
Abstract
Aim:
To determine the prevalence of pulmonary hypertension (PH), identify associated factors, and evaluate outcomes after adenotonsillectomy in children and adolescents with adeno-tonsillar hypertrophy (ATH) in a low-resource setting.
Methods:
We retrospectively analyzed 1500 patients ≤ 20 years undergoing adenotonsillectomy for ATH in Hawassa, Ethiopia (2022-2025). Pulmonary pressure was estimated via tricuspid regurgitation or pulmonary acceleration time; right ventricular function was assessed with TAPSE and RVMPI. Logistic regression identified PH predictors, and the Friedman test compared pre- and 12-week postoperative measurements.
Results:
PH prevalence was 5.9%. Independent predictors included wasting, overweight/obesity, AN ratio > 0.75, daytime mouth breathing, stertor, and obstructive sleep apnea. Among 89 affected patients, 8 had longitudinal and 6 global RV dysfunction. PH and RV dysfunction resolved by 12 weeks post-surgery (P < .001).
Conclusion:
PH affects a subset of children with ATH but is showed significant improvement following adenotonsillectomy, emphasizing early detection and surgical intervention.
Keywords
Introduction
Adenoids and tonsils are lymphoid tissues located at the junction of the respiratory and digestive tracts and function as part of the immune defense. Due to their location, they are continuously exposed to microbial antigens and allergens, which can stimulate an immune response and often lead to their hypertrophy.1,2 Adeno-tonsillar hypertrophy (ATH) refers to the enlargement of lymphoid tissues within Waldeyer’s ring, including the adenoids, palatine tonsils, and lingual tonsils.2,3
Chronic obstruction caused by adeno-tonsillar hypertrophy can have significant adverse effects on both the cardiovascular and pulmonary systems. 4 Pulmonary hypertension and right ventricular (RV) dysfunction were among the commonly reported cardiopulmonary complications.5,6 Previous studies have suggested that adenotonsillectomy have been associated with improvement in PH and RV dysfunction, highlighting the potential clinical benefits of timely surgical intervention.7,8 In pediatric populations, early reversal of PH and RV dysfunction is particularly important because persistent cardiopulmonary strain can lead to long-term morbidity and adverse outcomes.
Although prior research has described the association between ATH and cardiopulmonary complications, most studies have been limited by small sample sizes or single-center designs. Furthermore, there is a notable lack of data from developing countries, including Ethiopia, which makes it difficult to generalize the findings to these populations. Importantly, existing literature often reports prevalence estimates without systematically evaluating predictors of PH or the degree of functional reversibility after adenotonsillectomy.
This study addresses these gaps by assessing the prevalence of PH and RV dysfunction in a large cohort of 1500 children and adolescents with ATH in Ethiopia, identifying clinical and anatomical predictors of PH, and evaluating changes in pulmonary artery pressure and RV function following adenotonsillectomy. By providing a comprehensive analysis of both prevalence and reversibility, this study offers novel insights beyond sample size alone and informs clinical decision-making in resource-limited pediatric populations.
Materials and Methods
Study Area, Period, and Design
This retrospective hospital-based follow-up study was conducted at the RUH ENT Clinic, Hawassa, Ethiopia, from November 1 to December 30, 2025. The study included 1500 children and adolescents who had undergone adenotonsillectomy for ATH between July 1, 2022, and July 1, 2025, whose records were reviewed during the study period. The RUH Clinic provides ENT services for both children and adolescents from the Sidama region, the south region, and the surrounding Oromia region. Surgical services, including adenotonsillectomy, ear and mastoid disease management, were performed by an experienced ENT surgeon with more than a decade of expertise. Two experienced pediatric cardiologists performed echocardiographic evaluations using a GE Vivid T9 echocardiography system with 3- to 6-MHz probes preoperatively for all individuals. For those with preoperative RV dysfunction or pulmonary hypertension, echocardiography was repeated at 6 and 12 weeks postoperatively.
Study Population and Eligibility Criteria
The study included individuals aged ≤ 20 years who underwent adenotonsillectomy for ATH between July 1, 2022 and July 1, 2025. Exclusion criteria included incomplete data on outcome variables, lack of adenotonsillectomy, congenital heart disease, chronic lung disease, anemia, or prior cardiopulmonary conditions that could independently influence pulmonary pressure. The inclusion of whole individuals who fulfilled the inclusion criteria considered the lower prevalence of pulmonary hypertension in children and adolescents with ATH to increase the power of the study.
