standard deviation = 0.06
The minimum number of samples required to satisfy the desired statistical constraints was 40. Therefore, the goal was to select at least 40 individuals from each group using convenience sampling. There were 47 patients with a history of severe COVID-19 (case group) and 42 healthy individuals with no history of COVID-19 or relevant clinical symptoms (control group) included in this study:

Sonographic Assessment
Common carotid artery (CCA) intima-media thickness (CCA-IMT) was measured by a radiologist according to the current guidelines 26 using a WS80A ultrasound equipment system (Samsung, Seoul, South Korea). The patients were first placed in the supine position with their necks turned away from the side of the examination. A high-frequency linear transducer (12 L-RS; 12-MHz) was then placed 1 cm below the bifurcation (1 cm proximal to the bulb), and sagittal imaging of the CCA was obtained, which allowed at least five measurements that were performed manually on each side, to obtain the average intima-media thickness (IMT) value. The CCA-IMT was evaluated as the distance between two echogenic lines at the intima-lumen interface (blood-intima interface) and the media-adventitial junction at the far and near walls, respectively (See Figure 1). All participants first underwent a comprehensive examination of vital signs, particularly bilateral blood pressure, to rule out subclavian steal syndrome. Grayscale and Doppler measurements were performed to assess possible arteriovenous malformations.
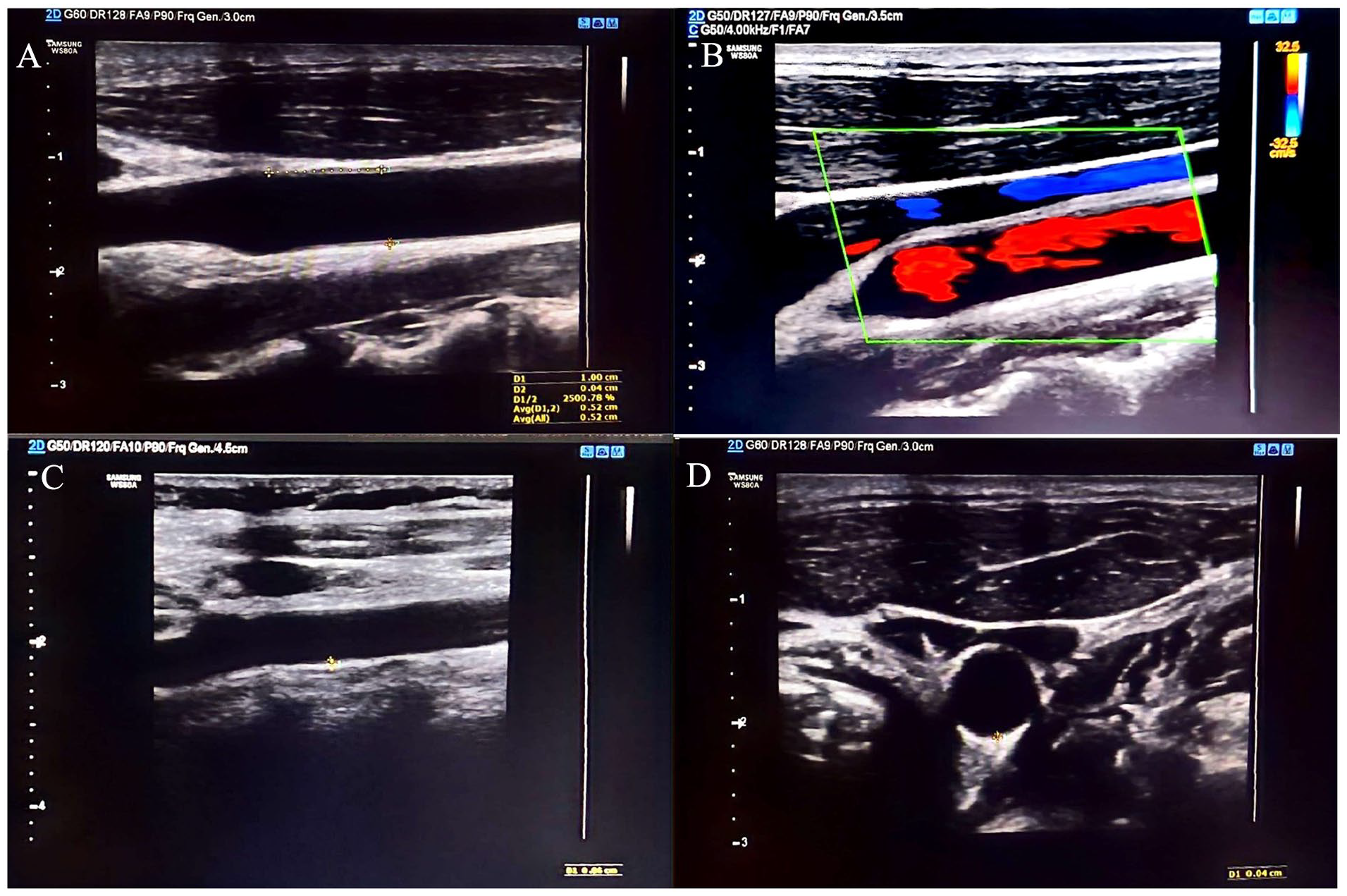
(A) The measurement on the posterior wall of the CCA, 1 cm from the carotid bifurcation. (B) The use of Doppler to determine carotid artery and intimal margin. (C) A gray-scale assessment of the CCA-IMT. (D) A representative transverse sonographic view of the CCA-IMT. CCA, common carotid artery; CCA-IMT, common carotid artery intima-media thickness.
