
Abstract
Objective. Despite educational outreach, bed-sharing prevalence is rising. Mothers’ and fathers’ bed-sharing practices, prevention message source, perceived source credibility, and the effectiveness of the prevention message were evaluated. Methods. Data were collected from 678 community parents via an online survey. Results were analyzed using descriptive statistics and phi tests. Results. Bed-sharing reasons focused on comfort and ease. Mothers were more likely to receive prevention messages from individual professionals or organizations, whereas fathers were more likely to hear prevention messages from spouses/coparents and grandfathers. Physicians were the most common source, and physicians and grandmothers were rated as the most credible and effective. Conclusions. Prevention message source varies between mothers and fathers, highlighting the need for continued research with fathers. Grandmothers and physicians are effective and credible sources of prevention messages. Although less frequent, prevention messages from grandmothers were most effective. There was no evidence of effective messages from educational campaigns.
Infant mortality related to bed-sharing, sharing a sleep surface (eg, bed, couch, chair) with another person, is preventable. Bed-sharing has long been recognized as a risk factor for sleep-related deaths 1 and is uniquely associated with multiple known sleep-related death risks, including a nonfirm sleep surface, loose bedding and sheets, close proximity to an individual who may smoke, and intoxication of an adult bed-sharer. 2 In 2015, an estimated 900 infants died of accidental suffocation and strangulation in the United States. 3 As the single greatest risk factor of sleep-related death in the first 4 months of life, 69% of infants who died in their sleep were bed-sharing at the time. 2
In response to sleep-related infant deaths in the United States, the American Academy of Pediatrics (AAP) has attempted to increase awareness of the potential dangers associated with bed-sharing by highlighting this risk in their recommendations to reduce infant death. 1 In their recommendations, the AAP states that infants should sleep on a separate, but proximate, sleep surface. In line with the AAP, the current consensus of public health professionals is to discourage bed-sharing and advocate room-sharing, where an infant sleeps in the same room but not on the same sleeping surface as a caregiver.4-6
However, these recommendations are not having their intended impact on common practice, as the reported prevalence of bed-sharing is still rising. Indeed, bed-sharing increased by approximately 10% from 1993 to 2010 in the United States. 7 It is plausible that the rise may be due to uninformed parents or contradictory messages related to bed-sharing. For example, Eisenberg and colleagues 8 found that 50% of mothers reported no physician advice on infant sleep location, and even when advice was provided, conflicting advice was also received from family or the media. Additionally, Ball and Volpe 9 found parents may reject advice against bed-sharing from professionals when it differs from their own beliefs. Due to the limited impact of current prevention efforts, it is imperative to understand parental decision-making processes regarding bed-sharing.
Despite the frequent suggestion that culture is a primary reason for bed-sharing, the practice of bed-sharing is common across many cultures and races/ethnicities. 10 Approximately 50% to 70% of US mothers report bed-sharing with their infants, whether purposefully or accidentally.10-12 Similar rates of bed-sharing have been reported globally. 10
Health Messaging
Prevention message source, source credibility, and, ultimately, the source’s effectiveness at preventing or reducing bed-sharing behavior should be considered. 13 General health information typically comes from health care professionals, public health campaigns, the media, and close relatives and friends.13,14 Advice regarding bed-sharing comes from various sources 14 as well, although prevalence rates of bed-sharing prevention messages are unclear.
