
Abstract
This study aimed to determine the magnitude of premature mortality from sudden infant death syndrome (SIDS) in Ethiopia. The Global Burden of Disease data used to estimate the Years of life lost (YLLs) attributed to SIDS. The finding indicated 3153 YLLs rate per 100 000 infants (95% UI: 1569, 5206) attributed to SIDS, with 4278 YLLs per 100 000 males (UI: 2005, 7929) and 1972 YLLs per 100 000 females (UI: 774, 4406). The rate was higher in the first 5 months of life [5861 per 100 000 infants (UI: 2922, 9606)]. Lower than the national rate was estimated in Addis Ababa [1299 YLLs per 100 000 neonates (UI: 618, 2260)]. In conclusion higher YLL rate attributed by SIDS was found at the national and sub-national level, with infants in the first 5 months of life were disproportionately affected.
Introduction
Premature mortality is an indicator of unmet life expectancy and reflects a country’s health achievements, considering that many of the causes of premature mortality are preventable. 1 Global Health 2050 calls this goal “50 by 50,” a 50% reduction in premature death by 2050. An important milestone on the way to this goal would be a 30% reduction in premature mortality by 2035. 2 The probability of premature death (PPD)—the chance of dying before 70 years of age—was 15% in Western Europe and Canada, 22% in the US, 37% in India, and 52% in sub-Saharan Africa. 3 Sudden Infant Death Syndrome (SIDS) is defined as the sudden and unexplained death of an infant under the age of 1 year. 4 Mortality from sudden infant death is still a major contributor to mortality in the first year of life worldwide. 5 In 2021, the global estimated number of SIDS was 30 608 (95% UI: 17 810-41 094), corresponding to a mortality rate of 24.16 per 100 000 infants (95% UI: 14.06-32.44). 6 Evidence indicated that, the overall age-standardized premature mortality rate declined from 292.1 in 1994 to 162.4 in 2019 per 100 000 populations globally. Despite this decline in mortality rates, the total number of premature deaths is expected to rise by 22.8%, increasing from 272 815 deaths in the period from 2015 to 2019 to 334 894 deaths from 2040 to 2044 worldwide. 7 Ethiopia is implementing the Health Sector Transformation Plan since 2015 to support the implementation of universal health coverage and to attain Sustainable Development Goals.8,9 Evidence on premature mortality from sudden infant death is an important indicator to see disparities in availability and accessibility to health care, as well as health resource allocation across the regions. However, there is limited evidence on the magnitude of premature mortality attributed by sudden infant death in Ethiopia from 1990 to 2023. Up-to-date information on the premature mortality from sudden infant death in Ethiopia is also crucial to monitor progress towards the 2035 WHO global infant mortality reduction.
This study aimed to determine premature mortality, measured by years of life lost (YLLs), from SIDS by sex, age, and location in Ethiopia from 1990 to 2023, using the Global Burden of Diseases (GBD) 2023 study’s input data, methods, and protocol. Findings from this study could help policymakers design context-specific interventions to prevent premature mortality from SIDS in Ethiopia.
Methods
Study Setting
This study was conducted in Ethiopia, which was administratively classified into regional states at Amhara, Tigray, Afar, Oromia, Southern Nations, Nationalities, and Peoples (SNNP), Gambella, Harari, Somali, Sidama, Benishangul-Gumuz, and South West, and chartered city administrations at Addis Ababa and Dire Dawa. More than three-fourths, 80%, of the population resided in rural areas, where there was only limited access to child healthcare services. 10
Data Sources
The study used the GBD 2023 study data to estimate the YLLs from SIDS in Ethiopia, from 1990 to 2023. The explicit list of GBD 2023 study input datasets are available at: https://ghdx.healthdata.org/gbd-2023/sources.
Data Analyses
The cause of death ensemble model (CODEm) was employed to estimate YLLs from SIDS. The YLLs were a measure of premature mortality, and were determined by multiplying the number of mortality from SIDS by the standard life expectancy at the age of death. The study quantified 95% uncertainty intervals (UIs) to account for uncertainty inherent in the input data and statistical modelling processes. Variation in estimates across locations over time was smoothed by applying the spatiotemporal Gaussian process regression (ST-GPR). The overall increase or reduction in age-standardized rates over the entire study duration, 1990-2023, was calculated by comparing the values at the start (1990) and end (2023) of the period, using the following formula:
Ethical Approval and Informed Consent
This study was conducted as part of the GBD Collaborators Network and adhered to the GBD protocol, which is found at: https://www.healthdata.org/research-analysis/about-gbd/protocol.