Variables and Operational Definitions
The dependent variables in this study were pulmonary hypertension (PH) and right ventricular (RV) dysfunction.
Pulmonary hypertension was defined as mean pulmonary artery pressure (mPAP) greater than 20 mmHg. Doppler echocardiography was used to calculate mPAP: both the TR-derived PASP formula and PAT-derived Mahan formula were used to account for variability in prior studies, with the higher value used when TR was traceable, and PAT alone used when TR was non-traceable. While this approach may increase sensitivity for detecting elevated pulmonary pressures, it may reduce specificity and could potentially overestimate PH prevalence; therefore, findings should be interpreted with caution. A sensitivity analysis was conducted to assess the impact of the mPAP estimation method on PH prevalence. Right atrial pressure (RAP) was incorporated into the calculation of mean pulmonary artery pressure (mPAP) in our study and was not disregarded. In pediatric echocardiography, RAP is commonly estimated from inferior vena cava (IVC) size and collapsibility, as pediatric-specific guidelines are lacking. In the study by Malakan Rad et al, adult guideline–based RAP values (3-8 mmHg) were applied in children and validated against invasive measurements. Accordingly, in our study, we applied a representative value of 5 mmHg, an average of the range reported in the aforementioned study, to minimize, although not completely avoid, underestimation of mean pulmonary arterial pressure. To ensure methodological robustness, sensitivity analyses were planned using RAP values of 3 and 8 mmHg, and mPAP was calculated accordingly for comparison. 9
Right ventricular function was assessed using tricuspid annular plane systolic excursion (TAPSE) indexed to body surface area for individuals under 18 years, and right ventricular myocardial performance index (RVMPI).10,11 Longitudinal RV dysfunction was defined as Z-score < −2 SD in children < 18 years and TAPSE < 17 mm in individuals aged 18 to 20 years, while global RV dysfunction was determined using age-specific RVMPI cut-offs (<18 years) or RVMPI > 0.4 in individuals aged 18 to 20 years. 12 The independent variables included demographic and clinical factors such as age, sex, nutritional status, residence, duration of symptoms, tonsillar size graded by Brodsky scale (0-4), adenoid/nasopharyngeal (A/N) ratio, history of intranasal steroid use, types of symptoms, and presence of non-cardiopulmonary complications. Nutritional status was categorized according to WHO standards, with overweight and obesity defined as weight-for-height > +2 SD or > + 3 SD for children under 5 years, and BMI-for-age > +2 SD or >+3 SD for children 5 years and older. Significant adenoid hypertrophy was defined as an A/N ratio greater than 0.75. Obstructive sleep apnea (OSA) was diagnosed clinically using symptom-based criteria due to the unavailability of polysomnography in our setting. In children, diagnosis followed the American Academy of Sleep Medicine pediatric criteria, including habitual snoring; labored, paradoxical, or obstructed breathing during sleep; daytime sleepiness; hyperactivity; behavioral problems; or learning and cognitive difficulties. 13 In adolescents, adults (>18 years) clinical guideline features were applied, including excessive daytime sleepiness, loud snoring, witnessed apneas, or gasping/choking during sleep, corresponding to ≥5 obstructive respiratory events per hour when polysomnography is available. 14 This may have resulted in non-differential misclassification, which could bias associations toward or away from the null, and therefore the magnitude of association should be interpreted cautiously.
Data Collection Techniques and Quality Assurance
Data were collected using a structured questionnaire adapted from previous literature and medical chart reviews. Medical residents collected the data after a 2-day training, under close supervision to ensure accurate interpretation of medical records. A pretest was conducted on 5% of the study population using medical records from individuals diagnosed with ATH who had undergone adenotonsillectomy at Hawassa Comprehensive Specialized Hospital to ensure consistency and data quality.
