
Abstract
Introduction
Epilepsy is one of the most common neurological diseases affecting almost 46 million people worldwide. 1 Seizures and epilepsy can have a significant impact on quality of life (QOL), and QOL is generally rated poorer in those with epilepsy than in people with other chronic illnesses. 2 Seizure freedom is strongly associated with improved QOL, and the goal of therapy is to achieve complete seizure freedom without significant medication-related adverse effects. The mainstay of therapy continues to be antiepileptic drugs (AED) in prophylactic regimens, but one of the greatest challenges comes with optimizing the balance between seizure control and adverse effects of AED. 3 Although the majority of patients can be adequately controlled with AED, a significant number, estimated to be as high as 30%, stay uncontrolled with conventional medical treatment. 4 This can be further complicated if a patient has comorbid conditions potentially affecting seizure control and/or potentiating adverse drug reactions.
Pharmacists’ involvement in the care of patients with chronic conditions can make a significant difference to patient outcomes. 5 Similarly, pharmacists can play an important role in helping patients with epilepsy manage their medications. One study evaluating the outcome of pharmacist-managed AED therapy in hospital patients found significantly improved clinical and economic outcomes among patients who received pharmacist-managed AED therapy. 6 However, few studies have shown that pharmacists need support tools and resources to further their knowledge and skills in managing patients with epilepsy.7-10 Two studies have identified a lack of familiarity with the condition and its treatment for pharmacists and a distinct need for educational tools.7,8 In addition, 2 studies aimed at evaluating pharmacists’ knowledge of AED concerning women’s health identified both several knowledge gaps and areas for educational intervention.9,10 As pharmacists provide direct care to patients with epilepsy, it is important for pharmacists to be knowledgeable and comfortable in the clinical management of AED. To ensure patients with epilepsy are receiving excellent pharmaceutical care, it is important to characterize whether knowledge gaps exist among pharmacists practicing in Canada. To our knowledge, a study investigating Canadian pharmacists’ knowledge and comfort with the management of epilepsy and evaluation of educational needs has not been conducted in the past. Analysis of knowledge and comfort among Canadian pharmacists could play a pivotal role in the development of clinical support tools. Pharmacy-specific clinical tools designed to address the knowledge and comfort gaps in the management of epilepsy and AED can further contribute to improved patient care outcomes.
Our study aimed to use an online survey to answer the following research question:
This will aid in the future development of pharmacy-specific epilepsy educational support tools.
Methods
Study Design
A cross-sectional observational study was conducted using a 4-section survey to characterize Canadian pharmacists’ knowledge and comfort in managing patients with epilepsy. The Research Ethics Board at the University of Alberta approved the study protocol (Pro00102554). The survey was completed anonymously and no identifying information was collected. Only pharmacists licensed to practice in Canada were included in the study. Implied informed consent was obtained through participation in the survey, and participants were able to withdraw consent midway by closing the survey window.
The Survey
The survey was developed by the researchers through evidence-based guidelines and designed to target knowledge most relevant to pharmacists. The survey was reviewed for clinical accuracy and relevancy by coauthor Dr Sherif Hanafy Mahmoud, a clinical associate professor at the University of Alberta and recognized expert in neurology-related pharmacy practice. The survey (see the appendix) consisted of 4 sections: (1) questions about nonidentifying demographics, pharmacy education, practice setting, and neurology-related experience (n = 9); (2) questions aimed at evaluating pharmacists’ comfort in the management of epilepsy (n = 5); (3) multiple-choice and true/false questions to assess epilepsy management and AED-related knowledge (n = 12); (4) select-all-that-apply and free-text form for assessment of needs (n = 2). Comfort questions were rated on a 4-point Likert scale and evaluated epilepsy-specific skills, such as checking AED prescriptions, patient counseling, AED therapeutic drug monitoring (TDM), and AED tapering. The knowledge domain covered a series of pharmacy-relevant epilepsy topics, such as important drug interactions, AED management, women’s health, and generic substitutions. Some knowledge questions were true or false questions, whereas others had multiple-choice answers; all questions included an “I don’t know” option to prevent arbitrary guessing of answers. Participants were not provided with resources for the survey, but were not restricted from using any. The needs assessment had 2 “select-all-that-apply” questions assessing the therapeutic areas of need and tools of interest. A free-text question at the end of the survey was provided for any comments participants wanted to share about other tools or measures not addressed in the questions. None of the questions on the survey were required and participants were able to submit the survey with only a few questions answered. The estimated time to complete the survey was 15 minutes.