The study used secondary data from Global Burden of Diseases 2023 study. Moreover, the estimates were aggregated at the population level so that individual-level data were adequately anonymized to ensure confidentiality of information. Therefore, ethical informed consent for participation was not required for this study.
Results
Years of Life Lost
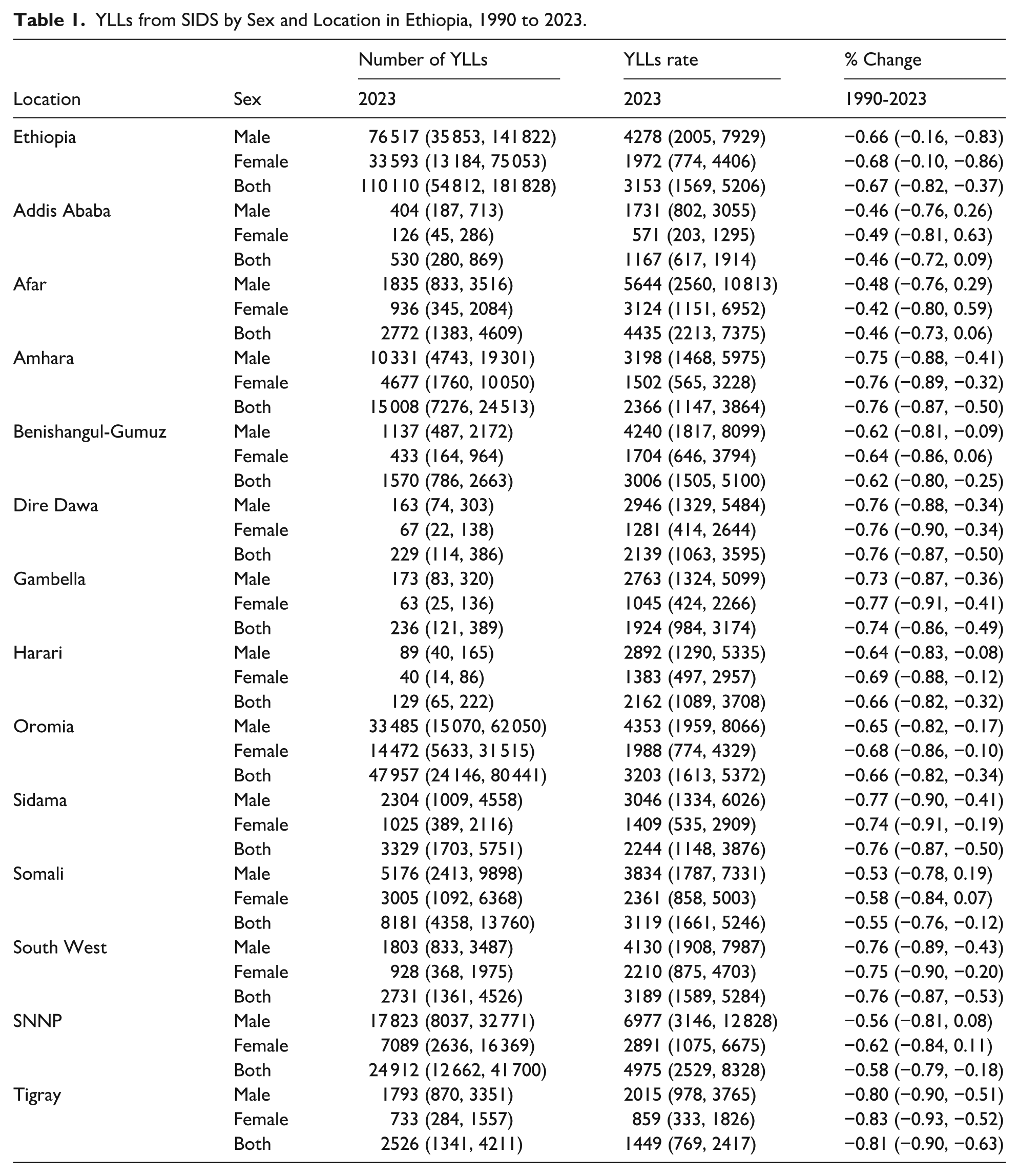
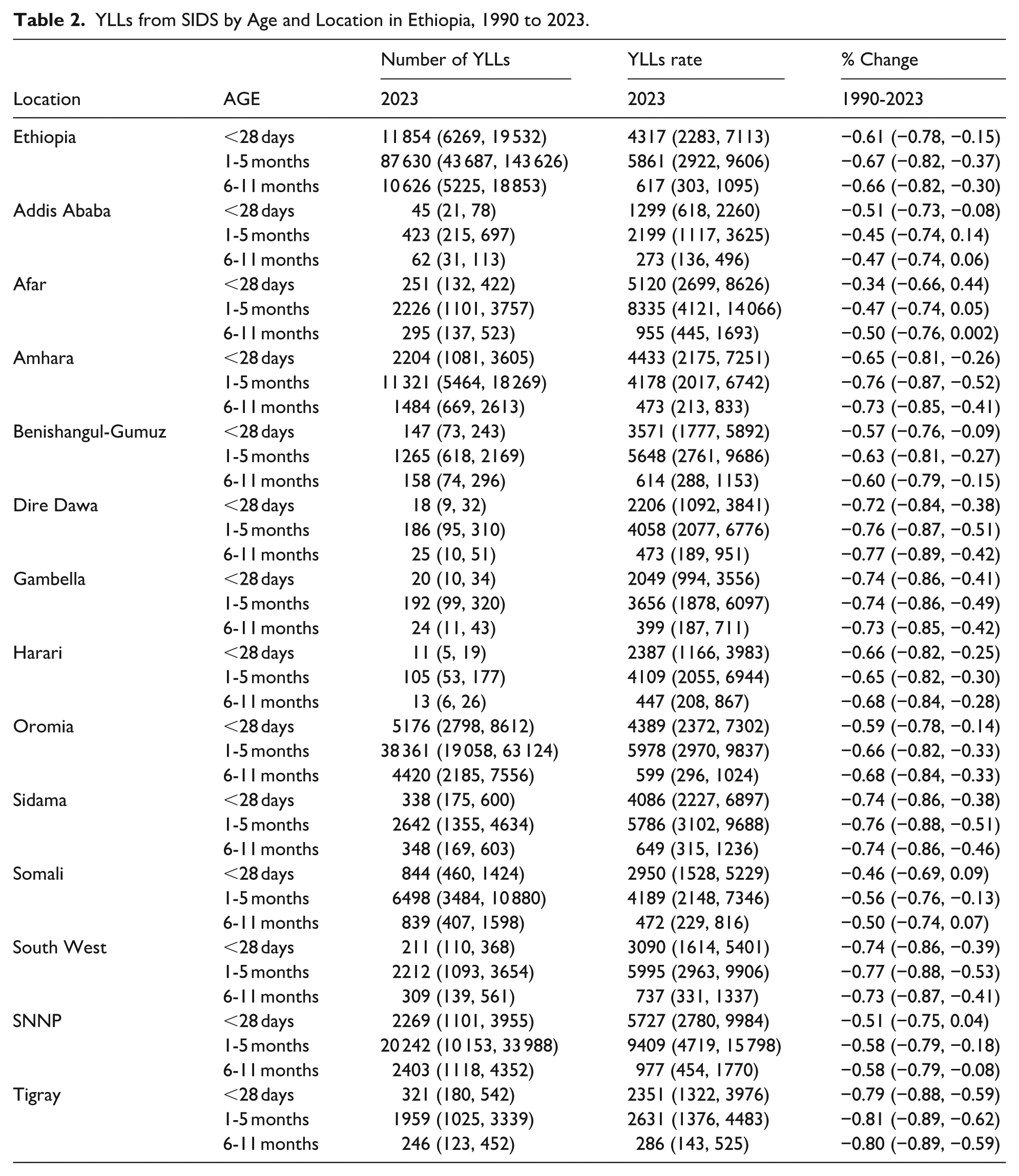
There were a total of 110 110 YLLs from SIDS (95% UI: 54 812, 181 828) in Ethiopia in 2023, with 76 517 YLLs among males (95% UI: 35 853, 141 822) and 33 593 YLLs among females (95% UI: 13 184, 75 053). This was equivalent to an estimated 3153 YLLs per 100 000 infants (95% UI: 1569, 5206), with 4278 YLLs per 100 000 males (95% UI: 2005, 7929) and 1972 YLLs per 100 000 females (95% UI: 774, 4406). Moreover, the rate was estimated to be higher in the first 5 months of life. However, lower than the national rate of YLLs among neonates [4317 YLLs per 100 000 neonates (95% UI: 2283, 7113)] was estimated in Addis Ababa [1299 YLLs per 100 000 neonates (95% UI: 618, 2260)]. From 1990 to 2023, with the exception of Addis Ababa (all age group infants), Afar regions (all age group infants), Somali (among < 28 days, and 6-11 months infants), and SNNP (among < 28 days infant), there is a notable decrease in the percentage of YLL rate change at the national and sub-national levels (Tables 1 and 2 and Figures 1 and 2).
