
Abstract
Pulmonary tumor thrombotic microangiopathy is a rare condition in which embolization of tumor cells to the pulmonary arterioles causes fibrocellular intimal thickening and activation of the coagulation cascade resulting in pulmonary hypertension and right heart failure. Herein, we highlight a young 35-year-old male with no known past medical history who presented with recurrent syncope and dyspnea, and was found to have severe right heart failure and pulmonary hypertension. He developed sudden clinical deterioration and died after a cardiac arrest. Autopsy revealed poorly differentiated gastric adenocarcinoma and pulmonary tumor thrombotic microangiopathy. New onset severe pulmonary hypertension and right heart failure without any other obvious etiology should encourage the reader to evaluate for pulmonary tumor thrombotic microangiopathy and undergo a diligent search for underlying malignancy. This case highlights recurrent syncope as a rare presentation of this rapidly fatal disease.
Introduction
Pulmonary tumor thrombotic microangiopathy (PTTM) was described in 1990 by von Herbay who reviewed 630 autopsy cases with known malignancy and found the prevalence to be 3.3%. 1 Most cases (79% in one systematic review) 2 are diagnosed post-mortem and syncope is an uncommon clinical feature. 2 This report describes a rapidly fatal case of hitherto undiagnosed gastric malignancy presenting with recurrent syncope.
Case
A 35-year-old Hispanic male construction worker with no past medical history presented with recurrent exertional syncope which was associated with chest pain, dyspnea, bladder incontinence, and stiffening of extremities. In the emergency department, he was found to be tachycardic (heart rate = 121 beats per minute), tachypneic (respiratory rate = 33 breaths per minute), and with an oxygen saturation of 93% on 2 L nasal cannula. Heart and lung examination were normal. He denied use of tobacco or illicit substances, a history of pulmonary embolism, liver disease, autoimmune disease, or a family history of pulmonary hypertension or syncope.
Electrocardiogram showed right axis deviation and sinus tachycardia. Echocardiography showed an estimated pulmonary arterial systolic pressure (PASP) of 73 mmHg, severe right atrial dilation, severely dilated and hypokinetic right ventricle (RV), and a right to left shunt across patent foramen ovale.
Chest tomography with pulmonary angiogram (CTPA) revealed bilateral patchy ground-glass opacities, centrilobular “tree-in-bud” nodules, enlarged pulmonary artery, and enlarged RV, but no pulmonary embolism, Figure 1. No findings to suggest metastatic disease. Radionuclide perfusion scan showed patchy perfusion defects throughout both lungs. Lower extremity Doppler ultrasonography to evaluate for venous thrombosis was negative, so the patient was administered prophylactic anticoagulation with heparin. Laboratory abnormalities included elevated pro-brain natriuretic peptide at 3680 pg/mL (30–125 pg/mL), troponin at 0.06 ng/mL (<0.03 ng/mL), and thrombocytopenia at 105 bil/L (140-340 bil/L). Autoimmune disease workup and evaluation for coagulopathy was non-diagnostic.

Chest Tomography showing subtle diffuse ground-glass (blue arrow) and multiple tree-in-bud opacities (red arrow) and enlarged right ventricle and right atrium.
During the hospitalization, he continued to have multiple witnessed seizure-like syncopal episodes (> 10) associated with sinus tachycardia requiring benzodiazepine pushes on two occasions. Video electroencephalogram was negative for epileptiform discharges. Computed tomography (CT) of the head, as well as carotid ultrasound were normal.
His oxygen supplementation increased to 15 L per minute via a non-rebreather mask and an arterial blood gas analysis showed an elevated A-a gradient of 580 and the following: pH = 7.43 (7.35–7.45), partial pressure of carbon dioxide = 24 mmHg (35–45 mmHg), partial pressure of oxygen = 66 mmHg (79–99 mmHg), and bicarbonate = 15 mMol/L (22–26 mMol/L).
He was scheduled for right heart catheterization. However, on hospital day 3, during an episode of syncope he developed sinus bradycardia (heart rate = 57 per minute), hypotension (blood pressure = 75/44 mmHg) and subsequent cardiac arrest resulting in death.
Autopsy showed poorly differentiated gastric adenocarcinoma, PTTM with direct tumor invasion to esophagus and surrounding gastric soft tissue Figures 2 and 3. There was metastasis to celiac and periaortic lymph nodes, the lumbar spine, and pulmonary tumor thrombotic microangiopathy. There was a left upper lobe pulmonary infarction with hemorrhage, pulmonary congestion, cardiomegaly with RV dilation and mild hepatomegaly. Brain neuropathology showed hypoxic-ischemic injury but no evidence of metastatic disease.