Data Analysis
Data were entered into EpiInfo-7 for cleaning and exported to STATA version 17 for analysis. Descriptive statistics were performed after testing normality using the Shapiro–Wilk test. Frequencies and percentages were used for categorical variables, while continuous variables were summarized using medians and interquartile ranges due to non-normal distribution. Tables and graphs were used for data presentation. Binary logistic regression was used to assess predictors of pulmonary hypertension. Bivariable analysis was performed for all variables, and those with P < .2 were included in the multivariable model for confounder control. Statistical significance was set at P < .05, and multicollinearity among the independent variables was assessed using the Variance Inflation Factor (VIF). Variables with VIF values greater than 10 were considered highly collinear. Appropriate corrective measures, such as removing 1 of the correlated variables, were then taken to address the issue. Wide confidence intervals observed for some variables, particularly overweight/obese categories, were noted as a limitation due to sparse data. Model fit was assessed using the Hosmer–Lemeshow goodness-of-fit test, which indicated an adequate fit, and discriminative ability was evaluated using the area under the ROC curve, demonstrating good predictive performance. Pulmonary artery pressure, RVMPI, and TAPSE were measured at preoperative, 6-week, and 12-week postoperative time points. Owing to non-normal data distribution, repeated-measures comparisons were conducted using the Friedman test. When significant, post hoc pairwise comparisons were performed using the Wilcoxon signed-rank test with Bonferroni adjustment. Effect sizes were calculated and expressed as differences in medians with corresponding interquartile ranges (IQRs) to enhance interpretability. Missing data were minimal (30 patients) and were handled by case-wise exclusion; the pattern and extent of missingness were examined to ensure it did not bias results.
Procedure
Indication for surgery follows ENT guidelines.15 -17 All patients underwent echocardiographic examination 1 day before surgery. Doppler echocardiography was used to estimate mean pulmonary artery pressure (mPAP). Both the tricuspid regurgitation (TR)–derived pulmonary artery systolic pressure (PASP) method and the pulmonary acceleration time (PAT)–derived Mahan formula were applied. When TR was traceable, mPAP was calculated using both methods, and the higher value was recorded. When TR was not traceable, mPAP was estimated using the PAT-derived method alone.8,18 -20 The right ventricular outflow tract acceleration time (AT) was used to estimate mean pulmonary artery pressure (mPAP) using the Dabestani–Mahan equation:
