
Abstract
Objective:
This study aimed to estimates Disability-adjusted life years (DALYs) for pediatric injury patients at a zonal referral hospital.
Methods:
This is a retrospective cohort study using pediatric injury registry data, DALYs for pediatric injured patients was calculated by adding the Years of life lost (YLL) and Years lived with disability (YLD). Discounting rate of 3%, age weighting parameter of 0.04 and Constant 0.1658 were considered during analysis.
Results:
This study included 1000 pediatric injury patients with median age of 7 years, mostly male 639 (63.9%). Road traffic injuries were the leading cause 341 (34.1%), and 65 (6.5%) died, burns caused 27 (41.6%) of deaths. Pediatric injuries resulted in over 4500 DALYs, with road traffic injuries contributing the most (1650 DALYs).
Conclusion:
This study reveals the high burden of pediatric injuries, with males contributing most DALYs. Road traffic injuries significantly contribute to disabilities, highlighting the need for child-focused interventions.
Introduction
Trauma is a leading cause of morbidity and mortality among pediatric and adolescent populations worldwide, with over 90% of childhood injuries occurring in low- and middle-income countries (LMICs). These injuries represent a significant portion of the global injury burden and are a leading cause of early and preventable deaths among children. Despite children representing nearly 16% of the world population, their heightened vulnerability during their active and exploratory early years poses unique risks, as they are unable to independently recognize and prevent potential injury hazards. 1
In Tanzania, pediatric injuries account for a substantial portion of trauma cases, with 25% of all cases reported. 2 Approximately one-third of these incidents result in hospital admissions or referrals to tertiary care centers due to severity and treatment complexity, particularly affecting children aged 0 to 4 years, emphasizing the critical need for targeted interventions in this demographic. 3 Global burden of disease studies highlights pediatric injuries as a major cause of years of life lost (YLL), with falls and road traffic injuries as key contributors. Notably, 94% of injury-related disability-adjusted life years (DALYs) occur in low- and middle-income countries. In Tanzania alone, injuries contribute to approximately 13% of the nation’s total years lived with disability (YLD) (p. 438). 4
Pediatric injuries lead to both immediate health impacts and long-term disability and are measured by DALYs in global health to guide policy and resource allocation. Research on DALYs related to pediatric trauma, especially in low resource settings, is scarce, as most existing studies concentrate on adult populations or specific types of injuries. This study aims to fill that gap by estimating DALYs for pediatric injury patients at zonal referral hospital in Northern zone of the country to better understand the burden of pediatric injuries and inform population-level care and prevention strategies. Data for this study was drawn from a trauma registry collected from November 2020 to June 2024.
Methodology
Setting
The study was carried out at a major zonal referral hospital that serves the Northern Zone and surrounding regions. The hospital is one of the country’s largest referral centers, providing care to an estimated population of 11 million people from both urban and rural areas. 5 The healthcare system in the country is a mix of both public and private services providers. The public healthcare system is organized into 4 levels: dispensaries, health centers, district hospitals and referral hospitals. Dispensaries and health centers provide basic healthcare services, while district and referral hospitals offer more specialized care. Emergency Medicine Department (EMD) sees approximately 1400 to 1700 pediatric injury patients per year. 6 Pediatric trauma registry was established in 2020 and is currently ongoing with prospective enrollment of all patients less than 18 years of age presenting to EMD for treatment due to injury. Data collected includes patient demographics, details of acute presentation, hospital-based care, and outcomes such as in-hospital mortality and morbidity. The registry aims to provide insights into the epidemiology, clinical presentation, and hospital outcomes of pediatric injuries, as well as to identify clinical factors associated with morbidity and mortality. The findings from the first cohort study conducted from November 2020 to October 2021 revealed considerably high mortality and morbidity rates of injured children, highlighting the needs for capacitating the health system to improve outcomes of pediatric injury patients in the study setting. 7
Study Design
This is a retrospective cohort study design utilizing data from a pediatric injury registry spanning from November 2020 to June 2024.
Study Population
Trauma patients less than 18 years old seeking care for any injury that occurred in the month prior to arrival who survived to evaluation in the EMD were included. Children with injuries sustained more than 1 month prior, those presenting for follow-up care, or cases with missing outcome data were excluded from the analysis. A total of 1000 pediatric injury cases met the inclusion criteria during the study period.
Morbidity Instruments
From the registry data, 2 morbidity instruments were used: the Glasgow Outcome Scale – Extended Pediatrics (GOS-E Peds) and the Patient-Specific Functional Scale (PSFS). These tools were administered at 3 time points at discharge, 2 weeks post hospital discharge, and 3 months post hospital discharge.
