
Abstract
Keywords
Introduction
In 2016, the American Academy of Pediatrics (AAP) recommended a safe sleep environment to reduce the risk of sleep-related infant deaths, including sudden infant death syndrome (SIDS), ill-defined deaths, and accidental suffocation and strangulation in bed. The AAP recommendations include room-sharing without bed-sharing, supine positioning, a firm sleep surface, breastfeeding, and the avoidance of soft bedding, overheating, and exposure to smoke, alcohol, and illicit drugs. 1
Bed-sharing is defined as the sleeping of an infant on the same surface as another person. 2 Bed-sharing is associated with an increased risk of SIDS 3 and also with an increased risk of conditions associated with SIDS. 2 A national study of infant sleeping practices reported that 13.5% of parents usually bed-shared, and 46% of parents reported that they have shared a bed at some time with their infant (age 8 months or younger) in the previous 2 weeks. 4 Our previous study reported that 6.3% of parents share a bed with their infant in the first week of life. 5
While breastfeeding is recommended to lower the risk of SIDS, 1 it is also a risk factor for increased bed-sharing. 6 In our previous study, breastfeeding was identified as an independent risk factor for increased rates of bed-sharing among maternal-infant dyads who delivered at a large urban academic health center. 5
Since 1938, the Finnish government has supplied mothers with a maternity package: a cardboard bassinet, which also contains baby supplies. The box itself doubles as a sleeping space for the infant. 7 No studies have examined the effect of the distribution a Finnish-style cardboard bassinet on the rates of infant bed-sharing.
This study was undertaken to measure the effect of a postpartum safe infant sleep educational program that included the use of a cardboard bassinet on the rates of bed-sharing in the first week of life, in maternal-infant pairs in general, and those dyads that exclusively breastfed.
Methods
Patients and Data Collection
Women who delivered at Temple University Hospital (vaginal and cesarean births) between January 1, 2015, and November 15, 2016, were discharged from the hospital with their infant, and had a phone number listed in the medical record were eligible for enrollment. Attempts were made to contact each subject within 72 hours of discharge. If the first attempt was unsuccessful, daily attempts to contact the subject were made over the next 3 days. Interviews consisted of general questions regarding the hospital stay as well as the need for follow-up appointments, what method of feeding the mother employed, if feeding issues existed, whether the mother had enrolled in the state women, infants and children supplemental nutritional program, and the presence of additional health issues or concerns. To determine infant and parental sleep behaviors, the following questions were also included:
1. Are you having any trouble feeding your baby?
2. Where does your baby sleep: crib, bassinet, Pack and Play, or other?
3. Does your baby sleep on his/her back, side, belly, or all of these?
4. Do you ever fall asleep with your baby in the same bed, couch, or chair?
5. Has a doctor ever talked to you about sleeping with your baby?
In the intervention group, the option for question 2 included a cardboard bassinet as a response and the following questions were also asked:
6. Do you use the “cardboard bassinet” you were given in the hospital? a. If yes: Do you use it as a bed for the baby? b. If no: Do you use the “cardboard bassinet” for any other purpose?
7. If you are breastfeeding, does the “cardboard bassinet” make breastfeeding easier, or harder, or the “bassinet” makes no difference?
8. Were you happy you received a “cardboard bassinet” from the hospital?
Educational level, smoking status, and method of infant feeding were recorded. Maternal age was obtained from the medical record. If the answer provided by the respondent for any question required input from a clinician, then the call was referred to a registered nurse to provide clinical input.
The primary outcome of interest was self-reported bed-sharing during the first week of life (question 4).
Study Design
This study was designed as a prospective, controlled, interrupted time series. 8 The subjects were divided into 4 separate groups. Two patient groups in aggregate were designated as the control group, and 2 aggregate groups were designated as the interventional group.
Control 1 (C1) consisted of mother-infant dyads enrolled between January 1, 2015, and October 31, 2015. These subjects received standard discharge instructions that addressed safe newborn sleep practices, umbilical cord care, and bathing, as well as anticipatory guidance regarding feeding, stooling, and voiding. This group was the sample for a previous study that described bed-sharing rates and risk factors for neonatal bed-sharing. 5
Control 2 (C2) consisted of subjects enrolled between November 1, 2015, and February 7, 2016, inclusive. These mothers received the same standard discharge instructions as C1.