Survey Distribution
The survey was developed and results were stored on REDCap, a secure password-protected database hosted at the University of Alberta. The survey was distributed through a secure link to licensed pharmacists across Canada through multiple mediums to reach the maximum number of participants (provincial college of pharmacists and pharmacists association’s newsletters, member emails obtained through respective colleges for Alberta and Ontario, postings on private Facebook groups for pharmacists, and through the Canadian Society of Hospital Pharmacists [CSHP] Pharmacy Specialty Networks). Between Alberta and Ontario, 12 240 pharmacists were emailed with an invitation to participate in the study. On each medium, participants were sent an initial invite followed by a reminder every week for a month. The survey accepted responses for a total of 3 months from August to November 2020.
Data Analysis
Descriptive statistics were used to summarize demographic, comfort, knowledge, and needs data. Continuous variables were presented as mean ± standard deviation (SD). Categorical variables were presented as frequency and percentage, n (%). Comfort and needs data were summarized based on the percentage of participants who selected available choices. Knowledge questions were graded using points and expressed as a percentage of correct responses out of a total of 12. The option “I don’t know” was considered as an incorrect response. Mean scores were used to express overall answers. Knowledge questions were also scored individually to compare higher and lower scoring areas of care. A score of 50% was used as the minimum passing score for the knowledge component of the survey. Predictors of knowledge score greater than 50% were determined. The association between individual covariates (such as age, sex, practice experience, level of education, and neurology-related experience) and scores greater than 50% was determined using