GOSE-E Peds
The GOS-E Peds is an 8-item instrument designed to measure outcomes in children after traumatic brain injury. It assesses important areas like physical and cognitive functioning, an external evaluation by assessing the patient’s abilities by asking the patients/caregiver a series of questions about the child’s functional level. 8 The score was dichotomized with a score of 1 to 2 representing “good recovery” and a score greater than 2 representing a “poor recovery.” 9 It has also been demonstrated to effectively detect changes in populations without head injuries. 10
Patient Specific Functional Scale
The Patient-Specific Functional Scale (PSFS) is a patient-reported outcome tool that allows patients or their caregivers to identify key daily activities they find important but are currently struggling to perform. These activities are then rated on a scale from 0 to 10, with higher scores reflecting better physical function. 11 The PSFS can be administered verbally, which makes it suitable for individuals with varying literacy levels. 12 At each follow-up, the patient or caregiver reassesses the same set of activities to track progress over time. During the initial evaluation at hospital discharge, participants selected 3 to 5 activities that were meaningful to them and rated their ability to carry them out. These same activities were reassessed during subsequent follow-ups to evaluate functional improvement. Commonly selected activities included walking, running, playing football, attending school, washing clothes, and social play with peers. 13 Unlike the GOS-E Peds, which provides a more structured assessment of recovery, the PSFS focuses on individualized outcomes based on the patient or caregiver’s priorities.
Data Collection
Trained research assistants were responsible for collecting patient data by obtaining information from patients or primary caregivers and reviewing medical records. If patients arrived at the EMD outside of scheduled data collection times, they were enrolled the following day if still hospitalized; however, patients discharged during this time were excluded. During the hospital stay, the research assistants closely followed up and recorded details of the care and discharge process. Following a discharge from the hospital, patients were followed up at 2-week and 3-month intervals to assess changes in physical function using 2 morbidity instruments namely The Patient-Specific Functional Scale (PSFS) and the Pediatric version of the Glasgow Outcome Scale Extended (GOS-E Peds). All data was captured using tablets within the REDCap system, 14 with the Principal Investigator overseeing quality control for all entries. To maintain data completeness and integrity, 2 full-time, trained research assistants followed up patients, assisted in collecting vital signs, and retrieved data from medical records. The research assistants had prior experience in scientific data collection but additionally they underwent 2 weeks of project-specific training. They also participated in weekly calls and meetings for the whole period of data collection with the research team to address any issues related to data collection and quality.
Disability-Adjusted Life-Years
The Disability-Adjusted Life Years (DALYs) represented the total healthy years lost due to injuries. DALYs were calculated by summing the years of life lost (YLLs) and years lived with disability (YLDs) due to injury and provided a comprehensive measure of the impact of both fatal and non-fatal injuries. This was represented by the formula DALYs = YLL + YLD. 15
YLLs quantifies the years lost due to premature death from injuries. YLLs were calculated by identifying the number of deaths attributed to each injury-related cause and multiplying each death by the standard life expectancy remaining at the age of death, as defined by the Global Burden of Disease (GBD) standard life table. The YLLs per death were based on the average life expectancy for both males and females at the mean age of death for each recorded injury mechanism. Meanwhile, YLDs reflect the years spent living with health impairments, estimating the duration of these injuries. YLDs for pediatric injury patients were calculated by considering the treatment status and assigning each injury condition a specific duration of disability based on clinical expectations and a standardized disability weight. Pediatric injury YLDs were then calculated as the product of the disease duration and the associated disability weight, with all standardized weights sourced from the Global Burden of Disease Study. 16
In the calculation of Years of Life Lost (YLLs) and Years Lived with Disability (YLDs), an age-weighting rate of 4.0% and a time discount rate of 3.0% per year were applied. The use of time discounting reflects the assumption that a year of healthy life gained in the future is valued slightly less than 1 gained in the present. This approach was commonly used in earlier Global Burden of Disease (GBD) studies and continues to be applied in various public health policy models to allow for comparability across studies. 17 Although recent GBD updates have moved away from using time discounting, we opted to include it for consistency with several prior studies in low- and middle-income countries and to allow comparability with similar local burden estimates. 18
Age-weighting function = Ce–βx (where C = constant equal to 0.16243, β = constant equal to 0.04, x = age, and e = constant equal to 2.71). 19
DALYs were estimated using proxy measures derived from available patient data. Diagnoses recorded in the trauma registry were used to assign condition types, each of which was matched to a corresponding disability weight based on Global Burden of Disease (GBD) estimates. These weights were used to calculate Years Lived with Disability (YLDs), while Years of Life Lost (YLLs) were estimated using standard life expectancy at the age of death. This approach enabled us to approximate the burden of injury in the pediatric population despite the absence of detailed clinical disability data.
