
Abstract
Purpose
To provide a review of randomized controlled trials (RCTs) on the efficacy and safety of zonisamide as an adjunctive treatment for partial-onset seizures in epilepsy patients ages 12 years and above.
Methods
Medline literature search for published double-blind RCTs involving zonisamide as adjunctive treatment for simple partial, complex partial, and secondarily generalized tonic-clonic seizures.
Results
Four RCTs comprising a total of 841 patients with medically-intractable simple partial, complex partial and secondarily generalized tonic-clonic seizures were published between the years 1993 and 2005. Zonisamide doses included 0, 100, 300, 400, 500 and 600 mg/day. Median change in frequency of all partial seizures compared to baseline was a 26.9%–51.3% decrease at zonisamide doses of 400–600 mg/day compared to a 4.7% increase to 18.1% decrease with placebo. Responder rates (>50% reduction) for all partial seizures was 26.9%–52.5% for zonisamide at these doses versus 9.8%–22% reduction for placebo. A dose-response relationship was noted up to 500 mg/day. Seizure free rates during the double blind treatment phases were 5%–6.2% for full-dose zonisamide versus 2% for placebo in two of the RCTs. Side effects were mostly CNS in type: somnolence, fatigue, dizziness and ataxia. Mild weight loss and anorexia were reported. Symptomatic renal calculi and serious rashes were not reported, but a few cases of possible stones seen transiently on ultrasound occurred, in these 4 RCTs. Four deaths occurred: none were taking zonisamide, and two appeared to be related to suffocation during seizures. Suicidal ideation and behavior occurred equally in placebo- and ZNS-treated subjects. Post-approval information suggests the rare occurrences of metabolic acidosis, oligohydrosis and hyperthermia, more commonly in children.
Conclusion
Zonisamide at a daily dose up to 600 mg is effective and generally well tolerated as adjunctive therapy in adolescents and adults with refractory partial-onset seizures.
Introduction
Zonisamide (ZNS), 3-sulfamoylmethyl-1,2-benzisoxazole (C8H8N2O3S), is a non-arylamine sulfonamide derivative which was developed by Dainippon Pharmaceuticals Limited of Japan, Parke-Davis Pharmaceuticals of the USA and Elan Pharmaceuticals of Ireland. It is in a class different from arylamine sulfonamide antibiotics such as sulfamethoxazole. ZNS is a white powder with a pKa = 10.2 which is moderately soluble in water (0.8 mg/mL) and 0.1 N HCl (0.5 mg/mL).
Indications
ZNS has been marketed in Japan under the trade name Exegran™ since 1989 and in South Korea for many years for the treatment of children and adults with partial-onset (simple partial, complex partial [CPS] and secondarily generalized tonic clonic) seizures and for generalized-onset (tonic, tonic-clonic, and absence) seizures. Zonisamide was approved by the United States Food and Drug Administration (FDA) on March 28, 2000 and by the United Kingdom for treatment of partial seizures with or without secondary generalization to tonic-clonic seizures (GTCS) in adults. It is marketed in the U.S., Asia and Europe by Eisai Pharmaceuticals under the brand name Zone-gran™. ZNS is also available in a generic formulation in some countries.
Mechanisms of action
The drug's anti-seizure properties may be due to multiple mechanisms of action. In vitro pharmacological studies indicated that ZNS blocks abnormal rapid repetitive opening of voltage-gated sodium channels 1 and voltage-dependent transient inward T-type calcium channels, 2 possibly stabilizing neuron membranes and suppressing neuronal hyper-synchronization. ZNS causes reduction of glutamate-mediated synaptic excitation 3 and alteration of monoamine (dopaminergic and serotonergic) neurotransmission.4,5 In vitro binding studies have demonstrated that zonisamide binds to the gamma-aminobutyric acid (GABA)/benzodiazepine receptor ionophore complex in an allosteric fashion, but this does not appear to produce changes in chloride flux or potentiate GABA synaptic activity. It may protect neurons from free radical damage by increasing the scavenging of hydroxyl and nitric oxide radicals in a dose-dependent manner.8,9 Zonisamide has mild carbonic anhydrase inhibiting effects, similar to the antiepileptic drugs acetazolamide and topiramate, but this effect is not felt to be a major contributor to its mechanism of action.