univariate logistic regression. Variables with estimated P < 0.2 were included in multivariate logistic regression models and adjusted odds ratios (OR) were determined. The fit of the final model was confirmed by using Hosmer-Lemeshow goodness-of-fit test. Area under the receiver operating characteristic (ROC) curve was determined to confirm model discrimination. Missing data, if any, were handled by complete case analysis. Level of significance was set at P < 0.05. Data analysis was conducted using Microsoft Excel and STATA software version 15.1 (STATA Corp, College Station, Texas).
Results
Survey Responses
A total of 903 responses were recorded through REDCap. After exclusion, a total of 605 complete responses were included in this study. Reasons for exclusion included responses that were empty (n = 61), duplicate (n = 4), and/or that contained only demographics (n = 42); partial responses that were not submitted were also excluded (n = 191). The response rate could not be accurately calculated as it is difficult to estimate how many pharmacists the social media posts reached. Of the participants invited through emails in Alberta and Ontario, the estimated response rate was 6.4%.
Demographics and Experience of the Survey Responders
Table 1 displays the summarized demographics, background, and experience of the study participants. Nearly two-thirds of the participants were females (61.6%) and the majority reported more than 10 years of practice experience (61.6%). A majority of participants reported Alberta (42%) or Ontario (51.3%) as their province of current practice, listed BSc Pharmacy (71.5%) as their highest level of pharmacy-related academic achievement, and obtained their degree from Canada (72.8%). The vast majority of the participants listed their current practice to be in community (66.1%) and had reported no experience working in a neurology-related field (75.5%).
Demographics, Background, and Experience of the Study Participants.