Outcome
The outcome data collected were in-hospital mortality and morbidity due to injury.
Secondary Information
Socio-demographic characteristics variables, acute presentation information, hospital-based care, PSFS scale, GOS-E score, GCS Score, mechanism of injury, injuries sustained, management of injuries, pre/post-hospital management, length of hospital stay, and other applicable variables were collected from the registry.
Glasgow Coma Scale (GCS) is widely used to determine the level of impaired consciousness among trauma pediatric patients. The scale has 3 aspects of responsiveness which include motor with a score of 6, verbal responses with a score of 5 and, eye-opening with a score of 4, making a total score of 15. GCS was categorized as mild (for scores of 13-14), moderate (for scores of 9-12), severely impaired level of consciousness (for scores of 3-8) and score of 15 for normal. 20
Data Analysis
The analysis was conducted using STATA version 17 (StataCorp, College Station, TX, USA) and Excel spreadsheet. Descriptive statistics were employed to summarize the data, with categorical variables presented as frequencies and percentages, and numerical variables summarized using measures of central tendency along with their respective measures of dispersion. For the estimation of DALYs, the YLL and YLD were calculated separately, then summed to determine the total DALYs. Subgroup analyses were conducted to estimate DALYs based on factors such as age group, sex, healthy condition by specialty and mechanism of injury. A sensitivity analysis was performed to evaluate how variations in disability weights or life expectancy assumptions influenced the DALYs estimates. In sensitivity analysis discounting rate of 3%, age weighting parameter (beta) of 0.04 and Constant (C) 0.1658 were considered during analysis.
Results
Sociodemographic Characteristics of Study Participants
A total of 1000 pediatric injury patients were included in the study (Table 1), with a median age of 7 years and IQR 4 to 12 years. The majority (n = 347, 34.7%) were aged between 6 and 11 years. Males were more than half of the participants, totaling (n = 639, 63.9%). Additionally, parents of majority of the children 670 (67%) lived together with their child.
Sociodemographic Characteristics of Study Participants (N = 1000).

Median age (IQR): 7 years (4-12 years).
Tribe: Others; haya, kurya, jaluo, jita, makonde, fipa, hehe, mrangi, mnyamwezi, mwarusha, zigua, and nyakyusa.
Clinical Characteristics of Study Participants
Among all injured pediatric patients (Table 2), Road traffic injuries were the leading cause of injury, affecting 341 (34.1%) patients, with pedestrians comprising the majority at 244 (71.6%). Falls were the second most common cause, accounting for 319 (31.9%) cases. As for burn injury, the majority 54 (42.5%) had severe burns covering 20% or more of their body surface area. Most patients 712 (71.2%) had a Glasgow Coma Score of 15 on arrival. A total of 129 (12.9%) patients were hospitalized for over 30 days and out of all patients, 316 (31.6%) had abnormal CT scan findings, with the majority of these 290 (91.8%) cases being abnormalities identified on head CT scans. Sixty-five patients (6.5%) died, with burns accounting for 27 (41.6%) of all deaths. Less than 1% (9 patients) of injured pediatric were referred to a rehabilitation unit.
Mechanism of Injury and Clinical Characteristics of Study Participants (N = 1000).
