
Abstract
Background. Tuberculosis (TB) remains a major cause of mortality and morbidity globally. Pediatric patients are more likely to develop severe disease. Abdominal TB is a rare manifestation of pediatric TB and can present with chronic and nonspecific abdominal symptoms. This study examines the clinical profile of pediatric patients with abdominal TB and treatment outcomes. Method. A retrospective study of patients admitted to a tertiary pediatric hospital in Singapore over 10 years. Clinical characteristics and outcomes were examined. Results. There were 3 male and 3 female patients with mean age of 11.3 years. Household contacts were traced in 3 cases. The most common presenting symptoms were fever, weight loss, and abdominal symptoms such as diarrhea, vomiting, and loss of appetite. Inflammatory markers were raised with mean C-reactive protein (CRP) and erythrocyte sedimentation (ESR) rate at 70.9 mg/L and 90 mm/h respectively. Abdominal imaging showed abnormalities such as splenic foci and thickened bowel wall with significant intraabdominal lymphadenopathy. Mycobacterium tuberculosis was isolated from stool, rectal swabs and intra-adominal specimens. Two patients underwent excisional biopsy of lymph node to obtain diagnosis. Two patients required emergency laparotomy and 1 patient received esophagogastroduodenoscopy and colonoscopy. Four out of the 6 patients had pulmonary involvement. Conclusion. Abdominal TB should be a differential diagnosis in children with chronic abdominal symptoms for at least 8 weeks with anemia, raised ESR and CRP. The gold standard for diagnosis still remains as positive microbiological culture. However, abdominal imaging studies are also vital in obtaining further supportive evidence for chronic infection.
Keywords
Introduction
Tuberculosis (TB) is a mycobacterial disease that is a major cause of morbidity and mortality worldwide. Since the introduction of the Singapore Tuberculosis Elimination Program in 1997, the incidence of TB declined from 57 per 100 000 residents in 1990s to a low of 35 per 100 000 residents in 2007. In 2016, the incidence of TB was 38.7 per 100 000 residents in Singapore and children aged younger than 19 years accounted for 2.1% of patients diagnosed with TB.1,2 The majority of cases (84%) had pulmonary disease with or without extrapulmonary involvement. The remaining 16% had extrapulmonary TB exclusively.
Diagnosis of TB is challenging, and is even more so in pediatric patients as TB can present in a myriad of symptoms and severity. Abdominal TB is a rare manifestation of pediatric TB infection. Children who are affected have been reported to present with chronic and nonspecific abdominal symptoms with constitutional symptoms. Hence, a high index of suspicion is required for early diagnosis in order to institute appropriate treatment.
This study aims to examine the clinical profile and treatment outcomes of pediatric patients with abdominal TB.
Methods
KK Women’s and Children’s Hospital is the largest tertiary pediatric hospital in Singapore and it accounts for 56.8% of pediatric admissions (excluding neonates) nationally (Ministry of Health Singapore). A patient list with the code tuberculosis was generated using the International Classification of Disease (ICD, Ninth revision, Clinical Modification, or ICD 10th Revision, Australian Modification, from 2012 onwards). Medical records from January 2008 to September 2017 of children aged <16 years with TB and were treated at KK Women’s and Children’s Hospital were retrospectively studied. Data including demographic characteristics, presenting symptoms, investigations, and treatment and clinical outcomes were collected from case notes, electronic records, and the infectious disease database.
The diagnosis of TB was made based on positive culture results, acid-fast staining, histopathology, polymerase chain reaction (PCR), tuberculin skin tests, and interferon-γ release assay (IGRA) in the presence of a clinical diagnosis of TB or suggestive chest X-ray (CXR).
In our center, the T-SPOT.TB assay (Oxford Immuno-tec, Abingdon, UK) is the preferred type of IGRA used for children aged >2 years because of lower rate of indeterminate results compared with QuantiFERON-TB Gold (Cellestis, Victoria, Australia). 2 All patients had CXR performed and were reported by in-house radiologists. All patients also had microbiological investigations done. Relevant fluid or biopsy specimens were sent for acid-fast bacilli (AFB) smear and culture, using the automated MGIT960 system for liquid growth and Lowenstein-Jensen slants for solid growth.