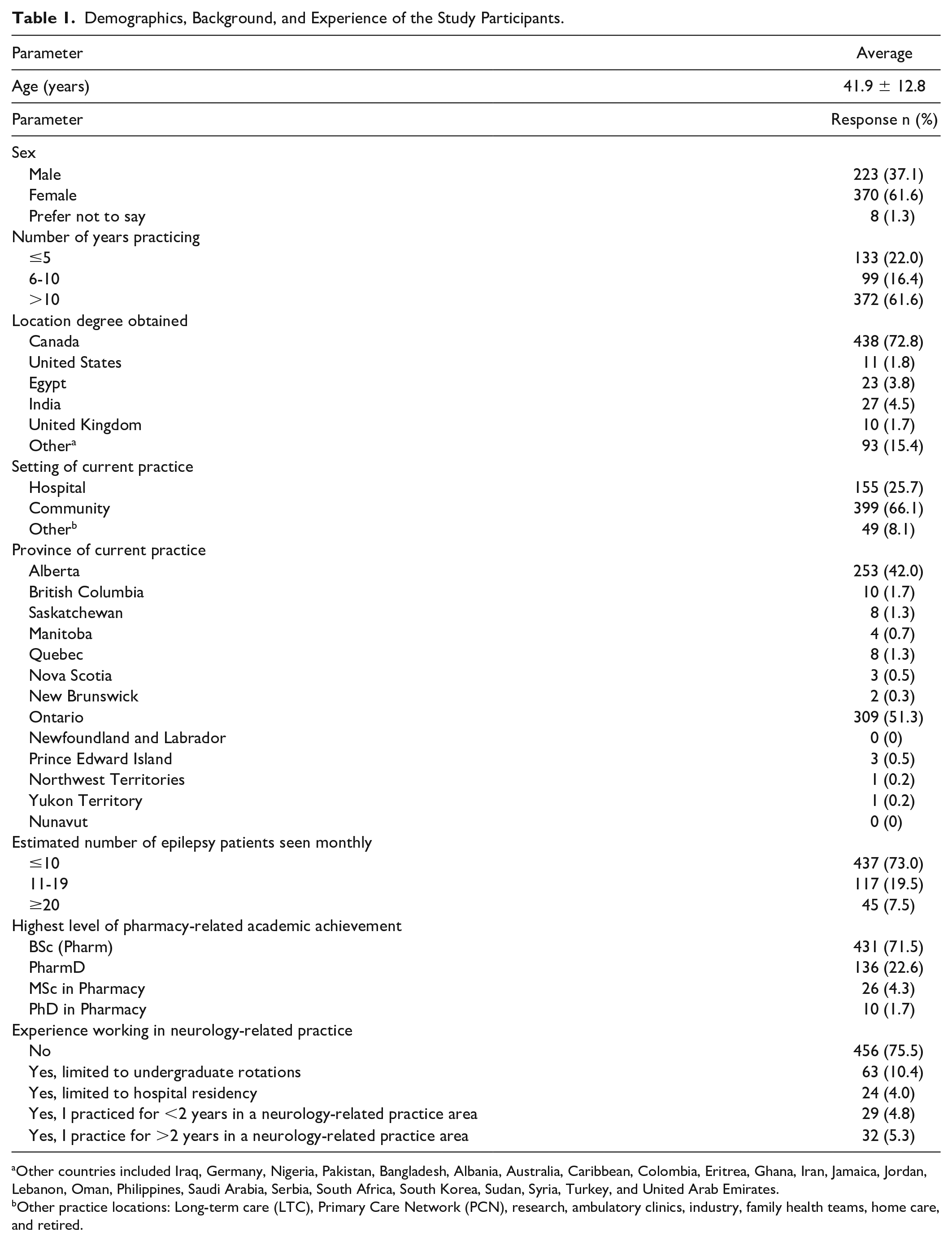
Other countries included Iraq, Germany, Nigeria, Pakistan, Bangladesh, Albania, Australia, Caribbean, Colombia, Eritrea, Ghana, Iran, Jamaica, Jordan, Lebanon, Oman, Philippines, Saudi Arabia, Serbia, South Africa, South Korea, Sudan, Syria, Turkey, and United Arab Emirates.
Other practice locations: Long-term care (LTC), Primary Care Network (PCN), research, ambulatory clinics, industry, family health teams, home care, and retired.
Pharmacists’ Comfort in Epilepsy Management
Figure 1 summarizes the pharmacists’ responses to comfort questions expressed as percentages. The response of the majority of participants was either “agree” or “strongly agree” to the statement inquiring about the comfort of participants in checking, identifying, and answering questions about drug interactions and counseling on AED. Conversely, more than 50% of the participants selected either “disagree” or “strongly disagree” when asked about their comfort with interpreting TDM and assisting patients to withdraw from AED. Interestingly, higher overall reported comfort was associated with higher scores on the knowledge component of the survey (P < 0.001).
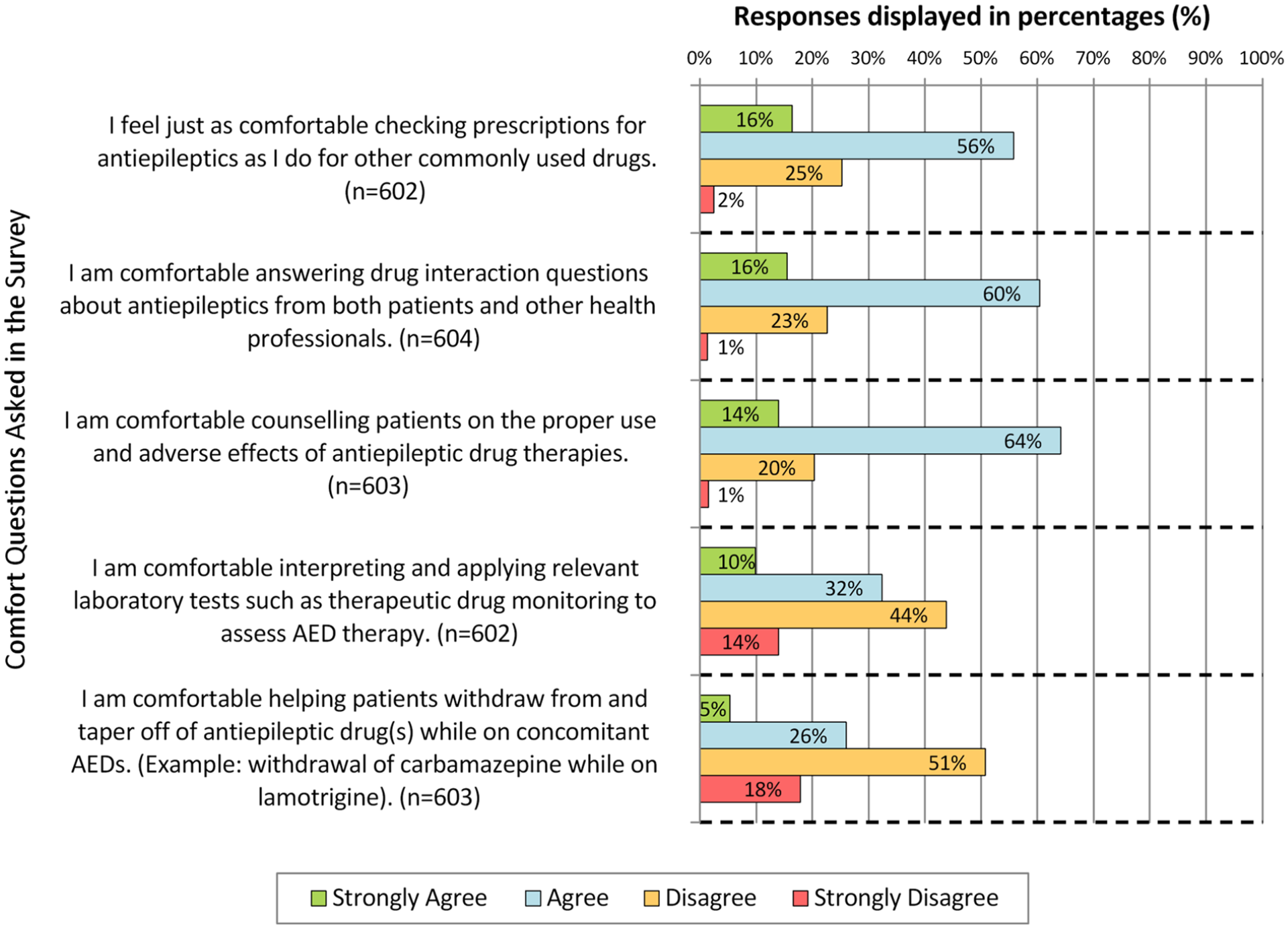
Canadian pharmacists’ comfort in epilepsy management survey responses.
Pharmacists’ Knowledge in Epilepsy Management
Figure 2 depicts the scores from the knowledge component of the survey. Participants scored the lowest in questions inquiring about AED choice based on the seizure type (22%), AED generic substitutions (32%), and TDM (39%). Conversely, the highest scores were noted on questions about more common topics such as nonpharmacological measures in epilepsy management (95%), folic acid use in women’s health (82%), and advantages of newer AED (74%). The overall average score on the knowledge component was 57.6% ± 19.1% (n = 602).
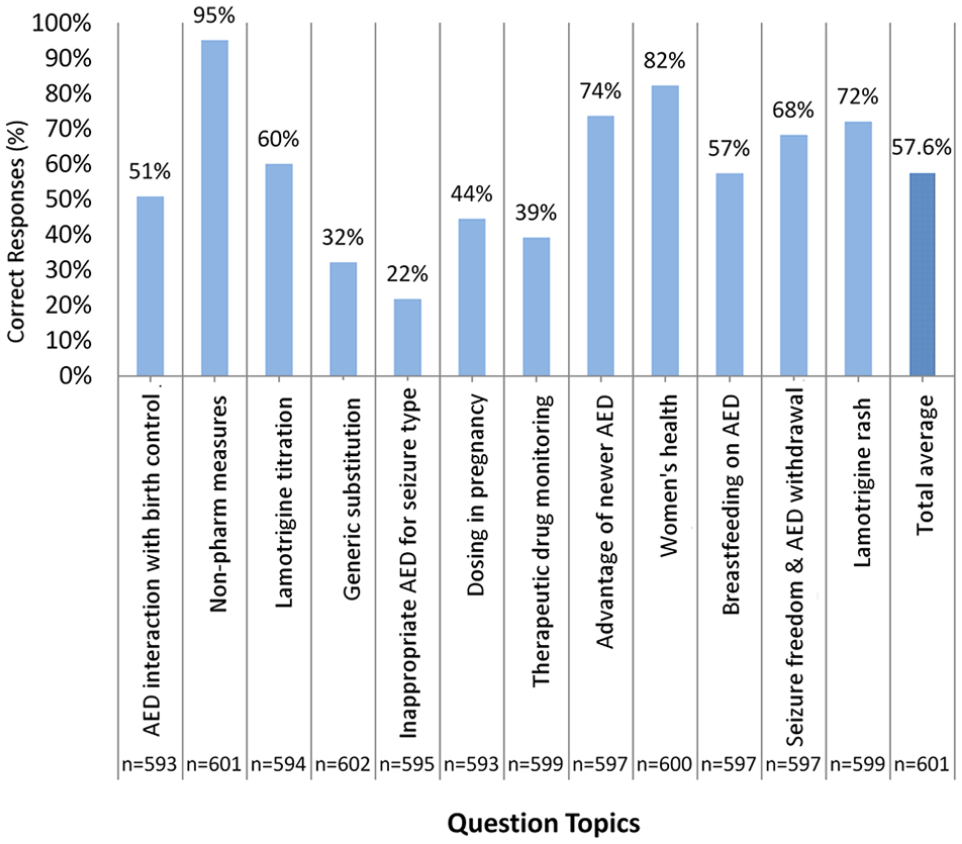
Overall scores on knowledge questions.
