
Abstract
Neuro-meningeal tuberculosis is a severe form of tuberculosis affecting the central nervous system. Tuberculous hypophysitis is a granulomatous inflammation of the pituitary gland, a rare but potentially severe pathology in the context of disseminated tuberculosis. In children, this condition presents significant diagnostic challenges. This article reviews the commonly used imaging modalities, typical radiological signs, and their role in the diagnosis and management of pediatric neuro-meningeal tuberculosis and its complications.
Introduction
Pediatric tuberculosis poses a significant global health threat. 1 Tuberculomas are a frequent and severe complication of tuberculosis in developing countries. 2 Intracranial tuberculomas occur in approximately 13% of children with neurotuberculosis. 3 Early diagnosis of tuberculomas is challenging; they are usually undetectable until they have grown large enough to cause significant neurological symptoms. Often, they are diagnosed late. Tuberculous hypophysitis is one of the rarest manifestations.4,5 Distinguishing tuberculous hypophysitis from other causes of hypophysitis, such as lymphocytic hypophysitis, sarcoidosis, and pituitary adenomas, is often challenging.
Case Report
We present the case of a young girl admitted to the CHP emergency department with a clear meningeal syndrome, including severe headaches, projectile vomiting, and neck stiffness. A lumbar puncture revealed cloudy CSF with 805 cells/µL (normal: <5 cells/µL), predominantly lymphocytes (85% lymphocytes, 15% other cell types), Elevated CSF protein with low glucose, Ziehl-Neelsen test: Presence of acid-fast bacilli (AFB) the culture revealed Mycobacterium tuberculosis after 4 weeks (Figure 1). The patient was started on anti-tuberculosis treatment. After 4 months, she presented with decreased visual acuity and neurological deterioration, including weakness and hypothyroidism, necessitating urgent consultation at the Children’s Hospital of Rabat. A CT scan revealed nodular leptomeningeal thickening with several tuberculomas clustered predominantly in the cavernous sinus and basal cisterns (Figure 2).
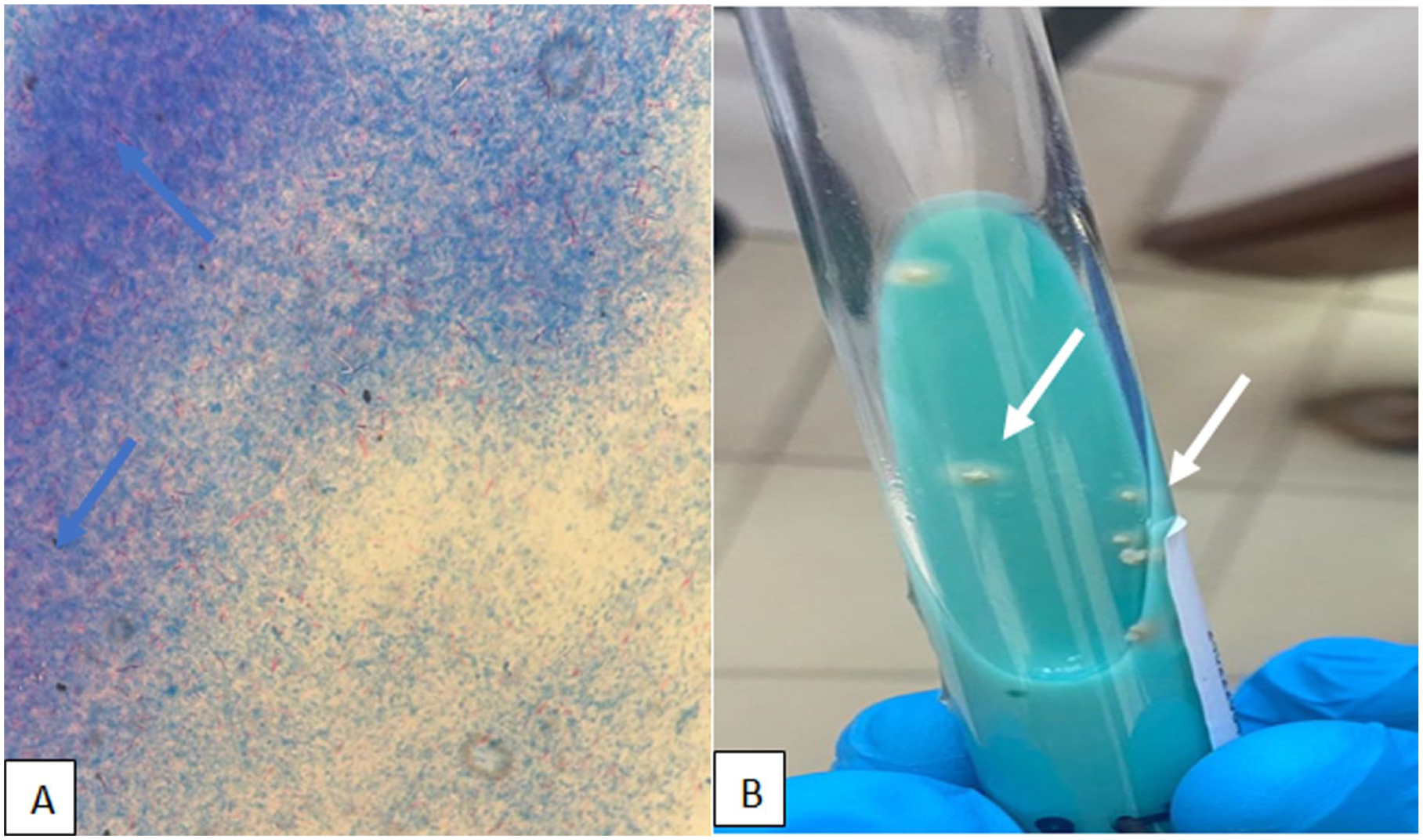
Ziehl-Neelsen test. (A) Presence of acid-fast bacilli (AFB; Indicated by pink structures against a blue background) blue arrow, the culture revealed Mycobacterium tuberculosis after 4 weeks. (B) Appearance of whitish colonies on a Lowenstein-Jensesn (white arrow).

Contrast-enhanced CT axial slice (A), coronal and sagittal reconstructions (B and C) showing leptomeningeal thickening and enhancement at the level of the basal cisterns (white arrow) with multiple tuberculomas (blue arrow).
