
Abstract
Objectives
To investigate the relationship between vitamin D-related gene single nucleotide polymorphisms (SNPs) and hepatitis B-related liver cirrhosis.
Methods
This study included patients with chronic hepatitis B who were admitted to the Liver Research Center of the First Affiliated Hospital of Fujian Medical University from July 2012 to August 2016. SNPs rs1544410 and rs2228570 in the vitamin D receptor gene and rs2282679 in the vitamin D-binding protein gene were detected using the imLDR™ multiple SNP typing kit. Genotype and allele frequencies were compared between groups using the chi-square test or Fisher’s exact test.
Results
A total of 226 patients with hepatitis B virus (HBV) infection were enrolled, including 116 with HBV-related cirrhosis and 110 patients without. The distributions of vitamin D-related gene SNPs in both groups were in accordance with the Hardy–Weinberg equilibrium. There was no significant difference in the frequency or allelic distributions of rs1544410, rs2228570, and rs2282679 between the two groups. Additionally, the SNPs were not associated with the severity of cirrhosis.
Conclusion
No significant connection was identified between vitamin D-related SNPs and HBV-related liver cirrhosis.
Keywords
Introduction
Vitamin D is an important fat-soluble hormone with multiple effects. The synthesis of vitamin D begins with the production of pre-vitamin D3 (25-hydroxyvitamin D) after sunlight exposure. 25-hydroxyvitamin D in the circulation then binds to vitamin D-binding protein and is hydroxylated to 1,25-dihydroxyvitamin D3 (1α,25(OH)2D3), the active form of vitamin D, in the liver and kidneys. 1 1α,25(OH)2D3 combines with the vitamin D receptor (VDR) to execute its biological functions. 2 Besides its known effects in the skeletal system, 3 increasing evidence has revealed immunomodulatory, 4 anti-inflammatory, anti-proliferative, and anti-fibrotic roles for vitamin D, with the latter two exerted by vitamin D binding to VDR. 2
Liver cirrhosis (LC) is the final stage of various chronic liver diseases, especially chronic hepatitis B (CHB), which is prevalent in Asia.5,6 Vitamin D deficiency is common in patients with chronic liver diseases.7–10
Vitamin D-related genes, which may be involved in the synthesis or activation of vitamin D, are reported to associate with fibrosis in several liver diseases including viral hepatitis, 11 non-alcoholic fatty liver disease, 12 hepatocellular carcinoma, 13 and autoimmune liver disease.14,15 A possible role for vitamin D-related gene single nucleotide polymorphisms (SNPs) in HBV-related hepatocellular carcinoma was recently suggested. 16 However, the relationship between of vitamin D-related gene SNPs and HBV-related cirrhosis has not yet been studied. Therefore, we conducted the present study to explore the role of vitamin D-related gene SNPs in liver cirrhosis.
Methods
Patients
HBV-infected patients who were admitted to the First Affiliated Hospital of Fujian Medical University from July 2012 to August 2016 were included in this study if they had provided blood samples that could be used for SNP testing. Exclusion criteria were other causes of hepatitis, including hepatitis C virus, human immunodeficiency virus, Epstein–Barr virus, and cytomegalovirus infection, hepatocarcinoma, alcoholic steatohepatitis, nonalcoholic fatty liver disease, and other diseases that may influence liver fibrosis. The following data were collected from all patients: age, sex, white blood cell counts (WBC), HBV–DNA levels, the proportion of neutrophils (N%), liver and kidney function tests, prothrombin time, and the international normalized ratio (INR).
Diagnostic criteria
Chronic hepatitis B
CHB was diagnosed according to the 2009 update of American Association for the Study of Liver Diseases Practice Guidelines: 17 1) hepatitis B surface antigen (HBsAg)-positive for at least 6 months; 2) serum HBV-DNA greater than 100,000 copies/ml (>20,000 IU/ml), lower value 10,000 to 100,000 copies/ml (2,000–20,000 IU//ml) in hepatitis B e antigen (HBeAg)-negative CHB; 3) a persistent or intermittent elevation in alanine aminotransferase/aspartate transaminase (ALT/AST) levels; and 4) liver biopsy showing chronic hepatitis with moderate or severe necroinflammation.