Furthermore, message credibility may vary depending on source. Individual family physicians and other health care providers are often rated as the most reliable and credible source of general health information.13-15 Hwang and colleagues asked parents about maternal trust in various sources on bed-sharing, infant sleep position, pacifier use, feeding, and vaccinations. 14 Trust of sources including nurses (range 23% to 41%), family members (range 30% to 55%), friends (range 13% to 22%), and the media (range 10% to 14%) was lower than that of physicians (range 56% to 89%). Furthermore, maternal trust in physicians, while high overall, varied depending on the specific topic. 14 For instance, the prevalence of maternal trust in physicians’ advice regarding infant sleep position was 80%, whereas advice regarding bed-sharing was only 60%. This study also highlights differential levels of trust within the health profession. Other research has shown that health care organizations, which often produce information packets or brochures, are often not deemed as credible. 16
Although trust in media was low in Hwang and colleagues’ study on infant care practices, trust in media sources varies. When limited to information found on the Internet, the media is often deemed credible. More than half of the US population uses the Internet to look up health information. 17 More than 70% of adults reported they trusted health information found on the Internet and equal numbers stated the information they found online influenced their health behavior. This is particularly concerning because Chung and colleagues 17 found much of the information available on the Internet about safe infant sleep is inaccurate and inconsistent with the AAP’s safe sleep guidelines. As previously indicated, other studies suggest that despite the high consumption of health information from mass media, trust is generally moderate to low.14,18 This disparity may be due to unclear definitions of the “media.” For instance, Chung and colleagues 17 specifically looked at Internet sources, whereas Hwang and colleagues 14 simply asked about trust in the “media.” Importantly, information found on the Internet is likely to have been sought by the user and may come from various sources (eg, health organization websites, physicians, parent blogs, or friend/support groups). Specifying the Internet as one broad category may limit the utility of any information gathered. Furthermore, separating out various specific types of media (ie, brochure; story in newspaper or magazine; TV news story; or bus, billboard, or other public advertisements) may help identify differences in prevention messaging based on media source.
Knowing the types of prevention message sources and perceived credibility of each source is an important step. However, determining the effectiveness of a prevention message source is, arguably, the most important factor to consider in reducing bed-sharing. It is necessary to understand whether people modify their behavior following others’ recommendations. Previous research shows that individuals are more likely to heed advice from sources they trust.19,20 Although compliance with physician recommendations is generally high, advice against bed-sharing specifically may not alter bed-sharing behavior. 17 Hackett and Simons 20 found that how the advice was received by the parent significantly influenced adherence to the safe sleep guidelines. Furthermore, even when targeted prevention messages for African American mothers were used, there were no notable differences in adherence to the safe sleep guidelines. 21 This overall low adherence may be because parents believe clinicians have a professional obligation to recommend against bed-sharing, even if these clinicians personally support bed-sharing. 22 Knowing the most effective prevention message source may determine the most effective intervention and this vary based on parent gender.
Incorporating Fathers in Research on Bed-Sharing
Paternal involvement is associated with higher maternal prenatal care usage, abstinence from both alcohol and smoking during pregnancy, and overall better infant sleep quality.23,24 The majority of infant sleep literature, and specifically literature on bed-sharing prevention, focuses on mothers with less attention given to the beliefs/behaviors of fathers.11,14,25,26 Fathers are involved in bed-sharing, and yet we know little about the dyadic decision-making process that takes place between couples about infant sleep. 25 Although overnight infant caregiving is conducted mostly by mothers, fathers are often involved in putting infants to sleep and soothing them after nighttime wakening.27,28 Furthermore, in an Australian study, mothers reported frequent negotiation of bed-sharing arrangements with the fathers. 27 Although parents report their primary reasons not to bed-share were desire for privacy and personal space,29,30 a primary reason to bed-share involves wanting to share nighttime caregiving between the mother and father. 24 This limited research on paternal involvement suggests the importance of fathers in bed-sharing decisions and highlights the need for researchers to explore potential differences in bed-sharing prevention messages.
Present Study
The current study investigated mothers’ and fathers’ bed-sharing practices and prevention message sources, parent perceptions of source credibility, and the reported effectiveness of these prevention messages to determine the best prevention message sources. It was hypothesized that bed-sharing prevention messages would most often come from health care professionals, various media sources, family, and friends and that health care professionals and family would be rated as the most credible and most effective sources of information about bed-sharing prevention.