Ethical Approval and Informed Consent
This retrospective study was approved by the SingHealth Centralised Institutional Review Board (CIRB Reference Number: 2015/2024), with waver of informed consent. Informed consent was waived as this was a retrospective study evaluating medical records (specifically at presenting complaints, diagnostic investigations, and complications of treatment and disease). No patient identifier was collected.
Results
The findings of our case series are summarized in Table 1. Of the 6 patients studied, half were male. The mean age was 11.3 years, and 2 were younger than 10 years at presentation. Household contacts could be traced in 3 of the patients. Five out of the 6 patients received Bacillus Calmette-Guérin vaccination at birth. We were unable to confirm history of ingestion of unpasteurized milk in 1 out of the 6 patients. One case was also noted to be retroviral positive. Screening inflammatory markers were raised with mean C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) at 70.9 mg/L and 90 mm/h, respectively.
Summary of Patients’ Details, Clinical Presentation, Investigations, Treatment, and Outcomes of Patients in the Study.
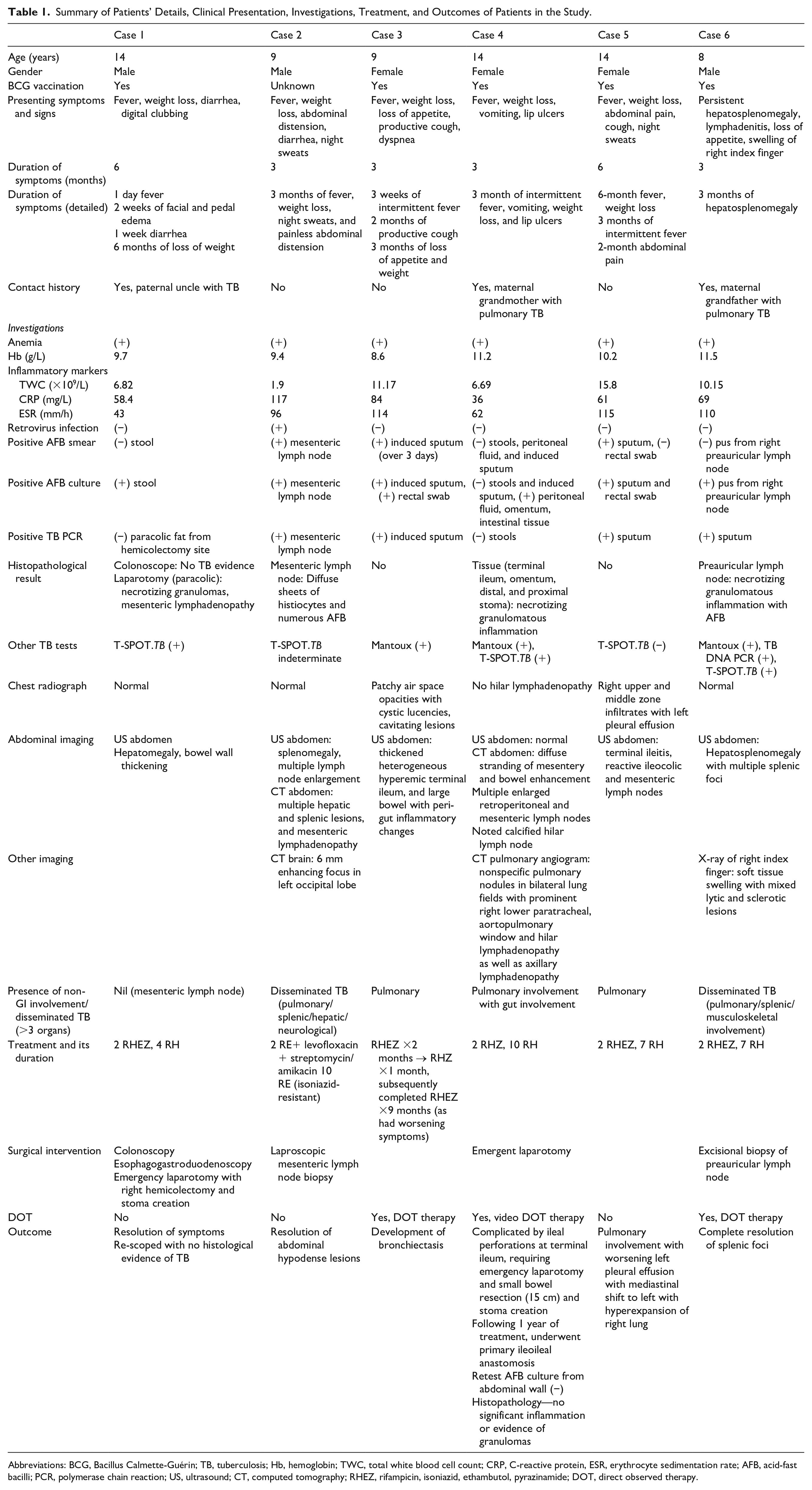
Abbreviations: BCG, Bacillus Calmette-Guérin; TB, tuberculosis; Hb, hemoglobin; TWC, total white blood cell count; CRP, C-reactive protein, ESR, erythrocyte sedimentation rate; AFB, acid-fast bacilli; PCR, polymerase chain reaction; US, ultrasound; CT, computed tomography; RHEZ, rifampicin, isoniazid, ethambutol, pyrazinamide; DOT, direct observed therapy.