Intervention 1 (I1) consisted of subjects enrolled between February 8, 2016, and May 3, 2016, inclusive. Prior to hospital discharge, these patients received additional safe infant sleep education based on the AAP safe infant sleep recommendations 1 delivered in person by a select group of registered nurses, under the direction of a pediatrician; visitors and family members were encouraged to attend the educational session. To reinforce infant safe sleep, each mother was given a summary of the teaching points on a laminated door hanger. The sessions were provided in the preferred language of the mother, using interpreter services as necessary.
Intervention 2 (I2) consisted of mother-infant dyads who delivered between May 4, 2016, and November 15, 2016. In addition to the sleep-specific educational session provided to I1, a cardboard bassinet was provided for the use of each infant at the time of discharge (purchased from The Baby Box Company; http://www.babyboxuniversity.com). Each box was made of cardboard, had a firm, nontoxic foam mattress, and a cotton fitted sheet (26¾ × 16¾ × 11½ inches; Figure 1). The cardboard bassinets meet or exceed all applicable tenets of the CPSC, Health Canada, and EN standards. 9 Each box also contained baby supplies (purchased or obtained separately from the boxes): a onesie, hat, wearable blanket, thermometer, nasal aspirator, baby wash, diapers, baby wipes, 1 pair of socks, children’s book about safe sleep, condoms, immunization card, list of community resources (including information on programs for free portable cribs), information on free smoke detector installation from the Philadelphia Fire Department, safety tips from the Philadelphia Police Department, and a pamphlet addressing breastfeeding and/or formula feeding tips. The purchase of the bassinets and their contents was funded by the W. K. Kellogg Foundation, Kohl’s Cares for Kids, and the Temple University OwlCrowd Campaign.

Cardboard bassinet distributed to patients.
Prior to bassinet distribution, each mother watched a 3-minute instructional video on the use of the bassinet, provided in English or Spanish; translational services were provided for those who preferred other languages.
The aggregate control group consisted of groups C1 and C2, and the aggregate interventional group consisted of I1 and I2. Subsets of women who exclusively breastfed from groups C1, C2, I1, and I2 were designated as groups C1B, C2B, I1B, and I2B, respectively.
Statistical Analyses
The primary outcome of interest was the bed-sharing rate. Since our previous study demonstrated that mothers who exclusively breastfed their infants had higher rates of bed-sharing in the first 8 days of life, an analysis of this subgroup was planned as noted above. Other outcomes of interest included the proportion of infants without an identified place to sleep (question 2—other) and the proportion of infants who slept on their backs (question 3).
A control group of 1261 subjects (C1) had already been studied and reported in detail. 5 Since the self-reported rate of bed-sharing in this group was relatively low (6.3%), a total sample size of 2896 subjects was required to detect a bed-sharing rate of 4.0% in the intervention group with 80% power. Since the nature of the interventions precluded a parallel study design, a time series was used. To maximize the number of subjects in the control group by including those subjects already reported, a Bayesian approach was undertaken. Briefly, the probability mass functions for C1 and I1 were modeled as β distributions and used as prior probabilities; additional control (C2) and intervention data (I2) were modeled using a binomial distribution. As a result, the posterior probability mass functions also could be modeled as β distributions.
To compute the rate ratios between the 2 groups as well as the 95% credible intervals and the probability that the rate ratio exceeded 1 (P(Θ > 1|X = pc/pi), where Θ = the true ratio of proportions), the posterior distribution of each proportion (pc = proportion of aggregate controls; pi = proportion of aggregate intervention) was sampled one value at a time. The ratio was calculated and the value was retained. This process was reiterated 100 000 times, without replacement, to simulate the posterior distribution of pi/pc. From this vector, the mean and 95% credible intervals of the simulated sample were calculated and the percentage of values in the sample >1 were determined. Calculation of P(Θ > 1|X = pc/pi) was also directly determined from the data using the method of Proschan et al. 10 The function for determining the 95% credible interval from a simulated distribution was from Kruschke. 11
All calculations and data cleaning were performed in R using the readxl, lubridate, xts, and basic packages.
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board of Temple University (Protocol Number 22996). Informed consent was obtained verbally before participation.
Results
All Subjects
Calls were made to 5187 mothers between January 1, 2015, and November 15, 2016; 2763 respondents completed the interview. For C1, 2386 calls were made and 1264 surveys completed (53%). In C2, 740 calls were made and 423 surveys completed (57%). In I1, 632 calls were made and 391 surveys completed (62%). In I2, 1429 calls were made and 685 surveys completed (48%).