Method
Participants
US community mothers (72%) and fathers (28%) of at least one school-aged child (6-12 years old) from 27 states were recruited (N = 678). Participants’ age ranged from 21 to 58 years (mean [M] = 37.4, standard deviation [SD] = 7.0), and education ranged from 6 to 20 years (M = 15.4, SD = 2.3). Seventy-five percent of participants were married, 14% were single (never married), and 10% were divorced. The sample was ethnically homogenous with 84% identifying as Caucasian/White; the remainder of the sample identified as Asian (5%), African American/Black (4%), Hispanic (3%), mixed ethnicity (2%), and Native American (1%). The number of children in participants’ families ranged from 1 to 8 (M = 2.3, SD = 1.2). Focus children were 53% female.
Participants were asked to answer survey questions retrospectively about bed-sharing patterns when the child was 0 to 24 months old. A sample older than the age of interest was chosen deliberately. Shalvi and colleagues 31 noted challenges in securing honest responses from participants who are currently engaging in controversial behaviors. Parents often bed-share despite expert advice against it and many report deliberately concealing this information from providers; 22 therefore, this study asked parents of children ages 6 to 12 to reflect back on when their child was 0 to 24 months to minimize the likelihood that parents would falsely report their bed-sharing patterns.
Procedures
This study, as part of a larger online survey, was approved by the local institutional review board. Participants were recruited using a convenience sampling approach in which a student in an upper level undergraduate college course asked potential participants whether they would be willing to complete an online survey through SurveyMonkey.com. All students received course credit for either recruiting at least 8 community parents for this study or, if not, documenting their recruitment efforts. That is, students were not put in the position to have to coerce parents to participate. Criteria for community parents’ participation included being English speaking and having a child between the ages of 6 and 12 in their home. Voluntary consent was secured before data collection on the first page of the survey of the study. No compensation was provided for participation.
Measures
Demographic variables were collected, including participant gender, age, marital status, years of education, race/ethnicity, and number of children. Child age and gender were also collected.
Bed-Sharing Questions
Table 1 shows the survey questions and response options. Questions that allowed multiple responses are specifically indicated. The online survey asked if parents had ever bed-shared, the frequency of participant’s bed-sharing behavior from birth to 24 months old, reasons for bed-sharing, bed-sharing prevention message source, and credibility of each source. Bed-sharing frequency was divided into 3 categories: never (0 times), occasionally (1-25 times), and frequently (over 25 times). Literature documents that accidental bed-sharing can occur when parents are extremely tired. 1 Thus, this study separated those that may have accidentally or occasionally bed-shared (less than ~1×/month) from those that may have bed-shared more intentionally/regularly (more than ~1×/month).
Bed-Sharing Survey Questions.

Statistical Analyses
In addition to descriptive statistics, phi coefficients were used to assess differences between prevention source, message type, gender, and reported history of bed-sharing.
Results
Forty-seven percent of participants reported that they never bed-shared, while 28% bed-shared frequently (over 25 times), and 25% bed-shared occasionally (between 1 and 25 times). Bed-sharing occurred in multiple locations during both daytime naps and routine nighttime sleep. Twenty-eight percent of participants bed-shared at night in bed, 23% during naps on a couch, 22% during naps in bed, and 8% at night on a couch.
The most common reasons for bed-sharing related to ease and comfort (“Infant slept better,” “More convenient,” “To facilitate breastfeeding,” “Infant was sick,” and “Parent slept better”; see Figure 1). “Heard bed-sharing safer for baby,” “Shortage of beds,” and “No crib, bassinet, or pack-n-play” were the least common reasons for bed-sharing. At least for this sample, availability of safer sleep options has little to do with the choice to bed-share.

Percentage of participants who reported each reason for bed-sharing.