Clinical Presentations
The most common presentation included fever, weight loss, and abdominal symptoms such as diarrhea, vomiting, and loss of appetite. Abdominal distension was observed in 1 case. The mean duration of symptoms prior to presentation was between 3 and 6 months. In the sixth case, the child was on outpatient follow-up for persistent hepatosplenomegaly with intermittent fevers following an infection with clinical features of infectious mononucleosis (Epstein-Barr virus serology was tested negative). It was in the third month of outpatient follow-up that he developed preauricular lymphadenitis with right index finger dactylitis, which necessitated hospital admission for further workup.
The initial differential diagnoses in 3 of the cases included protein-losing enteropathy secondary to inflammatory bowel disease (IBD), infective gastroenteritis, and hematological malignancy.
None of the patients had a history of TB. One patient had isolated abdominal involvement. The remaining all had pulmonary involvement, of which one of them also had neurological and another had musculoskeletal involvement.
Two out of the 6 cases required emergency surgical intervention, of which one even required a right hemicolectomy with stoma creation.
Laboratory Findings
All cases presented with anemia (mean hemoglobin level = 10.1 g/dL) and raised inflammatory markers (mean CRP = 70.9 mg/L and ESR = 90 mm/h). Five out of the 6 cases were found to have normal total white blood cell counts on admission.
T-SPOT.TB was performed in 5 out of the 6 cases of which 3 were positive, 1 was indeterminate, and 1 was negative.
Microbiological confirmation was performed in all cases. AFB smear was positive in 50% of the cases and AFB culture was positive in all cases.
Of those with TB-PCR performed, 4 out of the 6 cases showed positive results.
In the 2 cases that underwent laparotomy, histopathology reports of tissue samples from paracolic tissues, terminal ileum, and omentum showed necrotizing granulomas, which were suggestive for TB infection. In the other 2 patients who underwent biopsy of lymph nodes, histopathology reported presence of numerous AFB.
Radiological Findings
In our case series, 2 out of the 6 cases had respiratory complaints. CXR was performed for all cases; however, only 2 were reported to have abnormalities, 1 of them was reported to have cystic lucencies with cavitating lesions, which was highly suggestive of pulmonary TB infection (Figure 1). In the fourth case, the first CXR was reported normal. A CT of pulmonary angiogram was performed later during the inpatient admission revealed multiple nonspecific pulmonary nodules in bilateral lung fields with prominent lymph nodes in the hilar, aortopulmonary, and axillary areas (Figure 2).

Initial chest X-ray of Case #3: 9-year-old girl with 2-month productive cough associated with worsening dyspnea, 3 weeks of intermittent fever, 3-month history of weight loss, showing bilateral patchy air space opacities, cystic lucencies in right perihilar region and infrahilar region. Cystic lucencies also seen in left mid-zone in peripheral areas.

Computed tomography scan of chest showing multiple small pulmonary nodules in right upper lobes.