Logistic regression of scores revealed multiple predictors of scores greater than 50%. Male sex was associated with higher odds of scoring >50% (OR = 1.48, 95% confidence interval [CI] = 1.01-2.12, P = 0.044). Newer graduates with practice years less than or equal to 5 years had the highest odds of scores >50% compared with participants with 6 to 10 years (OR = 0.36, 95% CI = 0.20-0.66, P = 0.001) or greater than 10 years (OR = 0.48, 95% CI = 0.26-0.89, P = 0.02) of experience. Participants currently practicing in hospital had higher odds (OR = 2.09, 95% CI = 1.33-3.31, P = 0.002) of scoring >50% compared with pharmacists currently practicing in community. Figure 3 summarizes the average score by the pharmacists stratified based on years of experience and current practice.
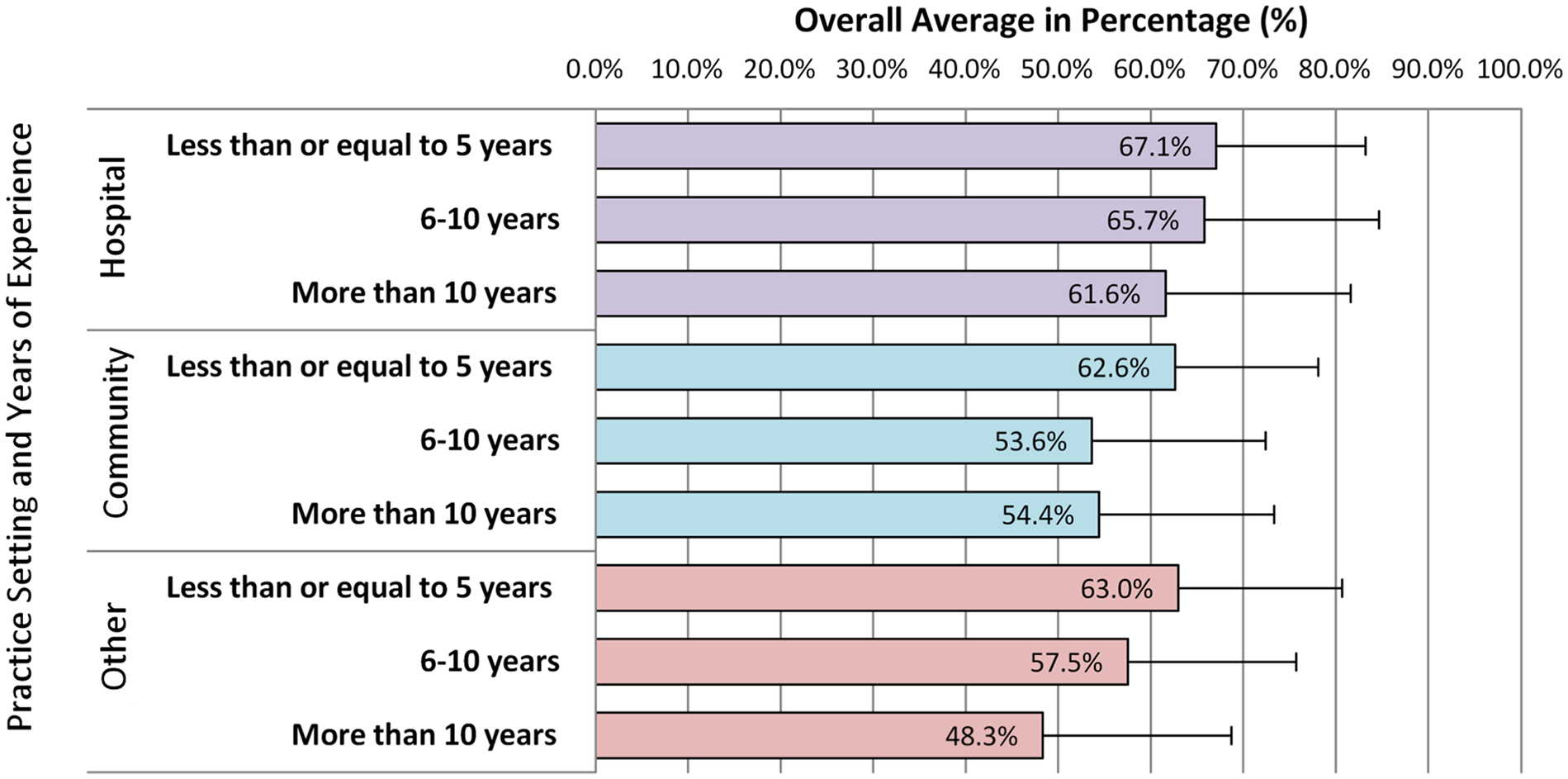
Average overall knowledge score of pharmacists stratified by practice setting and years of experience.