Regarding prevention messages, 30% reported no bed-sharing prevention advice, 21% received a prevention message from one source, 26% received a prevention message from 2 or 3 sources, and 23% from 4 or more sources. Those who reported receiving a prevention message also reported each of the prevention message sources they encountered (see Figure 2). The most common source was a physician, followed in frequency by a TV news story, newspaper/magazine, their child’s grandmother, and a friend.
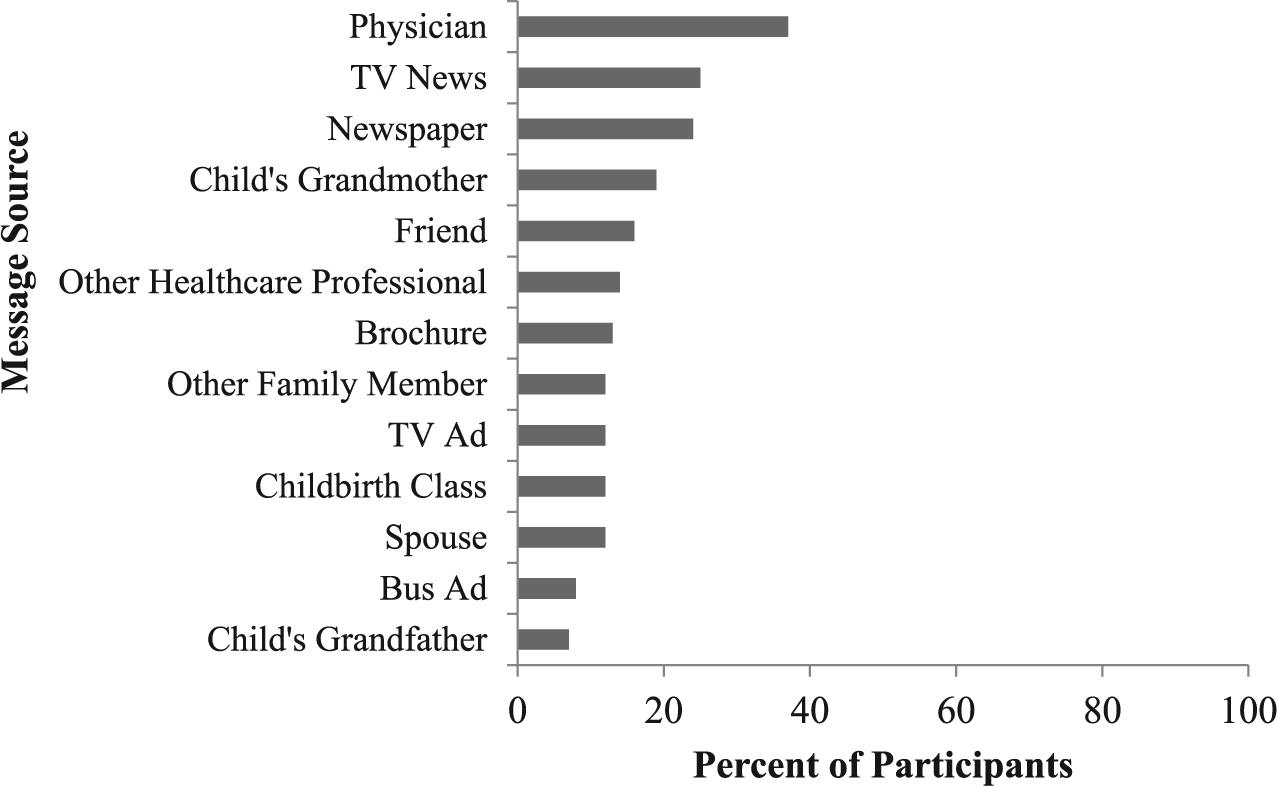
Percentage of participants who reported each bed-sharing prevention source.
Although there were no gender differences in whether a prevention message was received (mothers 71%, fathers 68%, ϕ = .022, ns), there were gender differences in which prevention messaging sources were encountered (see Table 2). Fathers were significantly more likely to receive a prevention message from spouse/coparents or grandfathers. In contrast, mothers were more likely to receive a prevention message from other health care providers, childbirth instructors, brochures, and public advertisements.