mPAP = 90 − (0.62 × AT), as proposed by Dabestani et al. 21 This approach was adopted to account for methodological variability across studies, as some rely on TR-derived measurements, others on PAT-derived estimates, and some use both. Right ventricular function was assessed using TAPSE (indexed to body surface area for individuals < 18 years) and RVMPI. Adenotonsillectomy was performed under general anesthesia, with adenoidectomy using a curette and tonsillectomy via cold dissection. Standard postoperative care included pain management, soft diet, hydration, and counseling on danger signs and activity restriction.
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board of Hawassa University, College of Medicine and Health Sciences (Ref. No. IRB 409/25). The requirement for informed consent was waived due to the retrospective nature of the study. All data were anonymized, and patient identifiers were removed prior to analysis to ensure confidentiality. The corresponding author can provide a copy of the IRB approval letter upon request.
Results
Sociodemographic, Anthropometric, and Clinical Profiles of Participants
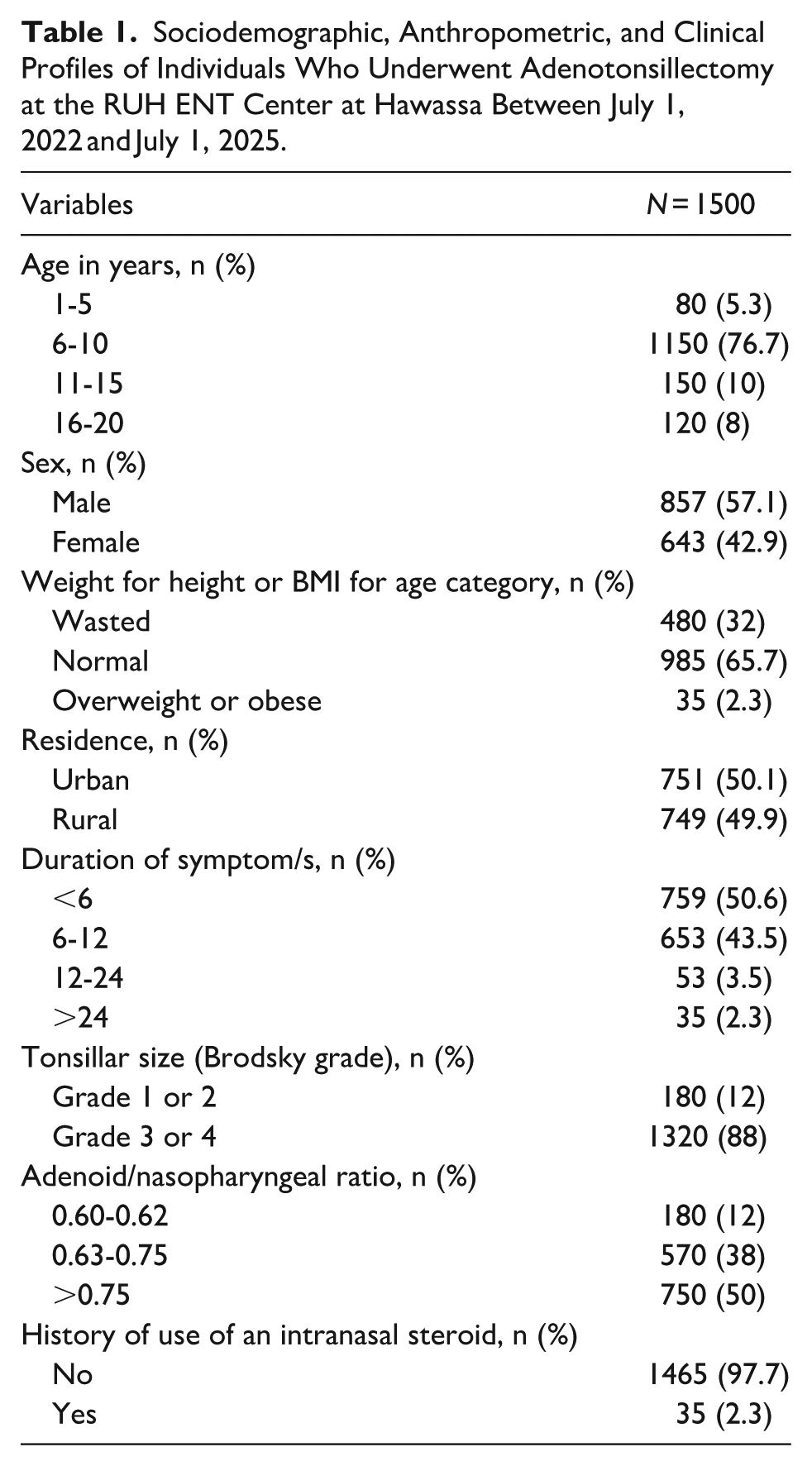
Out of 1530 individuals who underwent adenotonsillectomy, 1500 fulfilled the inclusion criteria and were included in this study. The median age was 8 years (IQR 7-10), with more than three-quarters (76.7%) aged 6 to 10 years, and a male-to-female ratio of 1.3. Nearly one-third (32%) were wasted, and 2.3% were overweight or obese. The majority (94.1%) reported a symptom duration of ≤12 months. More than three-quarters (88%) had grade 3 or 4 adeno-tonsillar hypertrophy, and 50% had an adenoid-to-nasopharyngeal ratio > 0.75 (Table 1).
Sociodemographic, Anthropometric, and Clinical Profiles of Individuals Who Underwent Adenotonsillectomy at the RUH ENT Center at Hawassa Between July 1, 2022 and July 1, 2025.
Types of Symptoms Reported by Caregivers or Individuals
Among the 1500 participants with adeno-tonsillar hypertrophy (ATH), a total of 10 887 symptoms were reported preoperatively. Respiratory symptoms accounted for 5814, sleep-related symptoms 4106, and oropharyngeal symptoms 967. Snoring was most common (73.3%), followed by nighttime mouth breathing (72%) and daytime mouth breathing (68.7%; Figure 1).

Types of symptoms reported by caregivers or individuals who had ATH and undergoing adenotonsillectomy at the RUH ENT Center, Hawassa, between July 1, 2022 and July 1 2025.
Types of Non-cardiopulmonary Complications Identified at Presentation
Figure 2 depicts the most commonly identified complications were OSA (34%), learning difficulties (33%), and SAM (26%).