Although, the exact mechanism(s) by which ZNS exerts its anti-seizure effects in humans is unknown, it has demonstrated antiepileptic effects in several experimental models. In animals, ZNS was effective against tonic extension seizures induced by maximal electroshock, a model of GTCS. It was ineffective against the seizures induced by subcutaneous pentylenetetrazol, a model of absence seizures. ZNS raises the threshold for generalized seizures in the kindled rat, a model for partial-onset epilepsy especially of temporal lobe origin. It also reduces the duration of cortical focal seizures induced by electrical stimulation of the visual cortex in cats. Finally, ZNS suppresses both interictal spikes and the secondarily generalized seizures produced by cortical application or tungstic acid gel in rats or by cortical freezing in cats. However, the precise relevance of these animal models to the many varieties of naturally-occurring human epilepsy syndromes remains to be determined.
Pharmacokinetics
Following a single ZNS dose, peak plasma concentrations occur within 2–6 hours. In the presence of food, the time to maximum concentration is delayed; occurring at 4–6 hours. However, food has no effect on the bioavailability of ZNS. Zonisamide extensively binds to erythrocytes, resulting in an eight-fold higher concentration of ZNS in red blood cells than in plasma. The pharmacokinetics of zonisamide are dose proportional in the range of 200–400 mg/day, but the Cmax and AUC increase disproportionately at 800 mg, perhaps due to saturable binding of zonisamide to red blood cells. Once a stable dose is reached, steady state is achieved within 14 days.
ZNS is hepatically-metabolized via CYP 3A4 reduction to the glucuronide of the open-ring metabolite 2-sulfamoylacetyl phenol (SMAP) followed by enzymatic hydrolysis. ZNS is excreted primarily in urine as parent drug and as SMAP, The elimination half-life of ZNS in plasma is (T½) is approximately 63 hours in monotherapy, 27 and 38 hours when taken with enzyme-inducing antiepileptic drugs phenytoin and carbamazepine respectively, and 46 hours when used adjunctively with valproic acid. ZNS does not induce its own metabolism, or inhibit or induce cytochrome P450 enzymes. The elimination half-life of ZNS in RBCs is approximately 105 hours. Twice daily dosing results in approximately 14% fluctuation in plasma levels, whereas once daily dosing results in a 27% fluctuation. It is approximately 40% bound to human plasma proteins. The percentage protein binding is unaffected by therapeutic concentrations of phenytoin, phenobarbital or carbamazepine. Marked renal impairment produces a 35% increase in the ZNS area under the curve. Its pharmacokinetics has not been studied in hepatic failure. In preclinical trials the median steady state near-trough plasma concentration was approximately 18 mcg/mL, but the useful range is likely to be 10–40 mcg/mL.
Dosing
The usual dose for adults is 400–600 mg/day, starting at 100 mg/d. It is reasonable to increase the dose by 100 mg/day every 2 weeks or longer due to its long half-life. Doses up to 600 mg/day have been effective, but the dose-ranging randomized-controlled trials described below provide no evidence of increased effect above 500 mg/day.
Adverse effects
If the dose is escalated quickly, there is a 20% incidence of CNS side effects. The most common adverse effects (AEs) in randomized controlled trials (RCTs) were somnolence, dizziness, fatigue, nausea, anorexia, rhinitis, ataxia, headache, weight loss, agitation, irritability, psychomotor slowing, difficulty with concentration, speech difficulties, depression, and psychosis. In 2009 the U.S. FDA issued a warning of increased risk of suicidal ideation in association with every type of AED. Because ZNS is a sulfonamide, it is contra-indicated in patients who have hypersensitivity to sulfonamides or to zonisamide, or who have a history of conditions which can be worsened by sulfonamides. Fatalities have occurred, although rarely, as a result of severe reactions including Stevens Johnson Syndrome, toxic epidermal necrolysis, fulminant hepatic necrosis agranulocytosis, aplastic anemia, and other blood dyscrasias. There is a 1.2% incidence of symptomatic renal stones, so consumption of 6–8 glasses of water per day is recommended. ZNS can cause metabolic acidosis characterized by hyperchloremia and decreased serum bicarbonate. This can result in hyperventilation, and non-specific symptoms such as fatigue and anorexia, or more severe symptoms including cardiac dysrhythmias or stupor. Chronic metabolic acidosis can have adverse effects on the kidneys and on the bones and growth retardation in children. The risk of ZNS-induced metabolic acidosis appears to be more frequent and severe in younger patients. It generally occurs early in treatment, but may occur at any time. Conditions which may predispose to ZNS-induced metabolic acidosis include renal disease, severe respiratory disorders, diarrhea, surgery, ketogenic diet and certain other drugs like acetazolamide. Finally, ZNS is associated with a low incidence of decreased sweating (oligohydrosis) and hyperthermia. In the first 11 years of marketing in Japan, 38 cases were reported yielding an estimated reporting rate of about 1 case per 10,000 patient-years of exposure. Oligohydrosis and hyperthermia are more common in children.