Differences in Reported Prevention Source by Gender and Type a .

N = 678.
P < .05. **P < .01. ***P < .001.
Physicians were reported as the most credible source, followed by grandmothers (see Table 3). By group, individual professionals were rated the most credible, followed by individuals with a personal relationship to the parent. Information from professional organizations/media were rated the least credible.
Source Credibility as a Function of Source Type a .
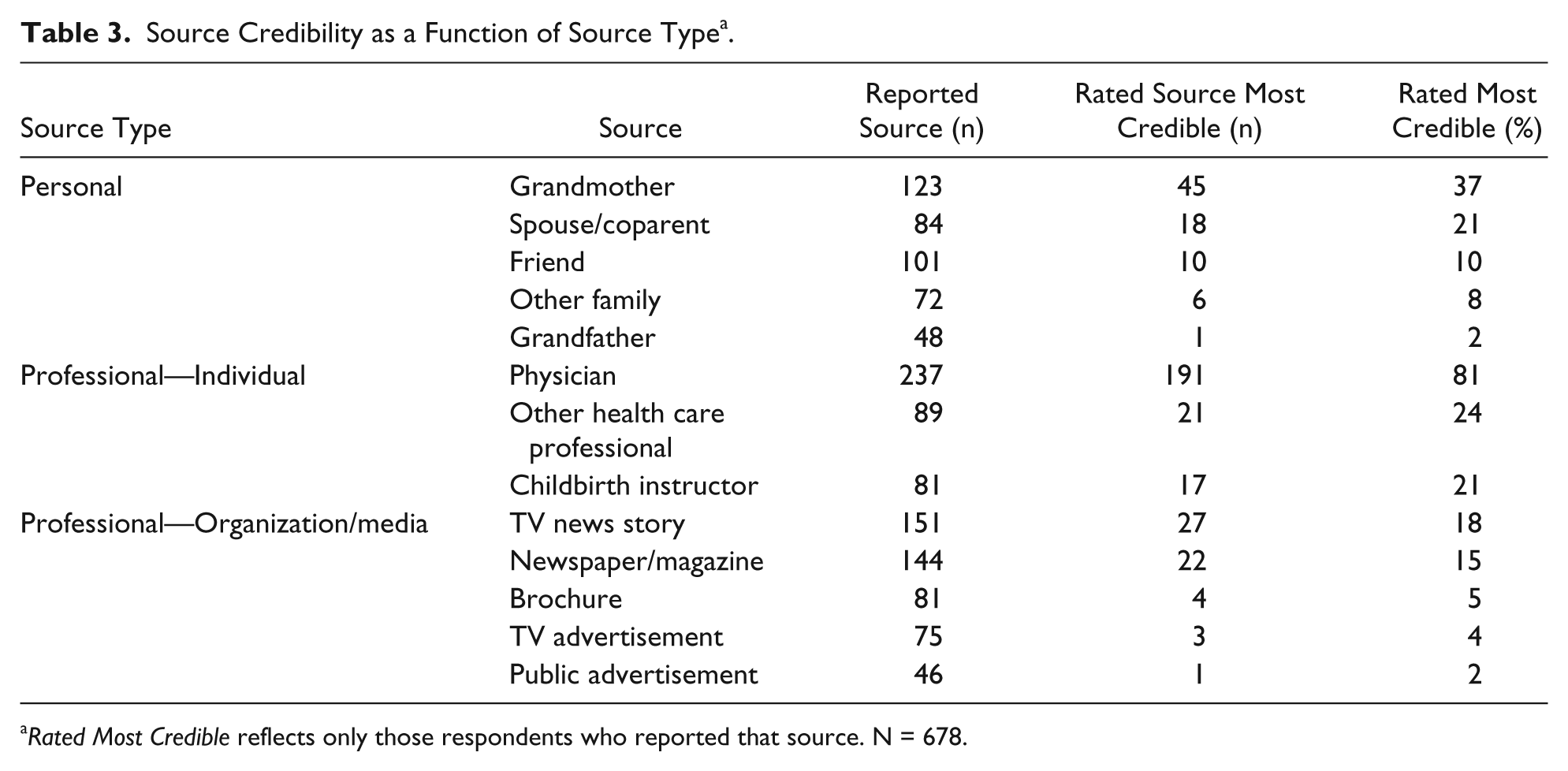
Rated Most Credible reflects only those respondents who reported that source. N = 678.