Types of symptoms complications identified in individuals with ATH and undergoing adenotonsillectomy at the RUH ENT Center, Hawassa, Between July 1, 2022 and July 1, 2025.
Prevalence and Predictors of Pulmonary Hypertension
As demonstrated in Table 2, out of 1500 individuals with ATH, 89 (5.9%) developed pulmonary hypertension. A sensitivity analysis of the 3 mPAP estimation methods showed that the prevalence of pulmonary hypertension (PH) was 6.1% using TR-derived mPAP only, 5.8% using PAT-derived mPAP only, and 5.6% using the higher of the 2 values when both were available. Agreement between the methods was excellent, with Cohen’s kappa values of 0.92 for TR versus PAT, 0.94 for TR versus higher-of-two, and 0.95 for PAT versus higher-of-two, indicating that the choice of mPAP estimation method had minimal impact on PH classification in our cohort. To assess the robustness of this assumption, sensitivity analyses were also performed using RAP values of 3 and 8 mmHg, which resulted in minimal changes in PH prevalence (5.82% and 5.97%, respectively).
Predictors of Pulmonary Hypertension in Individuals Who Underwent Adenotonsillectomy at the RUH ENT Center at Hawassa Between July 1, 2022 and July 1, 2025.

Note. Data are presented as
In the multivariable logistic regression analysis, 5 variables were included, with 89 pulmonary hypertension events, yielding an events-per-variable ratio of 17.8, which exceeds the recommended minimum and supports the robustness of the model. The model demonstrated good discriminative ability with an ROC AUC of 0.87. Model calibration was adequate, as indicated by the Hosmer–Lemeshow goodness-of-fit test (χ2 = 5.31, P = .72; Figure 3). Individuals with wasting had 2.1 times higher odds of pulmonary hypertension compared to those with normal weight (Adjusted Odds Ratio [AOR]: 2.1, 95% CI: 1.5–3.7; P = .04). Overweight or obese participants had a fourfold increased odds (AOR: 4.0, 95% CI: 2.2–13.1; P < .001). The wide confidence interval for overweight/obesity suggests imprecision. An adenoid-to-nasopharyngeal ratio > 0.75 was associated with 2.4 times higher odds (AOR: 2.4, 95% CI: 1.3–6.1; P = .03). Daytime mouth breathing and stertor were associated with 2.0 (95% CI: 1.2–3.5; P = .03) and 2.7 (95% CI: 1.6–4.7; P = .02) times higher odds, respectively. Presence of obstructive sleep apnea (OSA, based on adult criteria) carried 3.6 times higher odds (95% CI: 1.9–6.7; P < .001).

ROC curve for the logistic regression model predicting pulmonary hypertension in individuals with ATH and undergoing adenotonsillectomy at the RUH ENT Center, Hawassa, between July 1, 2022 and July 1, 2025.
Resolution of Pulmonary Hypertension
Baseline median mPAP was 31.5 mmHg (IQR 26–40.5). At 6 weeks post-adenotonsillectomy, the median mPAP significantly decreased to 15.5 mmHg (IQR 11–20.5), with a further decline to 6.3 mmHg (IQR 4.2–8.3) observed at 12 weeks. By 6 weeks, 82 of 89 individuals (92.1%) had pulmonary pressures below the diagnostic threshold for pulmonary hypertension, and the remaining 7 (7.9%) also reached this threshold by 12 weeks, with no evidence of relapse or residual borderline elevations during the follow-up period. The Friedman test demonstrated a statistically significant change in median mPAP across the 3 time points (P < .001), and post-hoc Wilcoxon signed-rank tests with Bonferroni correction confirmed significant differences between all follow-up intervals. Median (IQR) differences were as follows: pre-op to 6 weeks, 16.0 mmHg (10.5–19.5); 6 to 12 weeks, 9.2 mmHg (7.0–11.0); and pre-op to 12 weeks, 25.2 mmHg (21.5–29.5), reflecting early postoperative normalization of pulmonary pressures (Figure 4).

Progress in mean pulmonary artery pressure at baseline (pre-op), 6 weeks, and 12 weeks following adenotonsillectomy in individuals with ATH and undergoing adenotonsillectomy at the RUH ENT Center, Hawassa, between July 1, 2022 and July 1, 2025.
