
Abstract
Objective:
To investigate the association of serum 25(OH)D levels with dengue severity in Vietnamese children and the association of common VDR gene polymorphisms with disease outcomes.
Methods:
This cross-sectional study included 178 children with confirmed dengue at a tertiary hospital in 2024. Serum 25(OH)D levels were measured, and 4 VDR polymorphisms (FokI, ApaI, TaqI, BsmI) were genotyped. Associations with WHO-defined severity were assessed using logistic regression.
Results:
Severe dengue was more common in older children and was characterized by greater plasma leakage and thrombocytopenia (P < .001). Serum 25(OH)D concentrations were independently and inversely associated with dengue severity, with an adjusted odds ratio of 0.89 (95% CI: 0.85-0.93; P < .001). In contrast, allele and genotype distributions of the 4 VDR polymorphisms did not differ significantly across severity groups (P > .05).
Conclusion:
Our findings suggest vitamin D status may be more relevant to dengue severity than inherited VDR variation.
Introduction
Dengue remains a major cause of viral illness transmitted by mosquitoes among children worldwide. Its rapid expansion over the past several decades has intensified pressure on public health systems, particularly in tropical and subtropical regions. Countries in Southeast Asia experience a disproportionately high burden of pediatric dengue infections and related fatalities, largely due to persistent endemic transmission and environmental conditions that support efficient vector propagation.1 -4 The clinical spectrum of dengue in children is broad, ranging from a self-limited febrile illness to severe dengue characterized by plasma leakage, thrombocytopenia, and organ impairment. Severe manifestations such as dengue shock syndrome remain a major cause of hospitalization and critical illness among pediatric populations in endemic areas.3,5 Despite advances in supportive care and improved case management, severe dengue continues to be associated with substantial morbidity and mortality, particularly among children with complications or delayed clinical recognition. 6
In Vietnam, dengue continues to be an important public health problem. The Mekong Delta is one of the regions with the highest number of cases each year. 7 In 2023, more than 167 000 dengue cases were reported nationwide, showing a high prevalence of dengue in the country and placing Vietnam among the most affected countries in Southeast Asia. Evidence from pediatric cohorts in the Mekong Delta indicates that currently used clinical warning signs and severity scoring systems show limited predictive accuracy for early shock detection. 8 This limitation reflects the fact that many clinical and laboratory abnormalities become apparent only during disease progression rather than at initial presentation. Current evidence indicates that severe dengue reflects the interaction of viral factors, host immune responses, and endothelial dysfunction. These findings underscore the multifactorial pathogenesis of the disease and emphasize the urgent need for improved early prognostic markers.9 -12
Vitamin D has emerged as an important immunomodulatory hormone with biological functions extending beyond its classical role in calcium and bone metabolism. The active form of vitamin D influences both innate and adaptive immune responses through the regulation of macrophage activation, cytokine production, and immune cell differentiation.13,14 In the context of dengue, accumulating evidence indicates that immune–endothelial interactions play a central role in disease severity, with functional disruption of endothelial barrier integrity rather than direct endothelial cell damage, which is considered a key mechanism underlying plasma leakage and shock.11,12 Experimental studies have demonstrated that vitamin D can modulate inflammatory responses by reducing the production of pro-inflammatory cytokines in activated immune cells and by regulating Toll-like receptor–mediated signaling pathways.15,16 With regard to dengue infection, these immunomodulatory effects suggest a potential role for vitamin D in influencing host inflammatory responses and immune-mediated vascular dysfunction, which are central to the development of plasma leakage.17 -19 A growing body of observational research, including studies involving children, has suggested that lower serum levels of 25(OH)D are linked to more severe manifestations of dengue infection.20 -22 However, the evidence remains mixed. Several studies have failed to confirm an independent association once potential confounding factors were taken into account. 23 These inconsistencies may be attributed to variations in study design, differences in patient populations, inconsistent criteria for defining disease severity, and the timing of vitamin D assessment during the acute stage of infection. Importantly, vitamin D is considered a negative acute-phase reactant, meaning that circulating 25(OH)D concentrations can decline in the presence of systemic inflammation. As a result, measurements obtained during acute illness may not accurately reflect an individual’s baseline vitamin D status, complicating the interpretation of findings in dengue research.24,25
Vitamin D exerts its biological effects largely through binding to the VDR, a nuclear hormone receptor that is widely expressed in immune cells as well as vascular endothelial cells. 26 Through this receptor, vitamin D plays an important role in regulating immune responses and inflammatory processes. Several well-characterized genetic variants of the VDR gene, most notably FokI, ApaI, TaqI, and BsmI, have been shown to influence receptor function or VDR expression, thereby modulating downstream signaling pathways. These polymorphisms have therefore been investigated in relation to susceptibility to, and clinical outcomes of, a range of infectious and inflammatory conditions.13,14,27 In the context of dengue infection, research exploring the relationship between VDR polymorphisms and disease severity has produced mixed findings that appear to vary across populations. Moreover, data specifically addressing pediatric dengue cases remain scarce, limiting firm conclusions in this vulnerable group.20,28,29
Serum 25(OH)D is commonly used to reflect overall vitamin D status in the body. However, the biological effects of vitamin D depend on its interaction with the VDR at the cellular level. Genetic variations in the VDR gene may influence how vitamin D functions in immune and endothelial cells. In dengue infection, examining both circulating vitamin D levels and VDR gene variants may help clarify whether disease severity is more related to vitamin D deficiency or to differences in cellular response to vitamin D.