Cirrhosis
Cirrhosis was diagnosed based on typical clinical features including a history of chronic liver disease, symptoms of chronic liver disease (i.e. ascites, varices, and hepatic encephalopathy), and/or imaging consistent with cirrhosis. Decompensated cirrhosis was defined as Child–Turcotte–Pugh (CTP) class B or C. 18
According to the presence of cirrhosis, patients were divided into cirrhosis and non-cirrhosis groups. Cirrhosis group patients were further divided into compensated and decompensated groups according to their CTP score on admission: CTP class A (scores 5–6), class B (scores 7–9), and class C (scores 10–15).
Sample collection
Peripheral blood samples were taken from all patients and peripheral blood mononuclear cells were separated by centrifugation at 1006.2 × g for 15 minutes and stored at −80°C. DNA was extracted from peripheral blood using a DNA purification kit (Axygen Biosciences, Union City, CA, USA). Three gene loci were chosen for study: rs2282679 of the vitamin D-binding protein gene (also known as the group-specific component (GC) gene), and rs1544410 and rs2228570 of the VDR gene.
Sample testing
SNP genotyping was carried out using the imLDR™ multiplex with primers listed in Table 1. The original database was analyzed by GeneMapper 4.1 software (Applied Biosystems, Foster City, CA, USA). Blood analysis was performed by the ADVIA 2120i automated hematology analyzer (Siemens Healthcare, Erlangen, Germany). Biochemical testing was carried out using an automatic biochemical analyzer (Siemens Healthcare, Erlangen, Germany). The blood coagulation function was detected by an STA automatic coagulation analyzer (Diagnostica Stago, Chausson, France).
Primers used to PCR-amplify vitamin D-related gene single nucleotide polymorphisms.

SNP, single nucleotide polymorphism.
Statistical analysis
Statistical analyses were performed by SPSS software, version 23.0. Continuous variables were represented as means ± standard deviation or medians (interquartile range) and compared using the t-test or the Mann–Whitney test, respectively. Categorical variables were expressed as counts (percentages), and differences in categorical variables were compared using the Chi-square test or Fisher’s exact test when the samples were limited in number. The Hardy–Weinberg equilibrium (HWE) was assessed in the study population using the SHEsis software platform (http://analysis.bio-x.cn). Genotype distributions were compared between cases and controls, and the results were reported as odds ratios (ORs) and 95% confidence intervals (CIs). A P value <0.05 was considered statistically significant.
Ethics
The study protocol was approved by the Institutional Ethics Committee of the First Affiliated Hospital of Fujian Medical University (IEC-FOM-013-1.0). Written informed consent was obtained from all participants. All methods were performed in accordance with the Declaration of Helsinki regarding ethical standards for research involving human subjects.
Results
Patient characteristics
A total of 226 patients with HBV infection were included in the study, of whom 116 had HBV-related cirrhosis. Of these 116, 64 (55.17%) had compensated cirrhosis and 52 (44.83%) had decompensated cirrhosis. No significant difference was found in sex, alanine aminotransferase (ALT), aspartate transaminase (AST), r-gamma-glutamyl transferase (r-GGT), creatinine, or N% between the two groups. Patient clinical characteristics and baseline laboratory data are shown in Table 2.
Patient demographic and clinical characteristics.