Brain MRI showed moderate communicating hydrocephalus with marked leptomeningeal enhancement predominating at the basal cisterns, particularly the interpeduncular and suprasellar cisterns. The meningeal thickening measured 3 mm in the most affected areas. Additionally, multiple intra-axial nodular lesions were noted, ranging from 6 to 12 mm in diameter, with peripheral ring enhancement and central hypointensity on T1-weighted images, consistent with tuberculomas.
The pituitary gland appeared enlarged, with a convex superior border and homogeneous enhancement after contrast administration, measuring 10 mm in height. consistent with hypophysitis, and enhancement of the pituitary stalk and adjacent meninges, as well as multiple tuberculomas, Patchy signal abnormalities in the right insulo-temporal subcortical white matter, iso-signal on T1, hyper-signal on T2, and FLAIR, with no enhancement post-contrast and no diffusion restriction, consistent with encephalitis (Figure 3).

Brain MRI, axial (A) and sagittal (B and C) T1-weighted images with gadolinium, showing nodular leptomeningeal, and pachymeningeal thickening and enhancement arranged in clusters, both supratentorial and infratentorial. Sagittal T1-weighted MRI with gadolinium (white arrow) reveals heterogeneous enhancement and hypertrophy of the pituitary gland, with thickening and enhancement of the pituitary stalk and adjacent meninges (blue arrow), along with multiple tuberculomas. Axial FLAIR sequence shows nodular signal abnormalities in the subcortical and periventricular regions, appearing hyperintense on FLAIR (green arrow), non-enhancing after contrast injection, and without diffusion restriction, consistent with encephalitis.
Discussion
Several medical and social factors contribute to the delayed management of neuro-meningeal tuberculosis in our setting. The insidious and atypical onset of tuberculous meningitis, lack of health education, and multiple obstacles patients face in seeking medical care often lead to diagnosis at an advanced stage. Neuro-meningeal tuberculosis typically occurs in children, with peak incidence between 2 and 6 years of age, and in young adults.
6
It can lead to severe complications such as encephalitis, tuberculomas, and, more rarely, hypophysitis. Tuberculous hypophysitis is a granulomatous inflammation of the pituitary gland, usually resulting from hematogenous dissemination of tuberculous bacilli to the pituitary region. It can be associated with tuberculous meningitis or intraparenchymal tuberculomas. Granulomatous inflammatory involvement of the pituitary stalk, gland, and optic chiasm is common in this presentation. Symptoms of neuro-meningeal tuberculosis include fever, general malaise, and classic meningitis signs (headache, projectile vomiting, neck stiffness), along with symptoms suggestive of pituitary involvement, such as fatigue, hormonal disturbances (hypothyroidism, corticotropin deficiency), headaches, and visual disturbances. Diabetes insipidus may occur due to neurohypophyseal involvement.