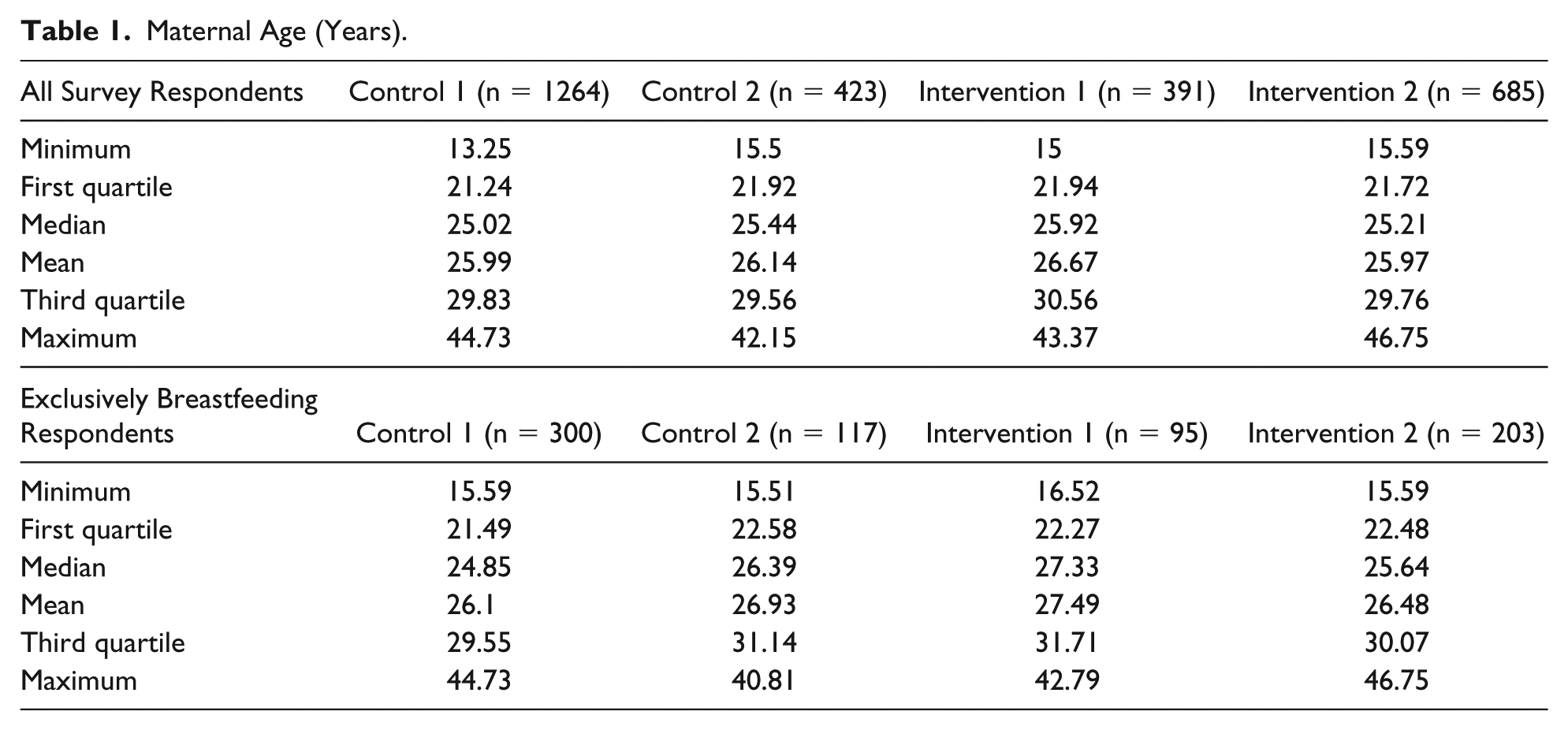
The demographics of the 4 different study groups are shown in Tables 1 and 2. The median age for C1 and C2 was 25.02 and 25.44 years, respectively (interquartile ranges = 21.24-29.83 and 21.92-29.56 years, respectively). The median age for I1 and I2 was 25.92 and 25.21 years, respectively (interquartile ranges = 21.94-30.56 and 21.72-29.76 years, respectively). The percentage of mothers who did not graduate high school was 29% greater in the combined control group (C1 + C2; pc/pi = 1.29; 95% credible interval = 1.14-1.43, P(Θ > 1|X = pc/pi) > .999). The proportions of subjects who smoked, breastfed, reported feeding issues, or had a clinical concern were similar among all groups.