Therefore, this study aimed to evaluate the association between serum vitamin D status and dengue severity in pediatric patients admitted to a tertiary hospital in the Mekong Delta region of Vietnam, and to assess whether common VDR gene polymorphisms are independently associated with disease severity.
Methods
Study Design and Population
This cross-sectional study was conducted at Can Tho Children’s Hospital, a tertiary pediatric hospital in Can Tho City, Vietnam, from January to December 2024. Children under 16 years of age with laboratory-confirmed dengue virus infection who were admitted during the study period were eligible for inclusion. Dengue infection was confirmed utilizing standard diagnostic methods, including NS1 antigen detection and/or serological testing, in accordance with national and institutional guidelines.30,31
To minimize selection bias, study subjects were enrolled consecutively. Based on the 2009 World Health Organization classification, participants were categorized as dengue without warning signs (D-WS), dengue with warning signs (D+WS), or severe dengue (SD). 31 Children with incomplete clinical data or insufficient blood samples for serum vitamin D measurement or genetic analysis were excluded.
All eligible pediatric dengue patients admitted during the study period were enrolled consecutively. A total of 178 children had complete clinical, biochemical, and genetic data and were included in the analysis. Because this was an observational study with a fixed recruitment period, no formal sample size calculation was performed. Although the sample was adequate to assess the association between serum vitamin D levels and dengue severity, it may not have been large enough to detect small genetic effects related to VDR polymorphisms.
This study was conducted in strict adherence to the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Hanoi Medical University (Approval No. 1059/GCN-HMUIRB, dated January 19, 2024). Administrative permission to conduct the study was also granted by Can Tho Children’s Hospital. Written informed consent was obtained from the parents or legal guardians of all participating children prior to enrollment.
Clinical and Laboratory Data
Demographic characteristics, including age and sex, were recorded at enrollment. Nutritional status was assessed during routine clinical evaluation based on standardized hospital protocols. Patients were classified as obese if their body mass index-for-age z-score exceeded +2 standard deviations, in accordance with the WHO Child Growth Standards for children aged 0 to 5 years and the WHO Growth Reference for children and adolescents aged 5 to 19 years.32,33
Clinical manifestations monitored during hospitalization included bleeding, hepatomegaly, and polyserositis (defined as pleural effusion and/or ascites detected via clinical examination or imaging). Acute-phase laboratory parameters included white blood cell count, platelet count, hematocrit, and serum albumin. Specific laboratory abnormalities were defined as leukopenia (white blood cell count <4 × 109/L), thrombocytopenia (platelet count <100 × 109/L), elevated hematocrit (>40%), and hypoalbuminemia (<35 g/L). 34
Measurement of Serum Vitamin D
Serum 25(OH)D levels were measured from blood samples collected during the critical phase of dengue infection (typically between days 3 and 6 of illness) using a chemiluminescent immunoassay (CLIA) on the Access 2 system (Beckman Coulter, USA), following the manufacturer’s instructions. Internal quality control procedures were performed routinely to laboratory standards. Vitamin D deficiency was defined as serum 25(OH)D concentrations <20 ng/mL, based on commonly used clinical cutoffs. 35
Genotyping of VDR Polymorphisms
Genomic DNA was extracted from peripheral blood samples using standard extraction protocols. Four common VDR polymorphisms—FokI (rs2228570), ApaI (rs7975232), TaqI (rs731236), and BsmI (rs1544410)—were genotyped using polymerase chain reaction amplification of the target regions followed by direct Sanger sequencing at the Center for Molecular Biomedicine, University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam.