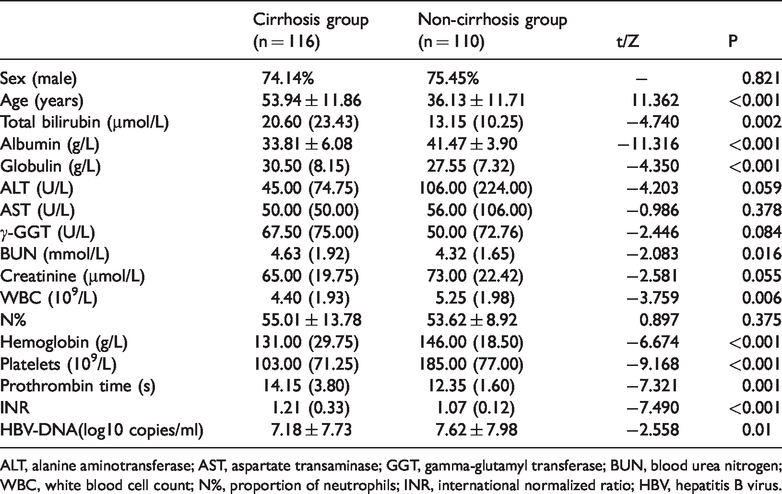
ALT, alanine aminotransferase; AST, aspartate transaminase; GGT, gamma-glutamyl transferase; BUN, blood urea nitrogen; WBC, white blood cell count; N%, proportion of neutrophils; INR, international normalized ratio; HBV, hepatitis B virus.
Vitamin D-related gene SNP genotype and allele frequencies
The distributions of vitamin D-related gene SNPs in the HBV-related cirrhosis and non-cirrhosis groups were all in accordance with the HWE. Genotype distributions and allele frequencies are listed in Tables 3 and 4. There was no significant difference in either the genotype of vitamin D-related gene polymorphisms or allelic distributions between the cirrhosis and non-cirrhosis groups.
Vitamin D gene genotypes.
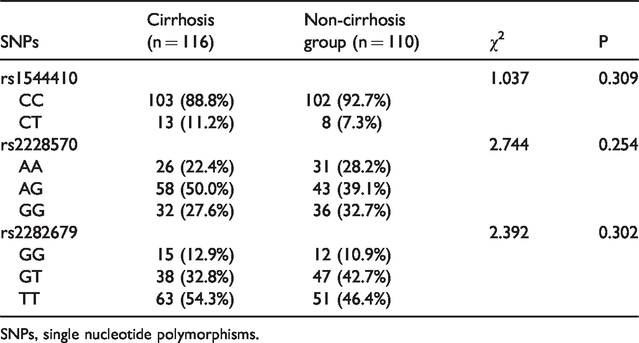
SNPs, single nucleotide polymorphisms.
Allele distribution between HBV-related cirrhosis and non-cirrhosis groups.
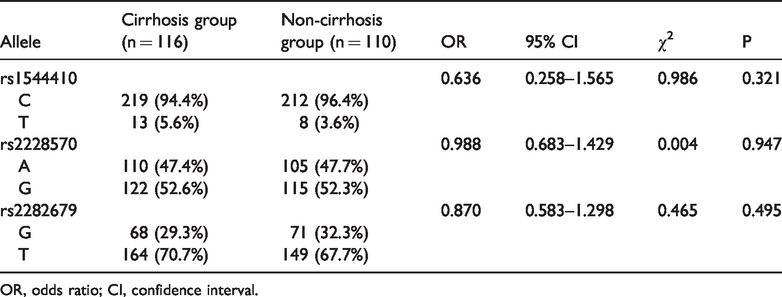
OR, odds ratio; CI, confidence interval.
The associate between vitamin D-related gene SNPs and cirrhosis progression
Patients with cirrhosis were divided into the compensated group and the decompensated group according to their CTP score. Patients with compensated cirrhosis had significantly lower age, globulin level, INR, and CTP, and significantly higher baseline albumin, hemoglobin, and platelet levels than those with decompensated cirrhosis (P < 0.05). There were no significant differences regarding sex, ALT, AST, r-GGT, total bilirubin, blood urea nitrogen, creatinine, WBC, N%, prothrombin time, or HBV-DNA between the two groups (Table 5). The distribution of genotypes was in accordance with HWE in both groups. There was no significant difference in the frequency of rs2282679, rs1544410, or rs2228570 genotypes or alleles (Tables 6 and 7).
Baseline characteristics of patients with compensated and decompensated cirrhosis.