Effectiveness against Partial-onset Seizures in Randomized Controlled Trials
Four RCTs comprising a total of 841 patients with medically-intractable simple partial, complex partial and secondarily generalized tonic-clonic seizures were published between the years 1993 and 2005. Zonisamide doses included 0, 100, 300, 400, 500 and 600 mg/day. Median change in frequency of all partial seizures compared to baseline was a 26.9%–51.3% decrease at zonisamide doses of 400–600 mg/day compared to a 4.7% increase to a 18.1% decrease with placebo. Responder rates (>50% reduction) for all partial seizures was 26.9%–52.5% for zonisamide at these doses versus 9.8%–22.0% reduction for placebo. In the two dose-ranging RCTs a dose-response relationship was noted up to 500 mg/day. Seizure free rates during the double blind treatment phases were 5%–6.2% versus 2% for placebo in two of the RCTs. Side effects were mostly central nervous system in type: somnolence, fatigue, dizziness and ataxia. Mild weight loss and anorexia were reported. Symptomatic renal calculi and serious rashes were not reported, but a few cases of possible stones seen on ultrasound were observed, in these 4 RCTs. Four deaths occurred; all were receiving placebo, and two appeared to be related to suffocation during seizures. Suicidal ideation or behavior was reported equally in placebo- and zonisamide-treated subjects.
ZNS 912 EU Trial
The ZNS 912 EU Trial was a randomized, placebo-controlled, double-blind, nine-center, European dose-response study designed to assess the efficacy of ZNS as adjunctive therapy for patients with partial-onset intractable epilepsy. 10 One hundred thirty nine Caucasian adults aged 18–59 years had a median rate of 10 complex partial seizures per month during the 4 months prior to enrollment despite taking 1–3 concomitant AEDs (mostly carbamazepine, phenytoin, phenobarbital, and primidone). Mean duration of epilepsy was approximately 22 years. The baseline phase lasted 8–12 weeks. Initial ZNS dose was 1.5 mg/kg/day and was planned to increase on advice of an un-blinded investigator to achieve a plasma concentration of 20–30 mcg/ml. If seizure frequency was not decreased by at least 50%, then the dose was planned to increase up to a maximum of 20 mg/kg/day or to a plasma concentration of 40 mcg/kg/day provided that no unacceptable side effects occurred. ZNS was actually raised to a dose of 7.0 +/- 2.6 mg/kg/day (approximately 500 mg/day for a 70 kg person) by day 84 of the study. Analysis was by intent-to-treat, based on the data of all subjects who completed at least one week of treatment (n = 67 zonisamide, 64 placebo).
At full dose, there was a complex partial seizure median reduction of 27.7% for zonisamide and increase of 3.9% for placebo. All partial-onset seizures showed a median decrease of 26.9% for ZNS and increase of 3.9% for placebo (Fig. 1). The percent of patients achieving at least a 50% reduction (responder rate) in complex partial seizures was 30.3% and 12.7% for ZNS and placebo, respectively, and for all partial seizures was 30.3% and 10.9% respectively. It appears that 5 ZNS and 2 placebo patients became seizure-free during treatment. The median plasma concentration during month 3 was approximately 16 mcg/mL.
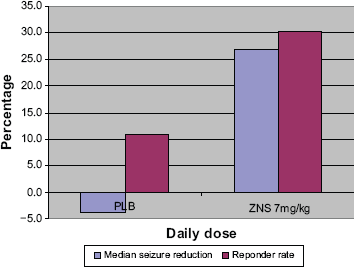
ZNS 912 EU RCT–-All partial seizures.
During the 12-week double-blind treatment phase 59% of patients receiving ZNS and 28% receiving placebo reported AEs. The most common AEs were fatigue, dizziness, somnolence, anorexia, abnormal thinking, confusion and ataxia. No symptomatic renal calculi were observed. Rash was not reported. Serum chloride levels increased by 3.0 mmol/L for ZNS and 1.0 mmol/L for placebo.