Abdominal ultrasound imaging was performed in all cases; however, only 1 out of the 6 cases was reported normal. The rest reported hepatomegaly, splenomegaly, and bowel wall thickening suggestive of inflammation with presence of lymphadenopathy.
In 2 cases, CT abdomen was performed that showed mesenteric, retroperitoneal lymphadenopathy, hepatic and splenic lesions, diffuse stranding of mesentery and bowel enhancement (Figure 3).

Images of computed tomography scan of abdomen showing splenomegaly with multiple enlarged lymph nodes with multiple hypodense cystic lesions in the spleen and liver.
In the second case, CT brain and sinuses were performed to investigate the cause of a new febrile episode, which was associated with new onset of tenderness over the left maxillary sinuses. This occurred after treatment for abdominal TB and sepsis had been optimized to meropenem, amikacin, levofloxacin, rifampicin, and ethambutol (as AFB culture results showed resistance to isoniazid). The CT brain showed a 6-mm enhancing focus associated with mild perilesional edema in the left occipital lobes (Figure 4). Cerebrospinal fluid samples taken via lumbar puncture were not suggestive for meningitis and were also negative in the TB-PCR.

Computed tomography scan of brain (of Case #2) showing 6-mm enhancing focus associated with mild perilesional edema in left occipital lobes.
In the sixth case, X-ray of the right index finger showed soft tissue swelling with mixed lytic and sclerotic lesions and this was suggestive of mycobacterial infection (Figure 5).

X-ray imaging of (Case #6) right hand of 8-year-old with TB dactylitis of the right index finger, showing mixed lytic and sclerotic lesions over the proximal phalanx of the index finger.
Treatment and Outcome
All cases received quadruple anti-TB therapy comprising rifampicin, isoniazid, pyrazinamide, and ethambutol for 2 months and then maintained on double anti-TB therapy for at least 4 to10 months. In the second case, the child received levofloxacin and streptomycin and amikacin as the culture showed resistance to isoniazid. Out of the 6 cases, 3 cases received treatment via direct observed therapy (DOT), of which 2 had to attend polyclinic to receive the medications and 1 had DOT via videoconference with the infectious disease specialty nurse throughout the treatment course.
At the end of treatment, the 2 cases that required surgical intervention had complete resolution of intraabdominal TB. This was evidenced by the absence of histological changes of inflammation and granulomas. In 2 other cases, repeat imaging was done that showed resolution of the intraabdominal lesions and splenic foci. However, in the remaining 2 cases with pulmonary involvement, although they both remain asymptomatic from abdominal complaints, they developed further pulmonary complications such as bronchiectasis and worsening pleural effusion with mediastinal shift.
The sixth case fully recovered from disseminated TB infection, but he passed away 2 years later from severe refractory hemophagocytic lymphohistiocytosis with multi-organ failure, which is unlikely to be related to the TB infection.
Discussion
Although pulmonary TB is the most common form of disease manifestation, extrapulmonary TB can affect other systems including lymph nodes, intestines, bone, joints, and meninges, and so on. Abdominal TB refers to TB infection of the gastrointestinal tract, peritoneum, lymph nodes, solid viscera such as liver and spleen. 3 It is the sixth most common form of extrapulmonary site of infection after lymphatic, genitourinary, bone and joints, military and meningeal TB. 4
The abdomen is involved in 11% of patients with extrapulmonary TB and the most common site of involvement is the ileocecal region. The most common presenting symptoms are abdominal pain, weight loss, loss of appetite, and fever.4-6 Tuberculous peritonitis is a rare form of extrapulmonary TB and is primarily observed in young adults 7 without other debilitating chronic disease such as diabetes mellitus or chronic renal failure requiring ambulatory dialysis.