Right Ventricular Dysfunction
Among the 89 individuals with pulmonary hypertension, longitudinal RV dysfunction was observed in 8 cases at baseline (median TAPSE 1.5 cm, IQR 1.3–1.7). At 6 weeks, 6 of 8 individuals (75%) showed improvement below the dysfunction threshold, and the remaining 2 cases (25%) normalized by 12 weeks. Friedman’s test indicated a statistically significant change in median TAPSE across the 3 time points (P < .001), with post-hoc comparisons confirming differences between each follow-up (Figure 5). Global RV dysfunction was observed in 6 individuals at baseline (median RVMPI 0.48, IQR 0.45-0.51). By 6 weeks, 4 of 6 showed improvement, and the remaining 2 normalized by 12 weeks. Friedman’s test demonstrated a significant change in median RVMPI across time points (P

Progress in TAPSE at baseline (pre-op), 6 weeks, and 12 weeks following adenotonsillectomy in individuals with ATH and undergoing adenotonsillectomy at the RUH ENT Center, Hawassa, between July 1, 2022 and July 1, 2025.

Progress in RVMPI at baseline (pre-op), 6 weeks, and 12 weeks following adenotonsillectomy in individuals with ATH and undergoing adenotonsillectomy at the RUH ENT Center, Hawassa, between July 1, 2022 and July 1, 2025.
Discussion
This study assessed the prevalence of pulmonary hypertension (PH) and right ventricular (RV) dysfunction, identified predictors of PH, and evaluated the short-term impact of adenotonsillectomy on pulmonary artery pressure and RV function in individuals with adeno-tonsillar hypertrophy (ATH). The findings highlight the importance of early recognition, risk stratification, and timely surgical intervention to potentially prevent long-term cardiopulmonary complications in this population.
While right heart catheterization remains the gold standard for diagnosing pulmonary hypertension, echocardiography provides a widely used, non-invasive alternative for screening and evaluating RV function.22 -24 Tricuspid regurgitation (TR) gradient was used to estimate systolic pulmonary artery pressure, while right ventricular myocardial performance index (RVMPI) and tricuspid annular plane systolic excursion (TAPSE) were used to assess RV function. 11 It should be emphasized, however, that echocardiographic estimates do not equate to invasive hemodynamics, and prevalence may therefore be under- or over-estimated.
Pulmonary hypertension and RV dysfunction are recognized complications of chronic, unrelieved upper airway obstruction.25,26 Persistent obstruction due to ATH can result in hypoxemia and hypercapnia, triggering pulmonary vasoconstriction.26,27 Over time, this increases RV afterload and may contribute to RV remodeling or dysfunction if prolonged. 28
The reported prevalence of PH varies widely. For instance, 51% in Turkey, 43.6% in Nigeria, 36% in Brazil, 21.9% in Kenya, 7.3% in Iran, and 5.9% in this study.18 -20,28,29 These discrepancies likely reflect differences in referral patterns, disease severity, sample sizes, and diagnostic criteria, including variation in mean pulmonary arterial pressure cutoffs (some studies use 25 mmHg).
The association between PH and body habitus in our study is consistent with prior literature. Overweight/obese individuals may have a higher risk due to the additive effects of ATH and obesity-related conditions such as obstructive sleep apnea (OSA), obesity hypoventilation, obesity-related cardiomyopathy, and endothelial dysfunction. 30 Intermittent nocturnal hypoxia, a hallmark of OSA, can induce pulmonary vascular remodeling through repetitive cycles of hypoxia and reoxygenation, promoting smooth muscle proliferation, vasoconstriction, and structural changes in the pulmonary vasculature. Systemic inflammation, which may be amplified in children with ATH due to chronic upper airway obstruction, could further contribute to endothelial dysfunction and elevated pulmonary pressures. 31
Underweight individuals may be predisposed due to increased susceptibility to recurrent respiratory infections and chronic hypoxia.32,33 These proposed mechanisms are hypotheses supported by literature, and the observational nature of this study prevents causal inference.