ZNS 922 trial
The ZNS 922 Trial was a randomized, placebo-controlled, double-blind, multicenter, United States dose-response study performed to assess the efficacy of ZNS at a dose of 100, 200 and 400 mg/day, and to determine safety and tolerability in people ages 12 years and older with partial-onset seizures. 11 Patients were required to have at least 4 simple partial motor, complex partial, or secondarily GTC seizures per month for 3 months prior to randomization. Patients were required to be on 1–2 baseline AEDs, one of which had to be phenytoin, carbamazepine, valproate, phenobarbital or primidone. Doses of concomitant AEDs were held constant during the study.
The initial 4-week baseline observation period, during which patients were required to have at least 4 partial-onset seizures, was followed by a 20-week double-blind treatment period. Subjects were divided into 3 groups: groups A, B1 and B2. Group A continued on placebo for 12 weeks then began zonisamide and titrated up to 400 mg/day and remained at that dose for 5 weeks. Group B1 was randomized to 100 mg/day for 5 weeks, and then titrated up to 400 mg/day for weeks 8–20. Group B2 titrated up to 200 mg/day by week 2, remained at that dose for 5 more weeks, and then titrated up to 400 mg/day for weeks 8–20. Renal ultrasonograms were obtained at entry, at week 12, and on withdrawal from the study. The primary efficacy outcome variable was the median percentage reduction in seizure frequency during weeks 8–12 in all 3 groups compared to their 4-week baseline frequency. Changes from baseline seizure frequency were also assessed for group B1 during weeks 1–5 (ZNS 100 mg/day) and for group B2 during weeks 1–6 (200 mg/day) compared to the change seen in the group A (placebo). Also, the change in seizure rate for Group A from baseline to weeks 16–20 (400 mg/day) was assessed. The secondary efficacy outcome variable was the responder rate (percentage of patients achieving a 50% or greater reduction in seizures).
Two hundred three patients were randomized and 146 (72%) completed the trial. Analysis was by intent-to-treat, modified intent-to-treat (those receiving at least one dose of study medication), and per-protocol. For the modified intent-to-treat population, ZNS at 400 mg/day produced a 40.5% median reduction in all seizures compared with only a 9% reduction for placebo, and a 43% responder rate for all seizures compared with a 22% responder rate for placebo (Fig. 2). Group A patients who crossed over from placebo to 400 mg/day (weeks 17–20) had a median reduction of 40.1% for all seizures and 55% for complex partial seizures compared with their placebo-controlled baseline rate. Seizure control was dose-dependent. The median reduction in frequency of all seizures for the 100 mg/day group was 24.7% for ZNS versus 8.3% for placebo. In the 200 mg/day group, reduction in all seizures was 20.4% for ZNS versus 4.0% for placebo. Responder rates were similar at these intermediate doses (Fig. 2). All these reductions for ZNS were statistically-significant compared to placebo (p < 0.05). When subjects were taking 400 mg/day, seizure concentrations for all groups were 16.5–21.3 mcg/mL. ZNS concentrations at 400 mg/day were not significantly different between responders and non-responders.
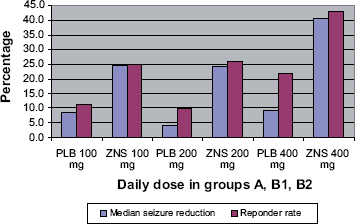
ZNS 922 RCT–-All partial seizures.
Patients withdrawing after exposure to medication were 10% for ZNS and 8% for placebo (no significant difference). Withdrawals for other reasons were equally distributed between the blinded ZNS and placebo groups. Rash occurred in one patient receiving placebo, and none taking zonisamide. No patients had symptomatic renal calculi in the 20-week study. On initial ultrasonograms, kidney stones were suggested in 4 subjects, but on follow-up renal ultrasound examintions no evidence of stone formation was found in any subject.