Maternal Age (Years).
Survey Responses for All Mothers.

Abbreviations: CL, credible interval; pc, posterior simulated proportion for Control 1 prior : Control 2 prior with 100 000 repetitions; pi, posterior simulated proportion for Intervention 1 prior : Intervention 2 prior with 100 000 repetitions; LCL, lower credible limit; UCL, upper credible limit.
The survey results are shown in Table 2. Compared with infants in the interventional group (I1 + I2), fewer infants in the control group slept on the back (pc/pi = 0.987; 95% credible interval = 0.972-1.0; P(Θ > 1|X = pc/pi) = .047); bed-sharing was more common among control infants (pc/pi = 1.34; 95% credible interval = 0.922-1.79; P(Θ > 1|X = pc/pi) = .955). Significantly more mothers in the intervention group identified an infant sleeping place other than a crib, bassinet, or Pack and Play (pc/pi = 0.584; 95% credible interval = 0.289-0.939; P(Θ > 1|X = pc/pi) = .023).
Subjects Who Exclusively Breastfed
The results for the breastfeeding subset are shown in Tables 1 and 3. Groups C1B (N = 300), C2B (N = 117), I1B (N = 95), and I2B (N = 203) consisted of infants who were exclusively breastfed from groups C1, C2, I1, and I2, respectively. The median age of C1B and C2B was 24.85 and 26.39 years, respectively (interquartile ranges = 21.49-29.55 and 22.58-31.14 years, respectively). The median age for groups I1B and I2B was 27.33 and 25.64 years, respectively (interquartile ranges = 22.27-31.71 and 22.48-30.07 years, respectively). The percentage of mothers who did not graduate high school was 45% greater in the control group (pc/pi = 1.450; 95% credible interval = 1.05-1.890; P(Θ > 1|X = pc/pi) = .994). The proportion of subjects who smoked, reported feeding issues, or a clinical concern were similar among all groups. Compared with respondents in the aggregate intervention group, fewer mothers in the aggregate control group reported adequate safe sleep teaching (pc/pi = 0.308; 95% credible interval = 0.264-0.35; P(Θ > 1|X = pc/pi) < .001). Bed-sharing was more common in the control group than the intervention group (pc/pi = 2.00; 95% credible interval = 1.01-3.15; P(Θ > 1|X = pc/pi) = .993). The proportion of subjects who reported that the infant slept somewhere other than a crib, bassinet, or Pack and Play was similar between the 2 groups (pc/pi = 0.713; 95% credible interval = 0.163-1.440; P(Θ > 1|X = pc/pi) = .174).
Survey Responses for Exclusively Breastfeeding Mothers.

Abbreviations: CL, credible limit; pc, posterior simulated proportion for Control 1 prior : Control 2 prior with 100 000 repetitions; pi, posterior simulated proportion for Intervention 1 prior : Intervention 2 prior with 100 000 repetitions; LCL, lower credible limit; UCL: upper credible limit.
Acceptance of the Cardboard Bassinet
Of the 1429 dyads who received the cardboard bassinet and a phone call, 685 responded to questions addressing acceptance of the cardboard bassinet (Table 4). Ninety-two percent (631/685) of the recipients used the cardboard bassinet in one way or another. The bassinet was used as a sleeping space by 51% (349/685) of the recipients; 12% (82/685) used the cardboard bassinet as the primary sleeping space for their infant. Of respondents who answered the question regarding satisfaction with the receipt of a cardboard bassinet, 99% (659/668) of respondents were “happy” that they received the cardboard bassinet.
Acceptance of the Cardboard Bassinet.

Of the 685 respondents, 199 exclusively breastfed their infants (Table 4). In this subset, 92% (184/199) of the breastfeeding respondents used the bassinet; 52% (104/199) used the bassinet as a sleeping space; and 11% used the bassinet as the primary sleeping space. Of the 104 recipients who used the bassinet as a sleeping space, 63 (60%) responded the bassinet makes breastfeeding easier.