Participants who received advice against bed-sharing, regardless of source, were not less likely to report bed-sharing (50%) than those who did not receive any advice (55%; ϕ = .043, ns). Source effectiveness of the 5 most common prevention sources was evaluated (see Table 4). Effectiveness of prevention source was defined as there being a significant difference in the prevalence of “ever bed-sharing” between those parents who did and did not receive a prevention message from that source. Grandmothers were the most effective prevention message source, with a 24 percentage point difference between those whose grandmothers discouraged bed-sharing and those who did not. Physicians were also effective prevention sources and more likely to provide the prevention message than grandmothers.
Effectiveness of 5 Most Common Prevention Sources a .

N = 678.
P < .01. ***P < .001.
Discussion
The ongoing incidence of infant death associated with bed-sharing demands a coordinated public health response. Consistent with previous research, 20 bed-sharing continues to be commonplace. One third of participants in the present study bed-shared frequently (more than 25 times) and one fourth bed-shared occasionally (1-25 times). Those that bed-shared frequently often reported doing so during naps on a couch/chair in addition to at night in bed. This is particularly concerning given the increased prevalence of sudden infant death syndrome during couch/chair bed-sharing. 1 Similar to other research32-34 of those who bed-shared, parents reported this decision was primarily because bed-sharing was easier or more comfortable for the parent/infant and did not depend on the accessibility of appropriate sleep environments.
Participants’ exposure to prevention messages varied considerably. Almost one third of participants reported never receiving a bed-sharing prevention message. As hypothesized and similar to previous research, 13 we found bed-sharing prevention messages primarily came from health care professionals, media sources, family (grandmothers), and friends. There were significant gender differences in prevention message source, such that mothers were more likely to hear prevention messages from individual professionals and organizations, while fathers were more likely to hear prevention messages from spouses/coparents and their child’s grandfather. Together with the limited previous research suggesting mothers often negotiate infant sleep arrangements with the fathers, 25 the results from the present study suggest the ongoing need for better understanding of the fathers’ role in bed-sharing decision-making and effective messaging that specifically targets fathers. Prevention efforts should focus on developing a targeted intervention for fathers to assist them in effectively discussing with their spouses/coparents the risk factors involved in bed-sharing.
The second hypothesis was partially supported. Similar to previous research, source credibility on a whole was much higher for physicians than other health professionals, family, friends, and the media. 14 In the present sample, grandmothers were identified as the most credible family member. 13 Other professionals were rated higher or equal to other types of family members (ie, spouse/coparent or grandfather). Individual health care providers were rated as more credible than health care organizations, and physicians were rated as more credible than friends and various media sources.14,16
In terms of prevention message effectiveness, the results showed that parents were less likely to bed-share when grandmothers and physicians provided the prevention message, although a smaller percentage of grandmothers were reported to deliver a prevention message than physicians. The effectiveness and importance of grandmothers’ advice on safe sleep has been previously researched in African American samples.32,35 Grandmothers are actively involved in creating sleep arrangements for infants and their beliefs about safe sleep positions influence parent adherence to the recommended sleep guidelines. 36 This study extends the understanding of grandmothers’ influence on sleep decisions by showing similar results in a White population as well. Prevention initiatives that harness the impact of grandmothers should be developed similar to Moon and colleagues. 21
Although DiMatteo 19 found that general health-related advice from physicians was typically effective, other research suggests parents may disregard physician advice on bed-sharing specifically.20,25 This study found that physicians were one of the most effective prevention sources, but these results do indicate that, for some individuals, physicians’ prevention messages had no impact on bed-sharing practice (ie, many who were told not to bed-share chose to do so anyway). Therefore, these results suggest continued variability in the effectiveness of physician prevention messages among parents. Parental factors, such as health literacy or ethnicity, may influence the effectiveness of physician prevention messages and should be explored in future work.