ZNS 912 US trial
The ZNS 912 US Trial was a randomized, placebo-controlled, double-blind, multicenter, dose-response study conducted in the U.S. to assess the efficacy, safety and tolerability of ZNS as adjunctive therapy for partial-onset seizures at a dose of 400–600 mg/day. 12 Subjects between ages 17 and 65 years were eligible if they had a history of at least 4 complex partial, and no more than 8 generalized tonic-clonic, seizures per month. They were required to be receiving at least one, but not more than two, of the following AEDs: carbamazepine, phenobarbital, phenytoin and primidone. There were several exclusion criteria, including sulfonamide sensitivity, glucose-6-phosphate dehydrogenase deficiency, a history of hemolytic anemia or acute intermittent porphyria. Initial ZNS doses were 400 mg/day for patients weighing ≤60 kg, 500 mg/day for patients weighing 61–70 kg, and 600 mg/day for patients weighing ≥71 kg. The daily ZNS dose was divided and given every 12 hours, and it was adjusted as necessary by a non-blinded observer based on plasma levels to obtain concentrations of 20–30 mcg/mL. The non-blinded observer ensured that the ZNS dose did not exceed 20 mg/kg/day and that plasma concentrations did not exceed 40 mcg/mL.
The primary efficacy outcome variable was the median percentage reduction in all partial-onset seizure frequency during weeks 5–12 of the treatment phase relative to baseline seizure frequency. The secondary efficacy outcome variable was the responder rate. One hundred fifty-two patients were enrolled during the baseline phase of the study and all were randomized. One hundred thirty-one patients, 82% in the ZNS group and 91% in the placebo group, completed the trial. The final dosage was <400 mg/day for 34.6% of patients, and ≥400 mg/day for 65.3% of patients. With regard to all partial seizures, the median change in seizure frequency with treatment compared to baseline was an increase of 4.7% for placebo and a decrease of 28.9% for ZNS (Fig. 3). This difference was significant (p = 0.0009). Surprisingly, although the responder rate was higher for the ZNS than for placebo (26.9% vs. 16.2% respectively), the difference did not reach statistical significance (p = 0.0796). The final median dosage of ZNS for responders was 500 mg/day or 6.4 mg/kg/day with a plasma level of 14.2 mcg/mL. These were all slightly higher than the corresponding doses and level in non-responders.
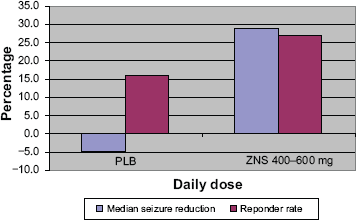
ZNS 912 US RCT–-All partial seizures.
The most commonly reported AEs were somnolence irritability, dizziness, nausea and fatigue. Mild treatment-emergent AEs were reported in 21.8% of ZNS subjects and 27.0% of placebo patients. Moderate severity AEs were reported in 38.5% of ZNS and 23.0% of placebo patients. 12 patients on ZNS and 1 subject receiving placebo withdrew due to AEs. Faster dose titration and higher doses were associated with greater incidence of AEs. One patient, randomized to placebo, died apparently due to a seizure. Four placebo patients had potentially serious AEs: one each experienced suicidal behavior, neoplasm, thrombosis, and psychosis. Eight ZNS-treated patients experienced 11 potentially serious AEs: depression, jaundice, stroke, psychosis, insomnia, anxiety, tachycardia, cholecystitis, suicidal behavior and intentional overdose. No clinically-significant changes in laboratory values or ECG were seen. With ZNS, there was a mean of 3 kg weight loss compared with a placebo group mean 0.4 kg increase in body weight during this 12-week trial.
ZNS 920 trial
The final study was a randomized, placebo-controlled, double-blind, 54-center, dose-response study conducted in Europe and South Africa. 13 It was designed to assess the effectiveness and safety of adjunctive ZNS at 100, 300 and 500 mg/day, and to determine if a dose-response relationship existed. Inclusion criteria included: age at least 12 years, partial-onset seizures, and a stable regimen of 1–3 concomitant AEDs. Patients were required to have at least 12 partial-onset seizures during a 12-week prospective baseline period. A total of 351 patients were randomized in a 2:1:1:2 ratio to placebo, or to ZNS at 100, 300, or 500 mg/day (given twice daily) respectively. Up-titration of study medication occurred over 6 weeks, and then patients entered an 18-week fixed dose maintenance phase.