Greater experience in neurology-related practice was also associated with higher odds of scoring >50% (OR = 2.18, 95% CI = 1.09-4.34, P = 0.027). Figure 4 summarizes the average score based on extent of previous neurology experience. Participants who reported no neurology experience or those with experience limited to undergraduate rotations displayed the lowest average score (56%). Contrarily, those who reported greater than 2 years of experience in neurology-related practice had the highest average score (73%).
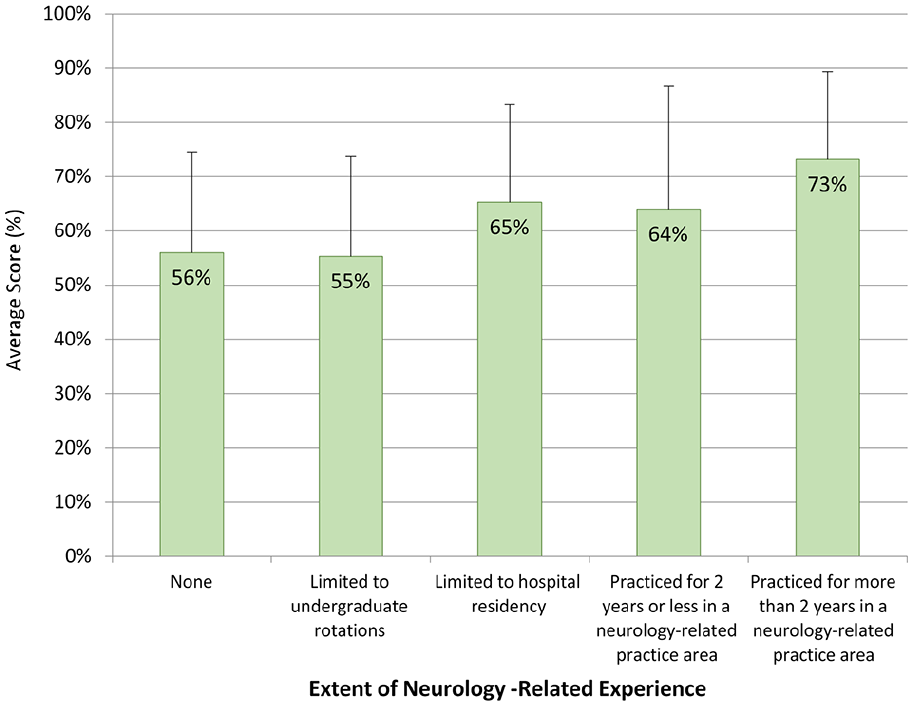
Average score on knowledge questions stratified by years of neurology-related experience.
Needs Assessment
Many participants selected multiple learning areas and reported interest in various tools to support their practice. Figure 5 summarizes the responses from the 2 select-all-that-apply questions used to conduct a needs assessment. Almost one-third of the respondents indicated an interest in learning specifics about initiating and monitoring AED (30%). In the free text for “other,” participants suggested a need for resources addressing withdrawal of AED and TDM. Few participants requested resources to learn about types of seizures and AED of choice for each. Among the option tools listed, nearly a third of the participants indicated a need for pocket summary tools (31%) and access to resources at place of work (28%). Among participants who selected “other,” some requested accredited continuing education courses to further their learning. In a free-text section at the end of the survey, many participants commented on a significant need to refresh their knowledge, lack of knowledge about types of seizures, and need for effective resources to support their practice.