Statistical Analysis
Statistical analyses were performed using SPSS version 26 (IBM Corp., Armonk, New York, USA). For descriptive comparison of the two groups, the chi-square test was performed and for quantitative comparison of the two groups, the Mann–Whitney U test was performed. Statistical significance was set at P ≤ .05.
Results
This study was based on the evaluation of 47 young adults (30.80 ± 5.78 years, 7 male and 40 women), who were evaluated 3–6 months after a positive SARS-CoV-2 test result and were compared with 42 healthy individuals (26.50 ± 5.85 years, 5 male and 37 female) (see Table 1).
Demographic and Sonographic Parameters of the Case and Control Groups.
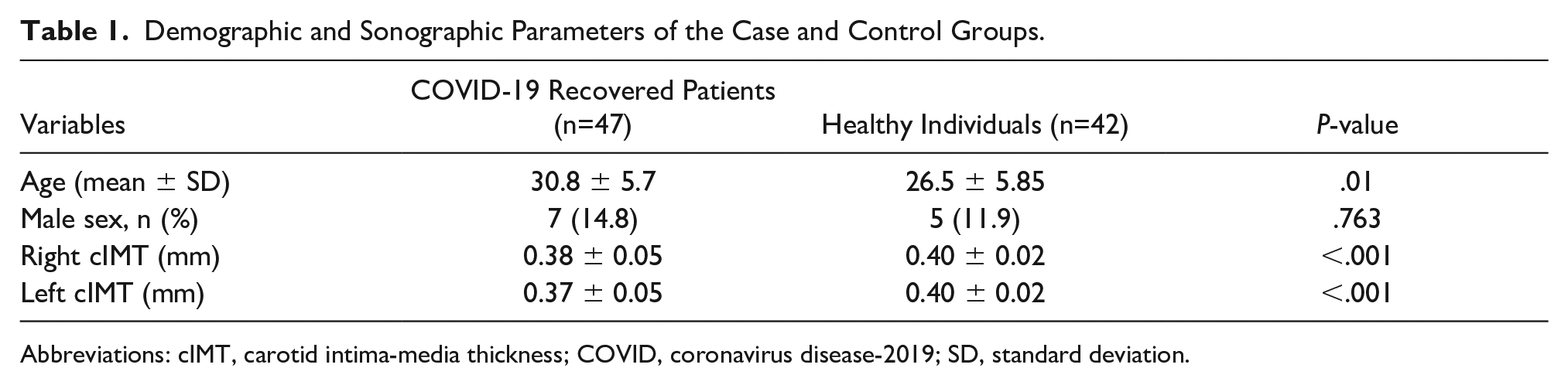
Abbreviations: cIMT, carotid intima-media thickness; COVID, coronavirus disease-2019; SD, standard deviation.
The mean right and left cIMT measurements were significantly lower in COVID-19 recovered patients compared with healthy individuals (right cIMT: case group, 0.384 ± 0.051 mm vs control group, 0.404 ± 0.026 mm, P < .01; left cIMT: case group, 0.385 ± 0.052 mm vs control group, 0.404 ± 0.025, P < .01) (see Table 1 and Figure 2).