ALT, alanine aminotransferase; AST, aspartate transaminase; GGT, gamma-glutamyl transferase; BUN, blood urea nitrogen; WBC, white blood cell count; N%, proportion of neutrophils; INR, international normalized ratio; CTP, Child–Turcotte–Pugh.
Genotype distribution of GC and VDR gene polymorphisms.

SNPs, single nucleotide polymorphisms.
SNP allele frequencies.

OR, odds ratio; CI, confidence interval.
Discussion
Vitamin D is increasingly recognized as playing anti-inflammatory and anti-fibrotic roles in various diseases. Moreover, previous studies showed a link between vitamin D-related gene polymorphisms and the development of several forms of liver diseases. However, the present study found no significant association between polymorphisms of the GC gene (rs2282679) and VDR gene (rs1544410 and rs2228570) and the risk of HBV-related cirrhosis in the Chinese population.
This negative result is supported by several studies. Arai et al. 19 reported that SNP rs2282679 was not associated with the severity of liver fibrosis in patients with biopsy-proven non-alcoholic fatty liver disease. Additionally, a meta-analysis of four studies with 357 primary biliary cirrhosis cases and 604 controls showed no association between SNP rs1544410 and disease risk. 20 In patients with CHB infection, SNPs rs2282679, rs1544410, and rs2228570 also showed no correlation with HBeAg seroconversion at 24 weeks after Peg-IFN therapy. 21 Similarly, SNPs rs2228570 did not affect the HBsAg clearance response to 48 weeks of Peg-IFN therapy in a Thai cohort. 22 Together with our own findings, these results provide clinical evidence for disputing the relationship between vitamin D-related gene polymorphisms and the progression of liver disease, as previously suspected. However, studies on different diseases and races may give entirely different results.
Indeed, a positive relationship between vitamin D-related gene SNPs and HBV-related liver diseases has previously been documented. 16 These discrepancies could be explained by a number of reasons. First, VDR and GC genes are highly polymorphic, 23 and a potential association between other GC and VDR SNP loci and HBV-related cirrhosis has been found by some studies. For example, variation in VDR rs7975232 and rs731236 is associated with a high HBV viral load and more severe fibrosis and necroinflammation. 24 Additionally, variation in genotype and allele frequencies of GC rs7041 was reported between HBV patients with hepatocellular carcinoma and healthy controls. 16 Second, the vitamin D function can be influenced by various genes and their polymorphisms, such as CYP2R1, DHCR7, and CYP27B1, 23 which were not assessed in our study. Third, there is known racial variation in the allelic frequency of VDR polymorphisms, 14 and because our study only investigated Chinese patients ethnic differences cannot be ruled out.
This study has several limitations. The sample size was relatively small, and the ethnic restriction to the Chinese population means that results should be interpreted with care for other populations. Finally, we mainly focused on gene expression, but the expression of encoded proteins is worthy of further study.
In conclusion, our results indicate that VDR and GC polymorphisms are not associated with the risk or severity of HBV-related liver cirrhosis in the Chinese population.
Footnotes
Authors' contributions
Su Lin and Yueyong Zhu conceived the study design; Shiying Liu and Yehong Lin performed data collection; Yueyong Zhu obtained funding; Su Lin and Yueyong Zhu administered the project; Yehong Lin and Jiali Wu obtained resources and carried out data analysis; Jiali Wu wrote the original draft of the manuscript; Su Lin, Mingfang Wang, and Bo Wan reviewed and edited the manuscript.
Consent
Verbal consent was obtained from the patients or their parents/carers for participation in the study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Disclaimer
The views expressed in the submitted article are our own and not an official position of the institution or funder.
Funding
This work was supported by the Fujian Medical University Departure Fund (grant no. 2018QH1047), the Medical Project of Fujian Province (grant nos. 2016-CX-33 and 2017J01187), the Health Commission Project of the Fujian Province Fund (grant no. 2018ZQN54), and the National Science and Technology Major Project of China (grant no. 2017ZX10202201-004-006).