Primer sequences and PCR conditions for each polymorphism are provided in Supplemental Table S1, and representative sequencing chromatograms are shown in Supplemental Figure S1.
Statistical Analysis
Categorical variables were summarized as frequencies and percentages, while continuous variables were presented as means with standard deviations or medians with interquartile ranges (IQR), based on data distribution. Comparisons across the 3 dengue severity groups (D-WS, D+WS, and SD) were performed using the Chi-square test or Fisher’s exact test for categorical variables (including genotype and allele frequencies). Hardy–Weinberg equilibrium was assessed for each VDR polymorphism using the chi-square test. For continuous variables, such as serum vitamin D levels, differences were assessed using one-way Analysis of Variance (ANOVA) or the Kruskal–Wallis test, as appropriate. When the Kruskal–Wallis test indicated a significant difference, pairwise comparisons were performed using Dunn’s post-hoc test with Holm correction.
To identify independent factors associated with dengue severity, multinomial logistic regression was employed (using the nnet package). Covariates included age group, sex, nutritional status, and serum vitamin D levels. Results were reported as odds ratios (ORs) with 95% confidence intervals (CIs).
All statistical analyses were performed using R software (version 4.5.2; R Foundation for Statistical Computing, Vienna, Austria). A 2-sided P value < .05 was considered statistically significant.
Results
Study Population and Baseline Characteristics
A total of 178 children with laboratory-confirmed dengue were included in the analysis and classified as dengue without warning signs (D-WS, n = 80), dengue with warning signs (D+WS, n = 25), or severe dengue (SD, n = 73).