3
Paraclinical investigations vary in specificity. Cerebrospinal fluid is typically clear, with lymphocytic pleocytosis,
Brain imaging plays a crucial role in diagnosing tuberculosis and tuberculous hypophysitis. Although no imaging signs are pathognomonic for tuberculosis, imaging helps identify sometimes asymptomatic lesions and complications and monitor their progression. CT scanning is the first-line examination due to its availability and ease of use in emergencies. In neuro-meningeal tuberculosis, CT can assess hydrocephalus, meningitis patterns, and tuberculomas. However, MRI is the preferred examination for detailed evaluation of brain parenchyma and meninges. It is particularly useful for identifying tuberculomas, meningeal enhancement, and cerebral infarctions associated with tuberculous vasculitis. 7 MRI is also key in diagnosing tuberculous hypophysitis, a rare but serious condition suspected in patients with neuro-meningeal tuberculosis who present with endocrine symptoms like diabetes insipidus, weakness, and hypothyroidism, as in our patient, along with neurological signs such as visual impairment, also present in our case.
Radiological signs to look for: Hydrocephalus can indicate the disease and precede basal leptomeningitis by several weeks. It may also occur during treatment, requiring regular CT surveillance or be seen in worsening hydrocephalus, as in our patient. Nodular leptomeningeal thickening and enhancement, most often located in the basal cisterns and sylvian fissure, may occasionally involve the cerebellar sulci. 4 After contrast agent (CA) or gadolinium injection, there is homogeneous enhancement of the basal meninges, often extending to the surrounding subarachnoid spaces, sylvian valleys, periprotuberant, and chiasmatic regions. This sign was present in our patient. The appearance of tuberculomas varies according to their evolutionary stage. They appear as hypo-signal on T1 and hyper-signal on T2 with homogeneous contrast enhancement. 8 Intraparenchymal tuberculomas were present in our patient, forming a grape-like pattern. Hypophysitis may also occur, as in our patient. Pituitary gland hypertrophy can be observed, often diffuse, with homogeneous or heterogeneous enhancement. After gadolinium injection, the pituitary gland and surrounding tissues may show heterogeneous enhancement. 4 Tuberculous encephalitis is a frequent complication of tuberculous meningitis .On MRI, it appears as a hyperintense area on T2 and FLAIR sequences, with gyriform enhancement of the peripheral brain parenchyma following contrast administration. 9
Tuberculous meningitis may also complicate into arteritis of the basal vessels, leading to ischemic or hemorrhagic strokes. 8 Infarction results either from thrombosis or artery spasms as they pass through the inflammatory exudate. 10 The infarct zone mainly involves the basal ganglia, internal capsule, and brainstem, and these lesions are detected earlier by MRI than by CT. 9 This sign was absent in our patient. Tuberculous abscesses are a frequent complication of neuro-tuberculosis. They almost always present as large, hypo-dense, solitary lesions, surrounded by a thin rim of contrast enhancement. They are indistinguishable from pyogenic abscesses, certain primary or metastatic tumors, or even resolving hematomas. On MRI, they appear as hypo-signal on T1 and hyper-signal on T2 in the central zone, with crown-like contrast enhancement, similar to pyogenic abscesses. 8 The imaging findings of tuberculous hypophysitis can be challenging to distinguish from other sellar pathologies. Pituitary adenomas, although common, generally exhibit a more well-defined mass effect, heterogeneous enhancement, and rarely involve the infundibulum or adjacent meninges. In contrast, lymphocytic hypophysitis can mimic tuberculous involvement with gland enlargement and stalk thickening, but it typically occurs in the postpartum period and lacks associated basal meningitis or tuberculomas. Similarly, sarcoidosis may involve the hypothalamo-pituitary axis but often presents with systemic findings and granulomatous lesions elsewhere. The presence of coexisting tuberculomas, hydrocephalus, and basal leptomeningeal enhancement provides strong clues favoring tuberculous etiology. This comparison underlines the importance of a comprehensive radiological and clinical approach to differentiate these entities.
Conclusion
Imaging plays a crucial role in diagnosing and managing neuro-meningeal tuberculosis, particularly in identifying complications such as hypophysitis, as seen in our patient. A thorough understanding of imaging modalities and specific radiological signs is essential for effective management.
Footnotes
Acknowledgements
The authors thank Professor SIHAM EL HADAD insight vis-à-vis the case.
Ethical Considerations
No ethical approval is required for de-identified single case reports based on our institutional policies.
Consent to Participate
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Author Contributions
AG: Contributed to acquisition. NB: Contributed to acquisition. SB: Drafted the manuscript. NA: Gave final approval. LC: Gave final approval. SHE: Agree to be accountable for all aspects of work ensuring and accuracy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.