YLLs from SIDS by Sex and Location in Ethiopia, 1990 to 2023.
YLLs from SIDS by Age and Location in Ethiopia, 1990 to 2023.

Sex-location specific YLL rates from sudden infant death syndrome in Ethiopia, 2023.
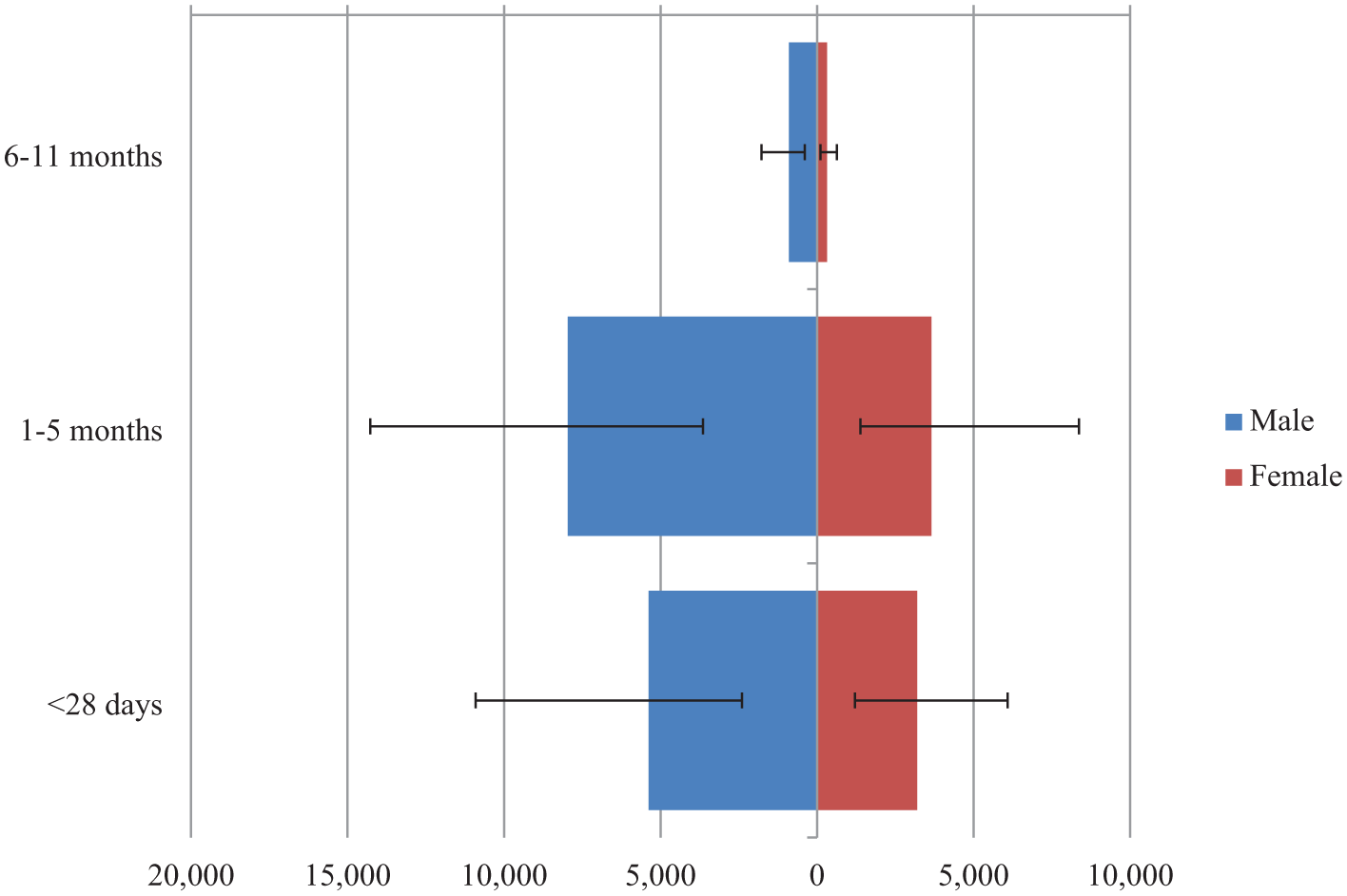
Age-sex specific rate of YLLs from SIDS in Ethiopia, 2023.