Compared with non-severe cases, children with severe dengue were older and showed more signs of plasma leakage on clinical and laboratory assessment. Older children (6-16 years) were more likely to have SD (P = .001), while sex and nutritional status did not differ between severity groups (P > .05). Polyserositis, hepatomegaly, and hypoalbuminemia were more common in children with severe dengue (all P < .001), while bleeding showed borderline significance across severity groups (P = .05). Thrombocytopenia and elevated hematocrit were also more frequent in more severe cases (P < .001 and P = .035, respectively), whereas leukopenia did not differ significantly between groups (P > .05; Table 1).
Clinical and Laboratory Characteristics of Children With Dengue According to Disease Severity.
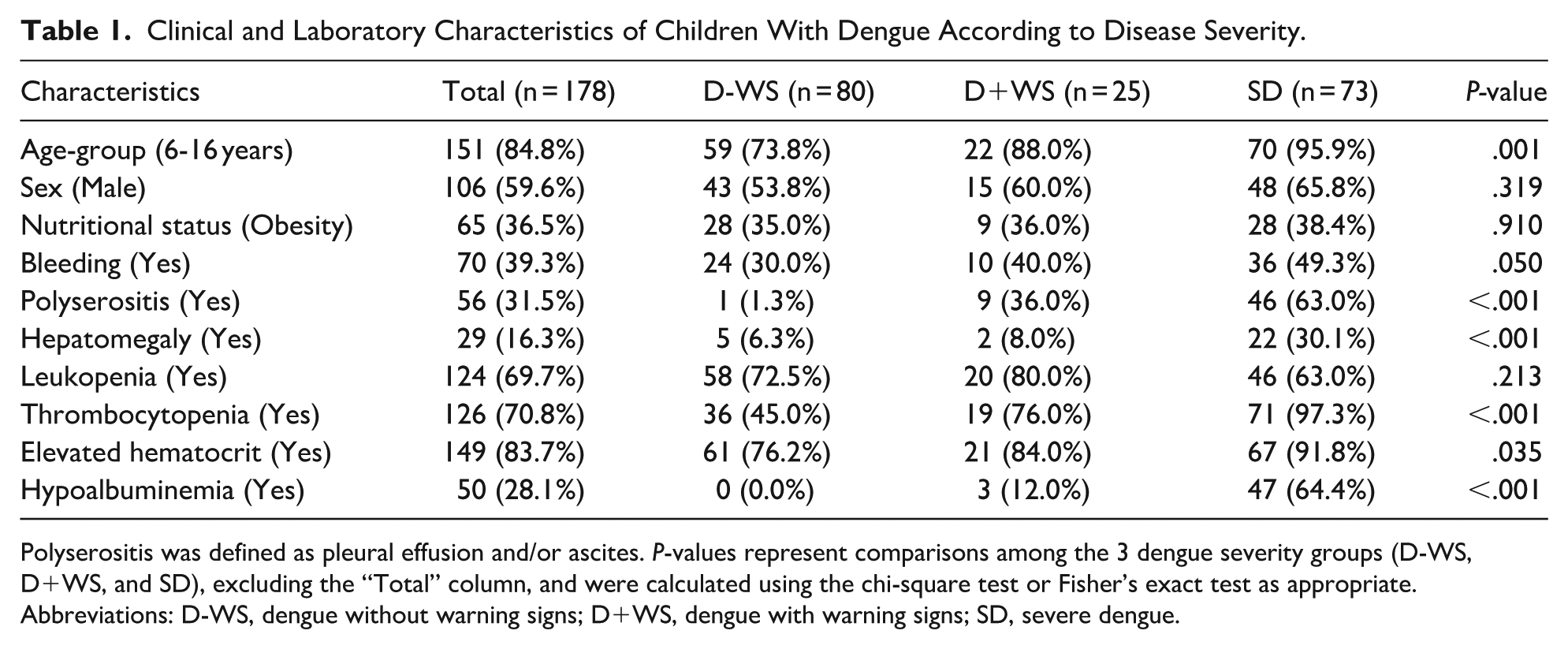
Polyserositis was defined as pleural effusion and/or ascites. P-values represent comparisons among the 3 dengue severity groups (D-WS, D+WS, and SD), excluding the “Total” column, and were calculated using the chi-square test or Fisher’s exact test as appropriate.
Abbreviations: D-WS, dengue without warning signs; D+WS, dengue with warning signs; SD, severe dengue.
Association Between Serum 25(OH) Levels and Dengue Severity
Serum 25(OH)D concentrations declined as dengue severity increased. Median 25(OH)D levels differed significantly among severity groups (Figure 1, P < .001), with the highest values observed in children without warning signs and the lowest in those with severe dengue.

Serum 25(OH)D concentrations across dengue severity groups. Box-and-whisker plots show median values and interquartile ranges. Overall differences among groups were assessed using the Kruskal–Wallis test, followed by Dunn’s post-hoc pairwise comparisons with Holm correction.
When classified by vitamin D status, the proportion of children with sufficient levels (≥30 ng/mL) decreased with increasing severity, whereas vitamin D deficiency (< 20 ng/mL) occurred more frequently in SD (Table 2, P < .001).
Association Between Serum 25(OH)D Status and Dengue Severity.
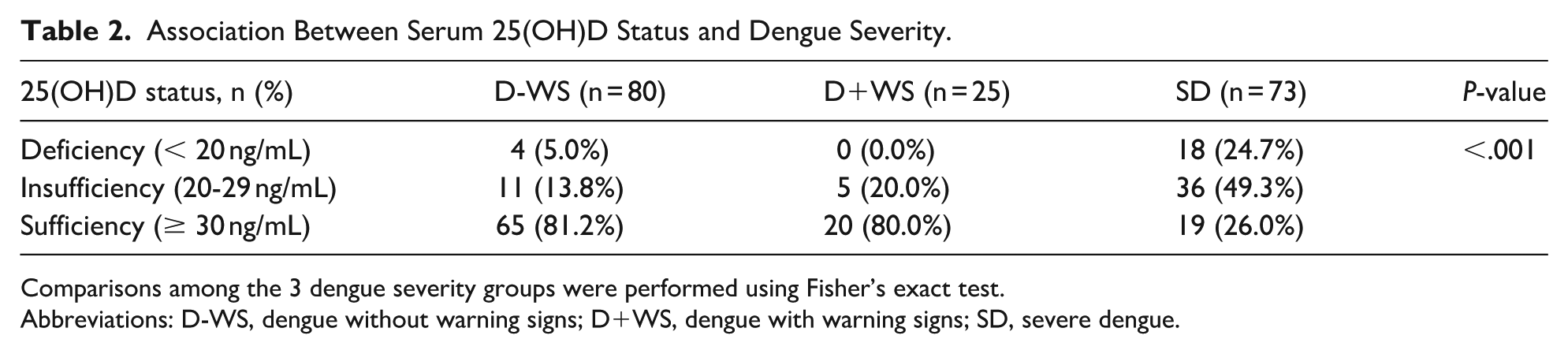
Comparisons among the 3 dengue severity groups were performed using Fisher’s exact test.