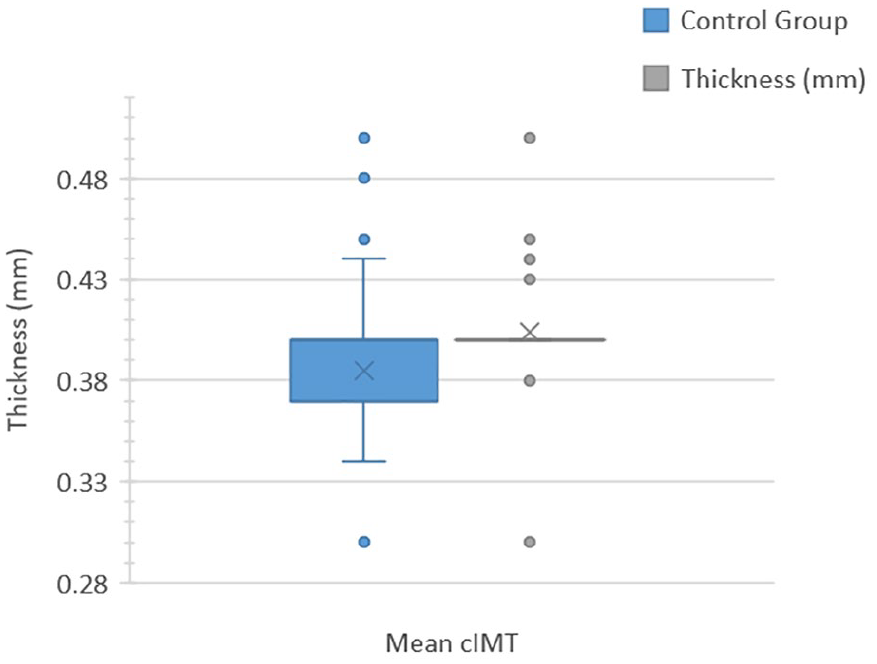
Box plot comparing the right cIMT between the case and control groups. cIMT, carotid intima-media thickness.
Discussion
The results of this cohort study demonstrated that post-SARS-CoV-2 infection had a significant effect on the CCA-IMT. Furthermore, these changes do not appear to have adverse CVD effects in patients who have recovered from COVID-19, and cIMT changes may be a reliable predictor of subclinical atherosclerosis and thrombotic events. 25 The acute phase of COVID-19 affects the cardiovascular system either directly through viral toxicity or indirectly through hypoxemia, sympathetic nervous system stimulation, thrombosis, systemic inflammation, dysregulation of immunity, and the renin-angiotensin system. 18 SARS-CoV-2 inhibits the conversion of angiotensin-2 to angiotensin 1 – 7 through its ability to bind to ACE-2 receptors, disrupting the non-classical axis of the renin-angiotensin system and leading to harmful vascular events. 4
Recent studies have shown that acute COVID-19 inflammatory process is associated with vascular complications. Ratchford et al 27 assessed vascular function via flow-mediated dilation, carotid-femoral pulse wave velocity (PWVcf), and single passive limb movement 3 to 4 weeks after a positive real-time PCR test for COVID-19. Their results indicated that COVID-19 is associated with vascular implications. In addition, Doğan et al 14 reported that the cIMT level of patients with COVID-19 was higher than that of healthy people. Bezerra et al 15 also showed that high IMT levels in hospitalized patients with severe COVID-19 were associated with increased mortality.
Despite these findings, post-COVID-19 era IMT levels in survivors have rarely been evaluated. The results of a longitudinal study (6 months follow-up) of arterial stiffness and blood pressure in young adults following SARS-CoV-2 infection showed that PWVcf levels decreased and arterial stiffness remained high for several months after recovery. 28 In addition, Lambadiari et al 29 showed a significant relationship between SARS-CoV-2 infection and endothelial dysfunction associated with myocardial dysfunction and COVID-19-related symptoms after 4 months of recovery. 29 Therefore, arterial complications are expected to occur in patients with persistent symptoms, such as dyspnea, cough, chest pain, and fatigue, as well as in patients with hypertension, approximately 6 months after recovery. Another long-term study (12 months follow-up) reported that COVID-19 patients at 12 months after infection presented with reduced levels of PWVcf and perfused boundary region which indicated the persistence of endothelial and vascular disorders 1 year after the infection. 30 Nevertheless, the current study showed that IMT levels decreased 3 to 6 months after acute COVID-19 infection. Further studies are required, especially in patients at high risk of thrombotic events, such as those with CVD, stroke, and chronic kidney disease, as well as in patients with residual symptoms of COVID-19.
Limitations
The major limitations of this study were its preexperimental research design, and threats to internal and external validity. In addition, the participants were recruited using convenience sampling and the majority of the participants were women, which may have indirectly influenced the results. Another issue encountered was the inability to assess the endothelial status prior to COVID-19 infection and at discharge; therefore, it was not possible to access prior cIMT data to determine the actual effect of SARS-CoV-2. This study was conducted on healthy individuals (no history of COVID-19 infection) and the impact of comorbidities, especially CVD, could not be assessed. It is also important to note that the control group was not evaluated using the COVID-19 PCR test to determine whether they were currently or previously infected with COVID-19. The lack of testing in the control group was due to the lack of adequate testing facilities during the pandemic. Finally, the cIMT were measured manually and the use of an IMT software for assessment may have improved the reliability and accuracy of the measurements.
Conclusion
The findings of this cohort study demonstrated that the cIMT decreased in patients with COVID-19. However, due to conflicting results from similar studies, further research is recommendedw.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is a specialty of radiology (MD) thesis supported by the Zahedan University of Medical Sciences (grant number: 10575).
Ethics Approval
Ethical approval for this study was obtained from the ethics committee and Institutional Review Board of the Zahedan University of Medical Sciences (REC.1401.303).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.