Together, these results suggest that a more targeted outreach on bed-sharing prevention is needed. Aligning public policy and prevention efforts with empirical research is crucial. Physicians do appear to be credible and effective prevention sources; however, much more information is needed about the context and content of these communications to better guide prevention efforts. The present study did not differentiate between physicians encountered in different contexts (eg, pre- vs postnatal, length of relationship). It is possible that many prevention messages are being delivered during the immediate postnatal period, when parents are likely overwhelmed and exhausted and less likely to listen. Future work should target education prior to the infant’s birth.
The current study was composed primarily of married, well-educated, White parents. Future research should include behaviors and attitudes for populations most at risk for infant mortality and sleep-related deaths and a more diverse sample. Mistrust of physicians is known to be higher among some minority populations, and response to intervention programs may vary by race and ethnicity.37-39
Due to the sensitivity of this topic area, we chose to conduct the present study retrospectively, to reduce the likelihood of deceptive responses. 31 For example, previous work has suggested the associated stigma of bed-sharing likely results in underreporting of bed-sharing behaviors. 40 However, retrospective data collection may increase reporting errors in the subsequent reporting of these events. Research designs that accurately capture these phenomena in real time, without triggering defensiveness, need to be developed.
The present study did not capture all possible prevention message sources. Public health or social workers, nurses, home visitors, early intervention workers, as well as specific Internet-only sources (eg, parenting blogs, public interest groups) may influence bed-sharing, but were not explicitly included within this study. Future research should consider these prevention sources. Furthermore, we cannot assume that all messaging discourages bed-sharing. Numerous sources actively promote “safe bed-sharing,” which they argue promotes the physical and psychological well-being of infants.1-9,41 Given conflicting bed-sharing messages and the ongoing popularity of bed-sharing, assessing the sources, source credibility, and source effectiveness of bed-sharing messages that emphasize safety rather than prevention would be important future work. This research may suggest ways to provide important safety information on bed-sharing to reduce overall risks to parents who are committed to bed-sharing.
Conclusion
Despite bed-sharing prevention campaigns, the practice of bed-sharing is still common. Much of the effort and spending in this area has utilized messaging sources that are known to be of limited value in changing parents’ behavior. These preliminary results strongly suggest that public policy and professional training should make use of an empirical approach to determine the elements of effective prevention efforts to reduce deaths associated with bed-sharing.
Practice Implications
Overall, both physicians and grandmothers emerged as credible and effective bed-sharing prevention message sources. However, not all grandmothers advise bed-sharing prevention. Furthermore, partners/spouses were common prevention message sources for fathers. According to parent report on physician advice against bed-sharing, there continues to be substantial room for improvement in messaging on this topic. Educational interventions should also involve grandmothers and spouses. Such interventions should target the specific and ongoing areas of concern that were uncovered in this study. Parents continue to bed-share on couches/chairs, almost as often as in beds. Sleep quality and the facilitation of breastfeeding continue to be common reasons for bed-sharing. Ways to improve sleep quality and the maintenance of breastfeeding without bed-sharing on any surface should be emphasized in parent/caregiver education on infant sleep.
Author Contributions
JEA: Contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CJN: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JJD: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy.
WHD: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted while Jillian E. Austin was funded by the University of Wisconsin System’s Advanced Opportunity Program Fellowship.