Abbreviations: D-WS, dengue without warning signs; D+WS, dengue with warning signs; SD, severe dengue.
Association Between VDR Polymorphisms and Dengue Severity
Genotype distributions were generally consistent with Hardy–Weinberg equilibrium across severity groups, with the exception of the FokI polymorphism in the D+WS group. None of the genotype frequencies differed significantly between severity groups (P > .05 for all comparisons). Homozygous variant genotypes for BsmI (AA) and TaqI (CC) were not detected in any group.
Allele frequency analysis showed similar findings. The distributions of major and minor alleles for all 4 polymorphisms were comparable across severity categories (P > .05). No association was found between VDR allelic variants and SD in this cohort. Across all severity groups, genotype and allele distributions demonstrated minimal variation (Table 3).
Association Between VDR Polymorphisms and Dengue Severity.

Overall, P-values were calculated using chi-square tests or Fisher’s exact test for comparison of genotype distributions across dengue severity groups.
Abbreviations: D-WS, dengue without warning signs; D+WS, dengue with warning signs; SD, severe dengue.
As none of the 4 VDR polymorphisms (FokI, ApaI, TaqI, and BsmI) showed a significant association with dengue severity in the genotype or allele analyses (all P > .05), these genetic variants were not included in the multinomial logistic regression model.
Multinomial Logistic Regression Analysis
In the multivariable model, serum 25(OH)D levels remained significantly associated with dengue severity after adjustment for age group, sex, and obesity. Higher serum 25(OH)D concentrations were linked to lower odds of severe dengue. The adjusted odds ratio (aOR) was 0.89 (95% CI: 0.85-0.93; P < .001) for SD compared with D-WS and 0.90 (95% CI: 0.86-0.95; P < .001) compared with D+WS (Table 4). Obesity was included as a covariate in the regression model and was not independently associated with dengue severity (P > .05).
Multinomial Logistic Regression Analysis of Factors Associated With Disease Severity.

Adjusted odds ratios (aOR) and 95% confidence intervals (95% CI) were obtained from multinomial logistic regression models. Comparisons of D+WS versus D-WS and SD versus D-WS were derived from a model with D-WS as the reference category, while SD versus D+WS was derived from a model with D+WS as the reference category. Serum 25(OH)D was analyzed as a continuous variable.
Abbreviation: Ref, reference category.
Discussion
Overall, our results point to a possible clinical relevance of the vitamin D axis in pediatric dengue severity. In this cohort of 178 children with laboratory-confirmed dengue from an endemic region, severe disease was more frequently observed among older children and was characterized by a high burden of plasma leakage and thrombocytopenia, reflecting the typical spectrum of SD in this setting. Two main observations deserve emphasis. First, serum 25(OH)D levels were independently and inversely associated with dengue severity, suggesting that vitamin D status could be a modifiable factor related to disease progression. Second, in contrast to the serological findings, common polymorphisms in the VDR gene showed no significant association with clinical outcomes, indicating that inherited variation in the VDR gene may be less relevant to dengue severity than dynamic changes in vitamin D status.
The identification of a potential biomarker associated with SD is particularly relevant in this setting. Recent evidence from the Mekong Delta has shown that existing clinical warning signs and severity scoring systems have limited predictive performance for dengue shock syndrome, thereby highlighting the need for improved prognostic indicators that can support early risk stratification in pediatric patients.
Obesity has been proposed as a potential modifier of vitamin D status and immune responses in infectious diseases and therefore represents a potential confounder in studies examining vitamin D–disease associations. In the present study, nutritional status, including obesity, was systematically documented and incorporated as a covariate in the multivariable regression analysis. However, obesity was not independently associated with dengue severity, nor did adjustment for nutritional status attenuate the observed association between serum 25(OH)D levels and disease severity. These findings suggest that the inverse association between vitamin D status and dengue severity observed in this cohort is unlikely to be confounded by obesity.