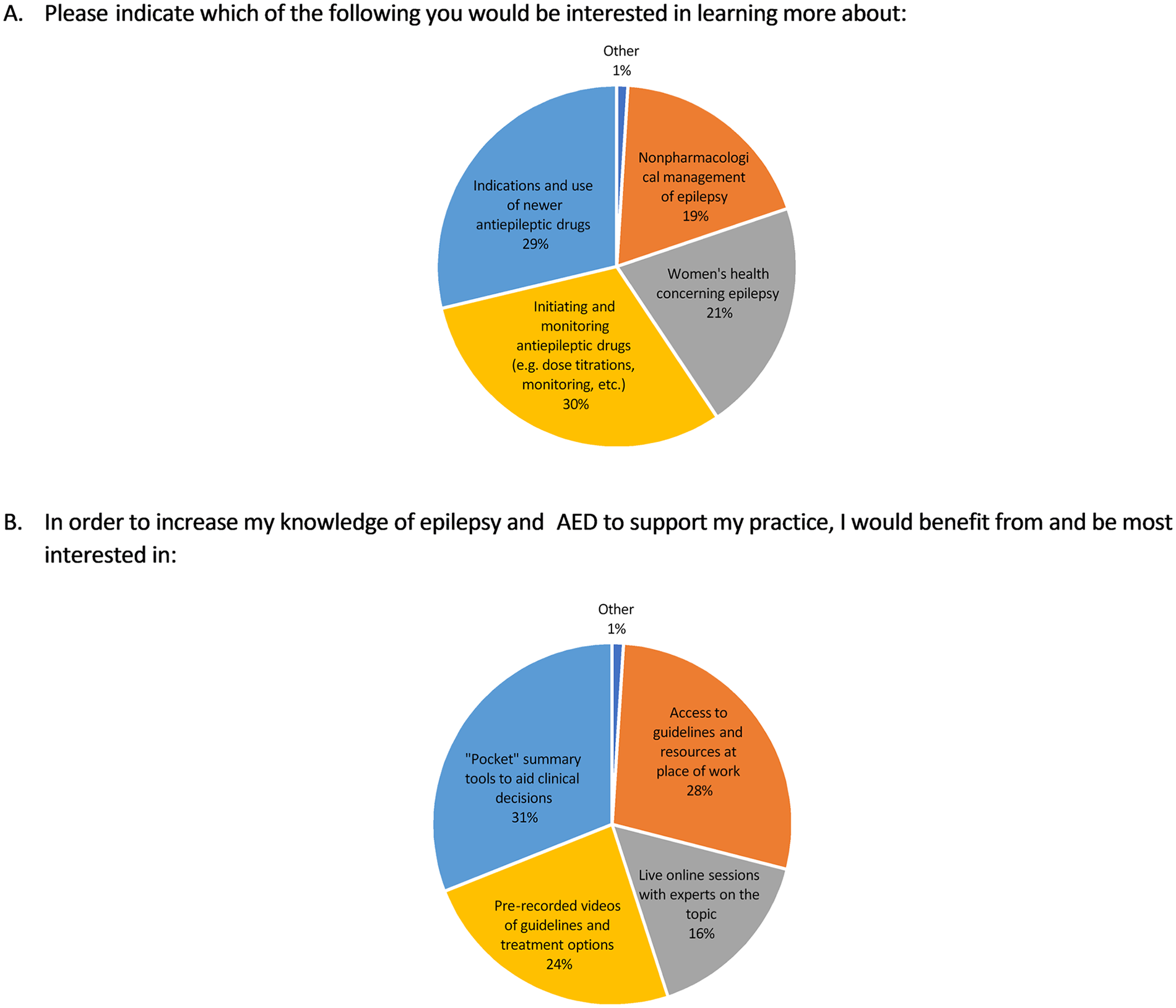
Canadian pharmacists’ epilepsy management needs assessment.
Discussion
As one of the most accessible health care providers, pharmacists play an important role in providing education about AED, identifying therapy-related problems, and managing burden of adverse effects. 11 Therefore, it is important to consider pharmacists’ level of comfort and knowledge in the management of epilepsy and AED therapy. To our knowledge, this is the first study conducted in Canada to characterize pharmacists’ comfort and knowledge of epilepsy management and has the highest number of responses to date in comparison with similar studies. Our survey identified various gaps in the management of epilepsy by pharmacists. First, the majority of pharmacists indicated low comfort in skills such as TDM and AED withdrawal. Higher scores on the knowledge component of the survey were associated with less than 5 years of practice experience, hospital practice, greater neurology-related experience, and male sex. Lowest scores were seen on questions more specific to epilepsy therapies such as generic substitutions, pregnancy dosing, and TDM. Overall, our study indicated a significant need for educational support tools.
Certain areas of higher comfort were identified in our study. As expected, counseling, checking prescriptions, and answering questions related to AED were rated high in comfort. Conversely, comfort levels for skills that require more knowledge and are more specialized to epilepsy management, such as TDM and AED withdrawal, were rated very poorly. In addition, although 68% of pharmacists were aware of potential AED withdrawal with prolonged seizure freedom, only 31% reported being comfortable managing patients withdrawing or tapering from therapy while on concomitant AED. These findings imply a significant disconnect between awareness and skill, and demonstrate a need for educational intervention addressing TDM and AED withdrawal guidelines.