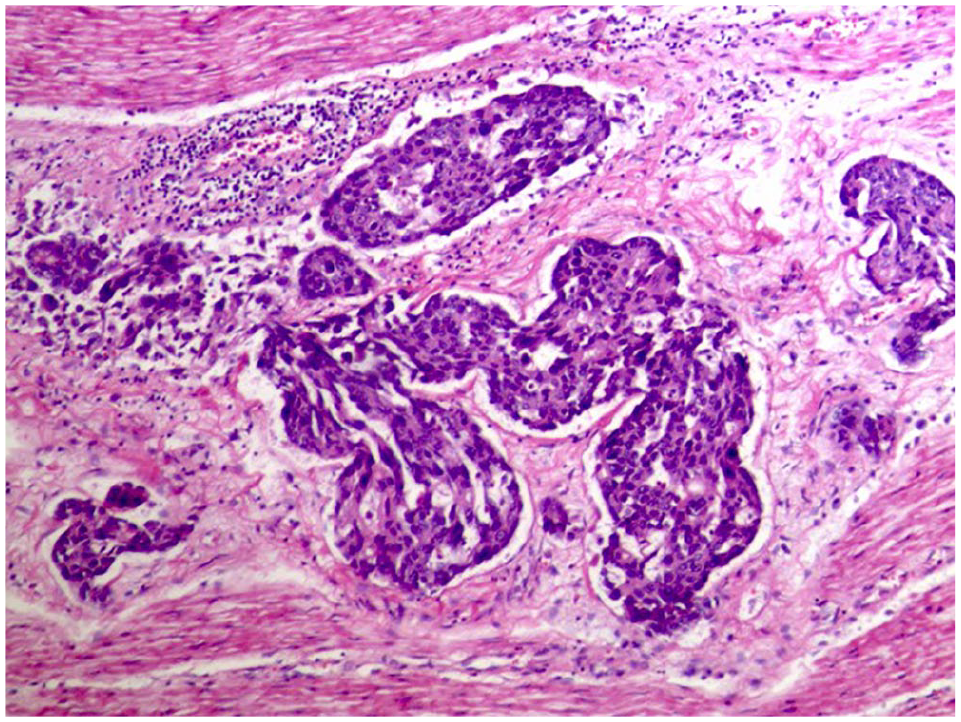
H and E stain showing highly atypical cells causing fibroblastic intimal hypertrophy in the pulmonary vessels, consistent with pulmonary tumor thrombotic microangiopathy.
H and E stain showing highly atypical cells invading muscularis externa in the gastric wall.
Discussion
PTTM is a rare disease, often diagnosed post-mortem, with mean time from onset of symptoms to death of 1 month. 3 Ante-mortem diagnosis is made in 15/160 cases (9.4%). 2 Common presenting features include dyspnea, hypoxemia, cough and abdominal pain.2,4 Syncope is an uncommon presentation found only in 3.7% in a series 2 and recurrent syncope at presentation has not been reported, to the best of our knowledge.
Syncope is defined as a transient loss of consciousness (TLOC) due to global cerebral hypoperfusion characterized by rapid onset, short duration and spontaneous recovery. 5 The etiology of recurrent syncope in this patient is likely multifactorial and includes RV failure, arrhythmias, recurrent pulmonary emboli, orthostatic hypotension, neurally mediated (reflex) syncope and seizures. 6 Severe RV failure causes syncope due to (a) decreased RV-Left ventricular interdependence, (b) RV-Pulmonary artery uncoupling and (c) resultant abrupt drop in systemic pressures due to decrease in stroke volume in the setting of fixed downstream obstruction and pulmonary hypertension.7,8 Arrhythmias can occur due to RV failure and right atrial dilation 9 or recurrent pulmonary emboli. 10 Syncope is a reported presenting symptom in PE 11 as well as PTTM. 12 Neurally mediated syncope can be triggered in the carotid sinus or gastrointestinal tract and leads to activation of the autonomic efferent pathway that causes an increase in parasympathetic or sympathetic activity, resulting in a “vasodepressor type” if hypotension and vasodilation predominates, or a “cardio-inhibitory type” when bradycardia or asystole predominates. 5 Gastrointestinal causes of recurrent syncope have been reported13,14 and could have been contributory in our patient since there was direct tumor invasion to esophagus and gastric soft tissue on autopsy. With bladder incontinence and stiffening of extremities as presenting features, seizure is a consideration for TLOC, but with a Calgary Syncope Diagnostic Questionnaire 15 score < 1 and a non-diagnostic electroencephalogram (EEG) in this case, syncope is more likely than seizures. Orthostatic vital signs were not documented.
Hypoxemia is a common presenting feature of PTTM. 3 Multiple case reports link the rapid progression of hypoxemia to worse outcomes. 16 Mechanisms of hypoxia in PTTM include reduction in RV cardiac output due to severe PH, right-to-left shunting, tumor infiltration of the alveolar lining, and impairment of gas diffusion across the capillary membrane due to arteriole hyperplasia and lymphatic obstruction. 16
Other abnormalities seen in PTTM include diffuse reticular and nodular opacities, and non-specific centrilobular micronodules (tree-in-bud opacities) on chest CT.4,17 Such nodules most likely result from hematogenous spread of malignancy through pulmonary arterioles. 17 Right heart catheterization reveals pre-capillary pulmonary hypertension (average PASP = 71) 2 and sometimes shows discordant pulmonary artery wedge and left ventricular end-diastolic pressures. 16 Cytological examination of wedge blood samples can detect tumor cells. 18 Positron Emission Tomography can localize metastatic sites and provide guidance for biopsy. 19 Lung biopsy provides the conclusive diagnosis of PTTM, but is rarely done when the patient is alive. 17 Histologically, tumor cells in pulmonary vessels engender a fibrointimal hyperplasia, in-situ thrombosis, and vascular narrowing. 1 PTTM is often associated with gastric adenocarcinoma, particularly the signet-ring cell subtype,2,17 but other sources include lung, breast, intestinal and ovarian tumors. When PTTM is diagnosed ante-mortem, therapy with anticoagulation, chemotherapy, imatinib, bevacizumab, dexamethasone, and a combination with pulmonary vasodilators (endothelin-receptor antagonist and phosphodiesterase type 5 inhibitors) has led to temporary improvement in cardiorespiratory status and hypoxemia. However, survival, even with treatment, remains poor.2,3
Conclusion
Recurrent syncope is a rare manifestation of PTTM. New onset severe pulmonary hypertension and right heart failure without any other obvious etiology should encourage the reader to evaluate for PTTM and undergo a diligent search for underlying malignancy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.