The two primary efficacy endpoints were the median percentage change in CPS between baseline and the fixed-dose assessment phase, and the 50% responder rate for CPS. Secondary efficacy variables were median percentage changes in simple and complex partial seizures, changes in all seizure types, and the number of seizure-free days per 28-day period. All patients who received at least one dose of ZNS were included in the safety analysis. Primary and secondary efficacy variables were assessed in three groups: the intent-to-treat population (ITT; all patients who received at least one dose of ZNS and who had any post-baseline partial seizure frequency data), the primary efficacy-analysis population (all patients in the ITT population with partial seizure frequency data collected during the fixed-dose assessment phase), and the efficacy-evaluable population (all ITT patients who averaged 4 seizures/month during baseline and who took at least 10 weeks of study medication including at least 2 weeks from the fixed-dose assessment phase). The primary efficacy analysis was conducted using the primary efficacy-analysis population. Three hundred fifty one patients were randomized in the 2:1:1:2 ratio, and 349 received at least one dose of study drug. The ITT population was comprised of 347 subjects. The primary efficacy-analysis population had 312 patients, and the efficacy-evaluable population had 294 subjects. Three quarters of patients were taking at least 2 concomitant AEDs. The most common concomitant AEDs at baseline were carbamazepine, divalproex, and lamotrigine. Most patients in each treatment group at baseline were taking an enzyme-inducing AED.
Primary efficacy-analysis population
For the primary efficacy-analysis population, during the fixed-dose assessment phase, treatment with ZNS at 500 mg/day produced a significantly greater (p < 0.0001) median reduction in all-seizure frequency from baseline than did placebo [51.3% (n = 101) vs. 18.1% (n = 112); (Fig. 4)]. Also, ZNS at 300 mg/day showed a significant reduction [41.8% (n = 45); p = 0.0005] in all-seizure frequency compared to placebo. In the same population, the responder rate for all seizures was higher in each ZNS group (500 mg/day, 52.5%; 300 mg, 42.2%; 100 mg, 29.6%) than for placebo (17.9%; Fig. 4). Likewise, treatment with ZNS at 500 mg/day produced a significantly greater (p < 0.0001) median reduction in CPS frequency from baseline than did placebo [51.2% (n = 86) vs. 16.3% (n = 89)]. In the same population, the responder rate for CPS was significantly higher (p < 0.001) in the ZNS 500 mg/day group compared with placebo (52.3 vs. 21.3%).
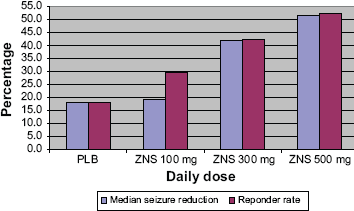
ZNS 920 RCT–-All partial seizures.
Intent-to-treat population
For the ITT population for all seizures, the median percent reduction from baseline was significantly greater than placebo [17.4% (n = 119)] for both ZNS 500 mg/day [46.1% (n = 118); p < 0.0001] and 300 mg/day [38.5% (n = 55); p 0.0034], but was not significantly greater than placebo for the 100 mg/day ZNS group. The responder rate for all seizures was higher in each ZNS treatment group (500 mg, 46.6%; 300 mg, 34.5%; 100 mg, 30.9%) than for placebo (17.6%). In this population, ZNS treatment at 500 mg/day produced a significantly greater reduction in CPS from baseline than did placebo [44.1% (n = 102) vs. 16.9% (n = 94),and the responder rate for CPS was likewise significantly greater (p < 0.001) for ZNS 500 mg/day than placebo (45.1% vs. 22.3%). The percentage of responders showed an apparent dose-response relation for all seizures, for SPS + CPS, and for CPS in the ITT population. Six patients (5%) treated with ZNS,500 mg/day, and two (2%) treated with placebo were free of all seizures during the 24 weeks of the combined titration and fixed-dose maintenance phases of the study. Worsening of the frequency of all seizures by >25% was observed in the ITT population in 6%,7%,and 9% of patients treated with ZNS, 500, 300,and 100 mg/day, respectively, compared with 16% of subjects given placebo.
Efficacy-evaluable population
During the fixed-dose maintenance phase, treatment with 500 mg/day of ZNS produced as significantly greater median reduction of CPS frequency from baseline than did placebo [49.8% (n = 74) vs. 16.4% (n = 86)] for the efficacy-evaluable population. The responder rate for CPS was significantly higher (p < 0.001) in the ZNS 500 mg/day group compared with placebo (50.0% vs. 20.9%).