The total average score of 57.6% by the participants indicated poor overall knowledge of epilepsy management. Our average score is similar to, or slightly higher than, prior studies evaluating similar parameters among health care professionals.7-10,12 Certain areas of management were identified as particular areas of concern. To illustrate, despite its potentially harmful effects for myoclonic seizures, only 22% of the participants selected carbamazepine as a potentially ineffective choice for myoclonic seizures. In addition, as pharmacists play a significant role in the monitoring of chronic medications, it is prudent, both clinically and economically, that pharmacists be aware of TDM indications. However, this skill was not evident in our findings as only 39% of the respondents were aware that routine TDM of AED is not recommended.
Certain high-scoring areas of management were identified. Although only 44% of the participants were aware of changes in pharmacokinetics related to dosing in pregnancy, a notably higher portion were aware of the importance of folic acid supplementation for women of childbearing potential (82%) and the significance of proper sleep in managing seizure threshold (95%). These high-knowledge areas identified by our study are consistent with prior studies evaluating the knowledge of women’s health 9 and general epilepsy management.10,12 Of note, the aforementioned higher scoring questions were more likely to be True/False questions, likely due to the limited choices and contextual interpretations of the statement. Contrary to a similar study by Roth et al., where less than 20% of the participants were aware of the urgency of a lamotrigine rash, our findings indicated higher awareness among pharmacists for an urgent physician referral upon lamotrigine rash occurrence (72%). 7 This result is similar to the findings of Shawahna et al. in which 67% of the participating pharmacists recognized the lamotrigine rash as an urgent referral. 10
Experience of less than 5 years in practice was associated with higher overall scores, a result correspondent with that of (Roth et al., 2016). The lower scores in pharmacists practicing for a longer duration may be explained by the changes in pharmacy curriculum and lack of resources in epilepsy management, and indicates a need for a further refresher. Interestingly, the number of patients with epilepsy seen monthly was not associated with higher scores, similar to findings noted in a study evaluating epilepsy knowledge of pharmacists in Ohio and contrasting to Shawahna et al., where the number of patients with epilepsy seen was directly correlated with higher scores.9,10 In addition, pharmacists practicing in hospital scored higher compared with their community counterparts. Increased familiarity with TDM and increased availability of resources at hospitals may be responsible for the difference. As expected, greater neurology-related experience was correlated with higher scores due to increased exposure and knowledge of epilepsy. Interestingly, contrary to other similar studies, our study identified male sex as a statistically significant predictor of higher scores. However, the degree to which participants’ sex independently contributes to higher scores is unclear.7,10,12
Low comfort and knowledge scores, as well as an indicated interest in further learning, depict a clear need for educational intervention. In addition, many participants selected “I don’t know” on several questions, demonstrating direct gaps in knowledge. Our findings addressing the need for educational tools are correspondent to several other studies.7-10,12 Based on the low scoring questions, identified comfort gaps, and needs assessment analysis, we identified the following topics that require further learning: TDM recommendations, AED withdrawal guides, AED use in pregnancy, appropriate AED based on seizure types, an overview of newer AED, and monitoring parameters for AED. As many participants indicated that they would benefit from pocket summaries, credited continuing education courses, and resources at work, we recommend epilepsy summary tools be developed. Specifically, quick reference guides, as seen in other chronic health conditions such as diabetes or online modules around epilepsy management, would be particularly of benefit.
Study Limitations
Some limitations, such as selection bias, a lack of validation for the survey, and caution with generalizability to all provinces should be noted. Access to directly inviting pharmacists from all provinces was limited, and thus, more than 90% of the respondents were from Ontario and Alberta. This reduces the generalizability of the results to pharmacists practicing in other provinces with few or no participants. Furthermore, the survey was available in only English, potentially creating a language barrier for French-speaking pharmacists. Although the survey was developed based on evidence-based guidelines, it was not validated through external parties. In addition, it is difficult to create comparisons of some of our results with other studies due to a lack of research directly measuring pharmacists’ comfort in epilepsy management.
Conclusion
Our study demonstrates that although pharmacists practicing in Canada displayed comfort and knowledge in certain aspects of epilepsy management, significant knowledge gaps exist in more specialized aspects of epilepsy and AED management. As pharmacists are involved in the dispensing and monitoring of AED therapies, these knowledge gaps must be addressed to optimize clinical outcomes. We suggest that educational tools such as pocket guidelines and online modules should be developed to further promote learning and best practice around epilepsy management. Future studies aimed at developing epilepsy support tools are needed.
Footnotes
Appendix
Author Contributions
A.C. participated in study design, data analysis, and interpretation of results; wrote the first draft of the manuscript; and revised and approved the final draft for publication. S.H.M. conceived the study and its design, initiated the project, obtained ethics approval, participated in data analysis and interpretation of results, and revised and approved the final draft for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Faculty of Pharmacy and Pharmaceutical Sciences, University of Alberta (Start-up award for Dr. S.H.M). The funding source had no role in the study design; collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.