Discussion
Bed-sharing is a common practice that increases the risk of SIDS and the exposure to conditions associated with an increased risk of SIDS. 2 To decrease the risk of all sleep-related deaths, the AAP safe sleep environment recommendations include room-sharing without bed-sharing, a firm sleep surface, supine positioning, and breastfeeding. 1 In 2003, the Chicago Infant Mortality Study reported an increased risk of SIDS associated with bed-sharing with parent(s) alone (odds ratio [OR] = 1.9; 95% confidence interval [CI] = 1.2-3.1) and bed-sharing in other combinations (OR = 5.4; 95% CI = 2.8-10.2). 12 A meta-analysis of 11 studies demonstrated an association of bed-sharing and SIDS (OR = 2.88; 95% CI = 1.99-4.18). 3 A cross-sectional study of sleep-related infant deaths from 24 states concluded that bed-sharing was the predominant risk factor for SIDS among infants aged 0 to 3 months. 13 The present study suggests that the distribution of a cardboard bassinet and face-to-face postpartum safe infant sleep education reduces infant bed-sharing in the first week of life.
Breastfeeding reduces the risk of SIDS. A meta-analysis of 24 case-control studies reported a summary OR of 0.55 (95% CI = 0.44-0.69) for SIDS in breastfed versus non-breastfed infants. Breastfeeding lowered the risk of SIDS, and exclusive breastfeeding increased this protective effect. 14 However, multiple studies have demonstrated an association between breastfeeding and increased rates of bed-sharing. Smith et al sampled a national cohort of 3218 new mothers from 32 representative hospitals between 2011 and 2014; 30.5% of the mothers exclusively breastfed their infants while 29.5% reported intermittent breastfeeding. 6 While the majority of mothers reported room-sharing without bed-sharing, infants who exclusively or intermittently breastfed were significantly more likely to bed-share (OR = 2.46 and 1.75, respectively) compared with formula-fed infants. Among the 1261 mother-infant dyads in Control 1 of the current report, infants who were exclusively formula-fed were significantly less likely to bed-share than those infants who were intermittently or exclusively formula-fed (OR = 0.4; 95% CI = 0.2-0.77). 5 The present study demonstrated that within the first 8 days of life, face-to-face safe infant sleep education and provision of the cardboard bassinet cut the rate of bed-sharing among exclusively breastfed infants almost in half.
To date, no studies have formally assessed the acceptance of a Finnish-style cardboard bassinet in an American population. In the present study, a majority of bassinet recipients used it as an infant sleeping space. A majority of exclusively breastfeeding mothers reported that the cardboard bassinet facilitated breastfeeding. Patient satisfaction with the distribution of the bassinet was high.
This study has several limitations. First, the low number of surveys completed in each group (53%, 57%, 62%, 48% response rates in groups C1, C2, I1, I2, respectively) may have introduced bias into the study. The degree of bias is difficult to assess since at least 3 attempts were made to contact each mother who delivered during the study period. Self-reporting is a second source of bias. Using video recordings to observe the activity, one study examined bed-sharing over the first 6 months of life. The study found an overall rate of 22% and 16% at 3 and 6 months of age, respectively. 15 This rate is substantially higher than the rates noted in the present study determined in the first week of life. While this may represent a true difference, it is also possible that the risk of bed-sharing increases over time. Finally, while the intervention described in this report reduced bed-sharing in the first 8 days of life, it is not known if the combination of face-to-face education and distribution of a cardboard bassinet will reduce bed-sharing throughout the first 4 to 6 months of life.
Conclusions
Face-to-face safe sleep education and the provision of a cardboard bassinet with a firm mattress and fitted sheet reduced the rate of bed-sharing in the first 8 days of life. This intervention had its greatest impact on a population at increased risk for bed-sharing: exclusively breastfed infants. Future studies are needed to determine (1) if the effect of this intervention is sustainable throughout the first 6 months of life; and (2) if this intervention can significantly reduce the incidence of sleep-related death in large populations over time.
Footnotes
Acknowledgements
The authors thank Lornajane Braunsar, BSN RN (Nurse Manager of Maternity), the Maternity Unit nurses and staff and Temple Access Center employees for their hard work and contributions to the SAFE-T Program.
Author Contributions
MH: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
BM: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JA: Contributed to conception and design; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JR: Contributed to conception and design; contributed to acquisition; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SA: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.