Discussion
This study aimed to determine the YLL rate from SIDS by sex, age, and locations in Ethiopia from 1990 to 2023. This study accounted for a total of 3153 YLLs per 100 000 infants (95% UI: 1569, 5206), with 4278 YLLs per 100 000 males (95% UI: 2005, 7929) and 1972 YLLs per 100 000 females (95% UI: 774, 4406). The YLL rate was estimated to be higher in the first 5 months of life. Additionally, lower than the national rate of YLL among neonates [4317 YLLs per 100 000 neonates (95% UI: 2283, 7113)] was estimated in Addis Ababa [1299 YLLs per 100 000 neonates (95% UI: 618, 2260)]. From 1990 to 2023, except Addis Ababa (all age group infants), Afar regions (all age group infants), Somali (among < 28 days, and 6-11 months infants), and SNNP (among < 28 days infant), there is a notable decrease in the percentage of YLL rate change at the national and sub-national levels in 2023 compared to 1990.
The YLL rate due to SIDS in this study is more or less similar to the YLL rate of sub-Saharan Africa and specifically with Eastern sub-Saharan Africa region. However, it is higher than the global YLL rate. Compared to the rate in 1990, there was a remarkable decline in the rate of YLLs at national and subnational levels. However, the estimated YLLs rates are still high, suggesting the necessity of effective interventions like safe sleep practices, maternal education, and strengthening new-born care within the national health system.11-13 This study indicated the necessity of effective interventions to reduce the existing higher burden of premature mortality from sudden infant death syndrome at national and subnational levels.13,14
In addition, in this study YLL rate due to SIDS was estimated to be higher in the first 5 months of life. This finding is supported by other study. 15 This could be due to the unsafe sleep practice, and the poor ability to respond to breathing challenges in this early infancy period. To address the higher YLLs rate due to SIDS interventions focussing prevention and management of SIDS, targeting infants aged 1 to 5 months are crucial.13,16-18
Additionally, the findings of this study showed that there was variation in the YLLs rate due to SIDS across the infant age categories nationally and across the regional states. Lower YLL rate due to SIDS among neonates was estimated in Addis Ababa compared to national YLL rate estimate. The possible reason for the lower YLL rate from SIDS in the capital city (Addis Ababa) compared to the other regional states could be due to the improved access and quality of maternal and infant care, better socioeconomic and cultural practices, and other public health interventions. Investigating the risk factors for higher YLL rate estimates in Addis Ababa is fundamental to addressing the gap and re-designing intervention accordingly. Moreover, the difference across regions indicates policy makers to provide special interventions in the prenatal and neonatal healthcare services. It is crucial to address the environmental, maternal, infant, and other modifiable behavioural factors which predispose the occurrence of SIDS.19-21
The study has revealed that there was a notable decrease in the rate of YLLs from SIDS at the national and sub-national levels in 2023 compared to the rate in 1990. Nevertheless, the rate remains unchanged in Addis Ababa, Afar, Somali, and SNNP. This calls redesigning appropriate new interventions and implementation strategies to improve the poor progress in reducing the YLL rate in these locations. Moreover, Context-specific interventions focussing low resource settings are crucial to improve to improve the well-being of infants.
Not having individual-level data restricted our capacity to provide a detailed discussion on specific risk elements, such as genetic predispositions, nutrition, and socio-environmental influences of SIDS. Despite these limitations, this study is of great significance in that it is the first study to analyse the YLLs rate due to SIDS nationally and sub-nationally.
Conclusion
Finding of this study showed there was a significant change in the rate of YLL from SIDS, similarly this study showed higher YLL rates from SIDS at the national and subnational levels in Ethiopia, with infants in the first 5 months of life disproportionately affected. Additionally, this study showed variation in the YLL rate due to SIDS across the infant age categories nationally and across the regional states. Despite a notable decrease in the percentage change in YLL at the national level, subnationally there was a variation in the percentage of change between the year 199o to 2023. In order to lower SIDS, proven context-specific preventative strategies are essential, particularly for these areas where the decline in SIDS has been slow. Providing education for SIDS prevention in the population is crucial to reduce the burden. Safe sleep practices, maternal education, and strengthening new-born care within the national health system can be recommended.
Footnotes
Acknowledgements
The Institute for Health Metrics and Evaluation under the University of Washington are acknowledged by the authors for their contribution to the Global Burden of Diseases collaborative initiative.
Author Contributions
AKB and ST conceived and designed the study. AKB, YBT, HHA, ZT, TG, ETW, KL, MG, GN, ST were involved in the analysis and interpretation of the findings. All authors have approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.