Most patients (68.3%) in the placebo group reported one or more AE. For the 100, 300 and 500 mg/day dose groups, 67.9%, 70.9% and 81.4% of patients reported any adverse effect, respectively. The majority of AEs in each treatment group were of mild to moderate severity. Serious AEs occurred in nearly equal numbers in the placebo and all three ZNS dose groups (0%–9.1%). One patient died before receiving the first dose of study medication. Two patients, both in the placebo group, died of causes considered by the investigator to be unrelated to treatment (suffocation during an epileptic seizure and unknown cause of death). Withdrawals due to AEs occurred in 10%, 1.8%, 18.2%, and 27.1% of the placebo and ZNS 100, 300 and 500 mg/day groups, respectively. Common AEs (defined as ≥10% of subjects in any group) included dizziness, difficulty concentrating, nausea, somnolence, and headache during the titration phase, and pharyngitis during the maintenance phase. At the end of the 18-week maintenance phase of the study, weight changes were a mean 0.2 kg gain for placebo, 1.0 kg loss for 100 mg/day, 0.1 kg gain for 300 mg/day, and 1.7 kg loss for 500 mg/day subjects.
Discussion
The results from each of these four pivotal RCTs examining ZNS as adjunctive treatment for partial onset seizures showed that ZNS at a dose of 400–600 mg/day (given twice daily) is significantly superior to placebo in reducing the median percentage of all seizures and CPS from baseline to treatment phases, and in increasing the proportion of patients who are responders. Evidence of a dose-response relationship, up to a total of 500 mg/day was shown in the ZNS 920 and 922 studies. Median percent change in all seizures ranged from a 4.7% worsening to an 18.1% improvement for placebo-treated subjects, and a 26.9 to 51.3% improvement for 400–500 mg/day patients, across the four studies. A small, but greater, percentage of patients were seizure-free during the maintenance phases of these studies who were receiving the highest dose of ZNS than those who were receiving placebo. In the ZNS 920 study, more than twice as many patients receiving placebo had a >25% worsening of seizure frequency than did subjects receiving 500 mg/day of ZNS.
ZNS has a long half-life of about 63 hours in plasma or serum in healthy volunteers. The half-life falls by about half in the presence of classical CYP 450 enzyme-inducing AEDs, such as phenytoin, carbamazepine and phenobarbital/primidone, and by about one-third in the presence of valproate. These four pivotal RCTs were conducted a number of years ago when the main concomitant AEDs were these older drugs. One wonders what would be the efficacy and AE results if these studies were conducted using cytochrome P-450 enzyme non-inducting AEDs such as are much more commonly used today. Likewise, it would be of great interest to know how effective and well-tolerated ZNS would be if it were studied in monotherapy, or in patients who were less medically-refractory than were the subjects in these four trials.
In these RCTs, AEs were mostly mild to moderate in degree. They were seen in a higher percentage of patients, proportional to dose. In the ZNS 912 US study, a slow titration of the drug was associated with fewer adverse events than was a faster titration. No deaths were felt to be related to study drug; some occurred in the placebo group or prior to receiving study medication. AEs sometimes seen with ZNS were somnolence, dizziness, fatigue, nausea, anorexia, rhinitis, ataxia, headache, weight loss, anxiety, insomnia, irritability, psychomotor slowing, difficulty with concentration, speech difficulties, depression, and psychosis. No substantial changes in clinical laboratory results or ECGs were reported. Suicidal behavior was seen in both placebo- and ZNS-treated patients in the ZNS 912 US study. Kidney stones, hepatic dysfunctions, blood dyscrasias or rash did not occur in these studies, but have been reported in a small percentage of patients in post-marketing surveillance. Likewise, metabolic acidosis, oligohydrosis and hyperthermia have been observed in post-marketing studies, more commonly in children.
Regulatory approval for adjunctive therapy for zonisamide was granted in many countries based upon these RCTs and some open label and sponsor data. Most neurologists select AED monotherapy for new-onset persons with epilepsy to reduce cost, complexity, drug interactions and adverse effects. Roughly one-third of new onset patients will be refractory to first, second and third monotherapy AED trials. 14 Such patients who are intractable to initial trials of mono-therapy are candidates for adjunctive therapy with AEDs such as zonisamide. Given its lack of major pharmacokinetic interactions with other AEDs, long half-life, proposed mechanisms of action, and generally good tolerability, ZNS should be considered among the agents useful for initial adjunctive therapy for partial-onset seizures.
Conclusion
In summary, zonisamide is a generally effective and safe AED in the modern adjunctive treatment of partial-onset seizures in localization-related epilepsy syndromes.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author reports no conflicts of interest.