Several pediatric studies from South and Southeast Asia have reported lower serum vitamin D levels in children with more severe dengue, which is consistent with our findings, although results have varied across populations. Studies from Eastern India have reported a significantly higher prevalence of vitamin D deficiency among children with severe dengue, 36 while data from North India similarly demonstrated lower serum vitamin D levels in patients progressing to more severe clinical manifestations, including hemorrhagic fever and shock. 37 In addition, pediatric data from Sri Lanka identified vitamin D deficiency as an independent risk factor for plasma leakage during the critical phase of illness, 21 supporting the biological plausibility of a link between vitamin D status and dengue severity given its established role in immune modulation and endothelial barrier integrity.14,17,18
Variability across studies may reflect the biological behavior of serum 25(OH)D, which functions as a negative acute-phase reactant. Circulating concentrations decline during systemic inflammation.24,25,38 Levels may change as patients progress through the febrile, critical, and recovery phases of dengue. Such variation complicates comparisons when vitamin D is assessed at different clinical time points.
In this study, serum 25(OH)D was measured during the acute phase of illness, and the observed concentrations may therefore represent a combination of baseline nutritional status and inflammation-related changes occurring during infection. Consequently, reverse causality cannot be excluded. Lower vitamin D levels in severe cases may reflect the intensity of the inflammatory response rather than serving as a pre-existing determinant of disease severity. Similar associations between lower 25(OH)D levels and greater severity have been described in other acute infection settings, including sepsis. 39
Accordingly, the cross-sectional design limits causal inference, and it remains difficult to distinguish whether vitamin D deficiency predisposes to severe dengue or primarily reflects ongoing disease activity. Furthermore, the clinical patterns observed in this pediatric cohort are broadly consistent with trends reported in adult populations from dengue-endemic regions. Studies across South Asia have documented a high prevalence of vitamin D deficiency among hospitalized adults, with lower serum 25(OH)D concentrations consistently associated with more severe clinical manifestations of dengue. 22 Although immune responses and physiological adaptations to viral infection differ between children and adults, the recurrence of similar patterns across age groups suggests that vitamin D may influence dengue pathogenesis through fundamental immunomodulatory pathways. 40 In adult cohorts, reduced vitamin D levels have also been linked to heightened pro-inflammatory cytokine activity. However, as highlighted by Javed, such associations must be interpreted with caution given the inherent limitations of cross-sectional study designs. 41
Nevertheless, the relationship between vitamin D status and dengue severity has not been uniformly observed across all clinical settings. Several pediatric and mixed-age studies from South Asia have reported heterogeneous findings, with some cohorts aligning with an inverse association and others suggesting substantial regional or population-specific variation.20,23,36,37 Notably, Villamor et al reported an unexpected association in which lower 25(OH)D concentrations during the acute phase were linked to a reduced risk of progression to dengue hemorrhagic fever or shock, underscoring the complexity of causal inference in this context. 23 Moreover, evidence from other endemic regions suggests that the nutritional landscape of dengue is multifaceted, with other micronutrients—such as ferritin or retinol-binding protein—potentially demonstrating stronger or more direct associations with disease outcomes than vitamin D alone. 42
In contrast to the associations observed for serum vitamin D levels, no significant relationships were identified between common VDR polymorphisms and dengue severity at either the allelic or genotypic level in this pediatric cohort. The distributions of the FokI, ApaI, TaqI, and BsmI variants were comparable across clinical severity categories, indicating that inherited variation in the VDR gene is unlikely to confound the observed association between circulating 25(OH)D levels and disease severity.
Previous studies of VDR polymorphisms and dengue outcomes have reported similarly mixed results. Early work from Vietnam suggested a potential protective role of specific VDR variants against severe dengue, 29 whereas subsequent studies in other populations have reported associations primarily with dengue susceptibility rather than disease severity. For example, Singh et al demonstrated that VDR TaqI (rs731236) and ApaI (rs7975232) polymorphisms were associated with an increased risk of dengue infection in an Indian population, but did not evaluate progression to severe clinical phenotypes. 43 Other studies have reported inconsistent or null associations when severity-based outcomes were considered.20,28 Differences across studies likely reflect variations in study design, outcome definitions (susceptibility vs severity), population-specific genetic backgrounds, and the interaction between host genetic factors and environmental influences.