A higher adenoid-nasopharyngeal ratio was associated with PH, reflecting more severe upper airway obstruction and chronic hypoxia, consistent with findings from studies in Turkey, Nigeria, and Kenya.34 -36 Similarly, daytime mouth breathing, stertor, and clinically diagnosed OSA were associated with PH, indicating clinically significant intermittent airway obstruction. 18
Adenotonsillectomy was associated with short-term echocardiographic improvement in pulmonary artery pressures and RV function. By 6 weeks, most individuals demonstrated normalization of pressures, with remaining cases improving by 12 weeks. Reductions in RVMPI and improvements in TAPSE were observed, suggesting enhanced RV performance postoperatively. These findings align with studies from Turkey, Italy, Egypt, and other countries. 7 This may reflect the relief of upper airway obstruction after adenotonsillectomy, which reduces hypoxia and pulmonary vascular resistance, leading to lower pulmonary artery pressure. However, it should be emphasized that long-term outcomes remain unknown, and these findings do not imply permanent reversal.5,7,8
Given the retrospective design, absence of a control group, and potential for regression to the mean, causal relationships cannot be established, and observed improvements should be interpreted as temporal associations.
Finally, these results have implications for screening strategies in resource-limited settings. Echocardiography offers a feasible, non-invasive tool for early identification of PH in children with ATH. Targeted screening of high-risk individuals (eg, extreme body weight, severe adenoidal obstruction, or clinical OSA) may optimize resource utilization and support timely intervention, although cost-effectiveness studies are warranted.
Conclusion
The prevalence of pulmonary hypertension (PH) in children and adolescents with adeno-tonsillar hypertrophy was found to be 5.9%. The presence of daytime symptoms, such as daytime stertor, mouth breathing, being underweight or overweight/obese, a higher adenoid-to-nasopharyngeal (AN) ratio, and OSA were significantly associated with the development of pulmonary hypertension. Based on these findings, we recommend targeted echocardiographic evaluation for children exhibiting these clinical features to enable early detection and management of PH.
Out of all individuals with pulmonary hypertension, 8 developed longitudinal and 6 developed global right ventricular dysfunctions. However, both pulmonary hypertension and right ventricular dysfunction showed improvement following adenotonsillectomy. Therefore, early recognition and surgical intervention in high-risk patients may be associated with improvement in in preventing or reversing cardiovascular complications such as pulmonary hypertension and right ventricular dysfunction.
Limitations of the Study
This study has several limitations. Its retrospective design, based on chart reviews, may have introduced misclassification bias. Pulmonary hypertension and right ventricular dysfunction were assessed using echocardiography rather than the gold-standard right heart catheterization or cardiac MRI, and obstructive sleep apnea (OSA) was diagnosed clinically rather than by polysomnography, potentially leading to diagnostic misclassification. The use of a fixed RAP value (5 mmHg), though consistent with prior pediatric studies, may not reflect individual hemodynamic variability, particularly in malnourished children.
Echocardiographers were not blinded to surgical status at follow-up, and inter-observer variability was not formally assessed, which could introduce measurement bias. Potential residual confounding factors such as altitude effects, anemia severity thresholds, and socioeconomic status were not fully accounted for. In addition, oxygen saturation data, either resting or nocturnal, were not collected, limiting evaluation of hypoxia-related mechanisms.
The short 12-week follow-up period limits assessment of long-term outcomes, and the absence of a non-surgical control group prevents definitive attribution of observed improvements solely to adenotonsillectomy, as spontaneous improvement or regression to the mean cannot be excluded. Being a specialized ENT center–based study may introduce selection bias, and postoperative echocardiographic changes may partly reflect regression to the mean, especially in patients with higher baseline values. The small number of right ventricular dysfunction cases also limits the interpretability of subgroup analyses. Despite these limitations, this study provides valuable data on the prevalence, risk stratification, and short-term echocardiographic changes in pulmonary hypertension among children with adeno-tonsillar hypertrophy, highlighting the potential role of adenotonsillectomy in early postoperative normalization of pulmonary pressures.
Footnotes
Acknowledgements
The authors gratefully acknowledge the data collectors and the dedicated staff of the RUH ENT Clinic for their invaluable support in this study.
Author Contributions
Mohammed Nasir: Conceptualization; Methodology; Data curation; Formal analysis; Investigation; Writing – original draft, Writing – review & editing. Muluken Bekele: Methodology; Supervision; Validation; Writing – review & editing. Sura Markos: Conceptualization; Supervision; Data interpretation; Critical revision of the manuscript for important intellectual content; Final approval of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.*