In terms of biochemical changes, anemia and raised inflammatory markers (CRP and ESR) are commonly noted in children with abdominal TB, as described in other case series.8,9
In any patient presenting with abdominal pain, weight loss, loss of appetite, and fever, apart from IBD and malignancy, abdominal TB should also be strongly considered. It has been well documented in literature that differentiating between intestinal TB and IBD is challenging. In a study by Larsson et al, it was found that weight loss was reported more frequently in children with intestinal TB. 9 This was also demonstrated in 5 out of the 6 cases in our case series. Ultrasonography of patients with TB showed hypodense lymph nodes with peripheral enhancement in mesentery and retroperitoneum. Endoscopic findings of transversely placed ulcers, increased nodularity of mucosa, and hypertrophic lesions with mural thickening are more suggestive for intestinal TB. In addition, abnormal endoscopic findings are typically localized to the site of tuberculous infection, which is typically in the terminal ileum or caecum. In Crohn’s disease, children tend to present with right iliac fossa pain. Endoscopic findings included crypt abscesses, focally enhanced colitis, skip lesions, and extensive lesions involving 3 or more intestinal segments.3,9
To distinguish ileocecal TB from Crohn’s disease would ideally require the microbiological and culture confirmation of Mycobacterium tuberculosis. However, diagnosis of TB in children is challenging. With recent advancements, IGRAs have emerged as possible alternatives to the traditional tuberculin skin (Mantoux) test. IGRAs that are commonly used are the QuantiFERON-TB Gold test and the T-SPOT.TB. They have been shown to have high sensitivity and specificity in adults, but their specificity and sensitivity for use in children have not yet been well described. Connell et al performed a 3-way comparison of the Mantoux test and IGRAs in children, 10 which showed significant difference in results of the Mantoux test and both IGRAs (most often Mantoux positive with negative IGRA results). 11 Hence, in patients who have symptoms that are compatible with a possible TB infection and have any IGRAs or Mantoux test positive, empirical TB treatment is recommended until there is microbiological confirmation. In our study, out of the 5 children who had T-SPOT.TB done, 3 were positive, 1 was negative, and 1 was indeterminate. However, in the 3 cases on whom the Mantoux was done, they were all tested positive.
Radiological studies such as ultrasonography, CT scans, barium studies, and magnetic resonance imaging are useful for the diagnosis of abdominal TB. These imaging studies can aid in detecting abdominal lymphadenopathy, ascites, bowel wall and omental thickening, as well as complications such as perforation or stricture formation.3,6,10,12,13
A combination of antituberculous drugs (isoniazid, rifampicin, pyrazinamide, and ethambutol) given either in a 6- or 9-month period has been shown to be effective in treating children with abdominal TB. 14 Relapse has been shown to be uncommon using these treatment regimens, and most children have complete cure of the condition at the end of treatment, which is also illustrated in our case series.8,15 DOT is important in ensuring compliance to treatment and achieving clinical resolution, even more so in the pediatric population. This is evident in 3 of the patients in our case series, who achieved complete resolution of illness. In addition, early surgical management of complications of abdominal TB is essential to decrease morbidity and mortality. Our case series also describes the use of DOT via videoconference in one of our cases with good clinical outcome. This may be a new means of direct observed therapy, which can be explored in future patients. A multicenter, randomized controlled superiority trial of video-based approach to DOT was performed by Story et al, 16 which showed encouraging results. Reasons cited were its cost-effectiveness and convenience for patients in not having to make time to visit a health worker every day. 16 In our center, smartphones or video devices with data plans and local bandwidth are generally easily accessible. Hence, DOT via videoconference may be a potential avenue for further research and improvement.
Long-term follow-up is essential for these children, to ensure resolution of symptoms after the completion of therapy, as well as to follow-up on their growth and surveillance for complications such as bronchiectasis for those with pulmonary involvement.
Conclusion
Abdominal TB should be strongly considered in children with abdominal and constitutional symptoms such as prolonged fever, loss of weight with change in bowel habits, with associated biochemical findings of anemia, and raised inflammatory markers. The diagnosis of TB still remains challenging despite the multiple modalities available. The gold standard of diagnosis is still microbiological diagnosis with culture-positive results. Complete resolution of TB infection requires strict compliance to TB treatment. In our study, this is via DOT, of which one case is via video-DOT. In the context where smartphones with adequate data plan and bandwidth is easily available, this is certainly an avenue to look into to improve patient compliance to treatment.
Footnotes
Author Contributions
SAW: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
DLM: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SWL: Contributed to conception; contributed to acquisition; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
KCT: Contributed to conception and design; contributed to analysis and interpretation; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
NWHT: Contributed to conception and design; contributed to analysis and interpretation; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CYC: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.