Overall, while VDR polymorphisms may affect susceptibility to dengue infection, circulating vitamin D levels during acute illness appear more closely related to disease severity. This pattern is consistent with the multifaceted and context-dependent nature of dengue pathogenesis. Several factors may account for the absence of significant genetic associations in this cohort. Allele frequencies and linkage disequilibrium patterns of common VDR variants differ across ethnic and geographic populations, which can influence the reproducibility of genetic associations. In addition, stratification into 3 severity categories reduced the sample size within each subgroup, potentially limiting power to detect modest genetic effects. Environmental and nutritional influences in children may also attenuate the measurable contribution of common VDR variants to clinical severity.44 -46
This study has several strengths, including its focus on a pediatric population in a highly dengue-endemic region, consecutive patient enrollment, and the integrated assessment of clinical features, serum vitamin D status, and VDR genetic variation.
Several limitations should also be acknowledged. The cross-sectional design and single time-point measurement of serum 25(OH)D limit causal inference and preclude assessment of temporal changes during illness. In addition, dengue serotype, viral load, and primary versus secondary infection status were not evaluated. Although the sample size was adequate for analyses of serum vitamin D levels, it may have been insufficient to detect modest genetic effects.
The findings of this study are important for understanding dengue severity in pediatric populations from endemic settings and have direct implications for early clinical risk stratification. The observed inverse association between serum vitamin D levels and dengue severity suggests that circulating vitamin D status may serve as a readily measurable biomarker to support early risk stratification in pediatric dengue, particularly in regions where existing clinical scoring systems have limited predictive performance. Although causal inference cannot be established, identifying potentially modifiable metabolic factors associated with severe outcomes is clinically relevant in resource-limited settings.
Studies that measure serum vitamin D repeatedly across different phases of dengue infection may help clarify how levels change over time and whether they are causally related to disease severity. Larger, multi-center pediatric cohorts are also needed to assess population-level variability and to more robustly evaluate gene–environment interactions. In addition, well-designed interventional trials examining vitamin D supplementation may help clarify whether low vitamin D status represents a modifiable risk factor or primarily reflects disease severity during acute infection, particularly in dengue-endemic, resource-limited settings such as Vietnam.
Conclusion
Lower serum vitamin D levels were linked to greater dengue severity in children from the Mekong Delta region of Vietnam, while common VDR gene polymorphisms showed no independent relationship with clinical outcomes. These findings point to a potential role of vitamin D status in pediatric dengue and support further investigation of its clinical relevance in endemic settings.
Supplemental Material
sj-docx-1-gph-10.1177_30502225261440423 – Supplemental material for Association of Serum 25-Hydroxyvitamin D and Vitamin D Receptor Gene Variants With Dengue Severity in Vietnamese Children
Supplemental material, sj-docx-1-gph-10.1177_30502225261440423 for Association of Serum 25-Hydroxyvitamin D and Vitamin D Receptor Gene Variants With Dengue Severity in Vietnamese Children by Hung Viet Phan, Hieu Lan Nguyen, Thuy Thi Dieu Nguyen, Ho Quoc Chuong and Phuong Minh Nguyen in Sage Open Pediatrics
Footnotes
Acknowledgements
We acknowledge the constant support from Can Tho University of Medicine and Pharmacy for this research. We also extend our gratitude to the Board of Directors of Can Tho Children’s Hospital and colleagues in the Pediatric Intensive Care Unit and Dengue Hemorrhagic Fever Department for helping with this study. We are deeply thankful to all of our participants for their invaluable contributions to this research.
Ethical Considerations
This study was conducted in strict adherence to the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Hanoi Medical University (Approval No. 1059/GCN-HMUIRB, dated January 19, 2024). Administrative permission to conduct the study was also granted by Can Tho Children’s Hospital.
Consent to Participate
Written informed consent was obtained from parents or legal guardians for their and their child’s participation before the study commenced.
Author Contributions
Concept and design: HVP, TTDN; data acquisition, analysis, and interpretation: HVP, PMN, HQC, HLN; drafting of the manuscript: HVP, PMN; critical review of the manuscript for significant intellectual content: PMN, TTDN, HLN. All authors approved the final version to be published and agreed to be accountable for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available due to restrictions imposed by regulations and contractual agreements. However, data supporting the findings of this article may be available upon reasonable request to the principal investigator, subject to case-by-case consideration.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.