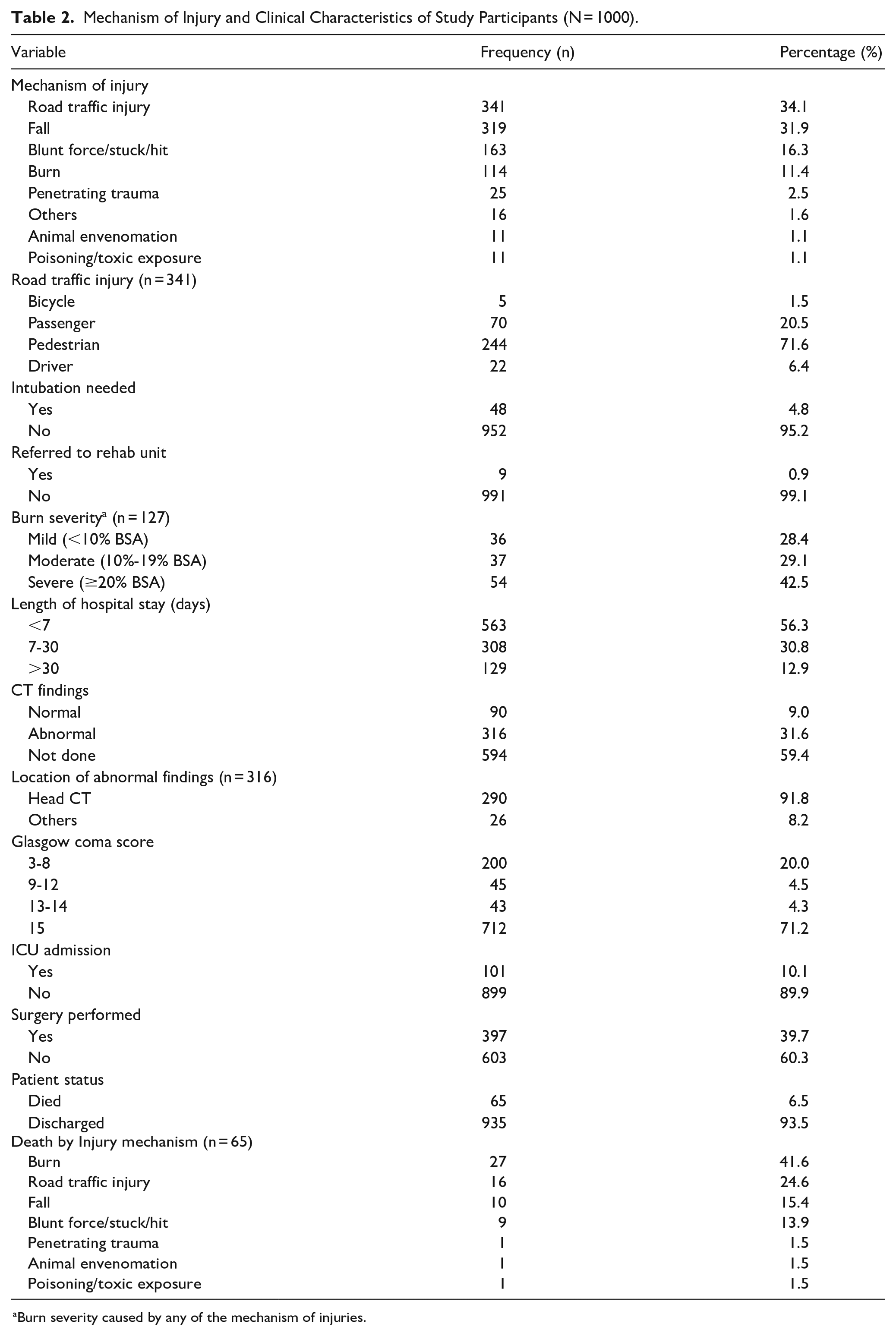
aBurn severity caused by any of the mechanism of injuries.
Estimation of Disability Adjusted Life Years (DALYs)
In the estimation of DALYs (Table 3) among pediatric injury patients, a total of 4508 years of healthy life were lost, comprising 2027 years of life lost due to premature mortality and 2481 years lived with disability due to injury-related impairments, across various surgery conditions. Traumatic brain injury accounted for the highest burden, with approximately 1590 years of healthy life lost, followed by general surgery conditions at 1457 years. The findings indicate that road traffic injuries contributed the highest DALYs among the mechanisms of pediatric injuries in our cohort, totaling 1650 DALYs. The DALYs for pediatric patients who sustained injuries from falls also indicates a considerable health burden, totaling 1386 DALYs. This is composed of 598 years of life lost due to premature mortality and 787 years lived with disability resulting from persistent functional impairments that extend beyond the acute phase of injury recovery. Notably, the YLD contribution is higher than the YLL, highlighting that the majority of the burden is related to ongoing residual impairments rather than mortality.
Total DALYS to Pediatric Injury Patients by Injury Mechanism and Health Conditions (N = 1000).

Abbreviations: DALYs: disability adjusted life years; YLL: years life lost; YLD: years lived with disability.
Estimation of Total DALYs by Gender and Age Groups
When analyzing DALYs by gender (Table 4), male pediatric patients accounted for more than half of the total years of healthy life lost, contributing 2855 years. Traumatic brain injury represented the greatest burden in males, with 1158 years of healthy life lost. In comparison, female patients, contributed 1654 years to the overall DALYs, with traumatic brain injuries again having the highest burden at 1158 years. The highest DALYs were observed among patients aged 6 to 11 years, totaling 1659 years, compared to other age groups (Figure 1). Interestingly, for nearly all age groups, the primary contributor to the total DALYs was the years lived with disability.
Total DALYS by Gender to Pediatric Injury Patients by Health Conditions (N = 1000).
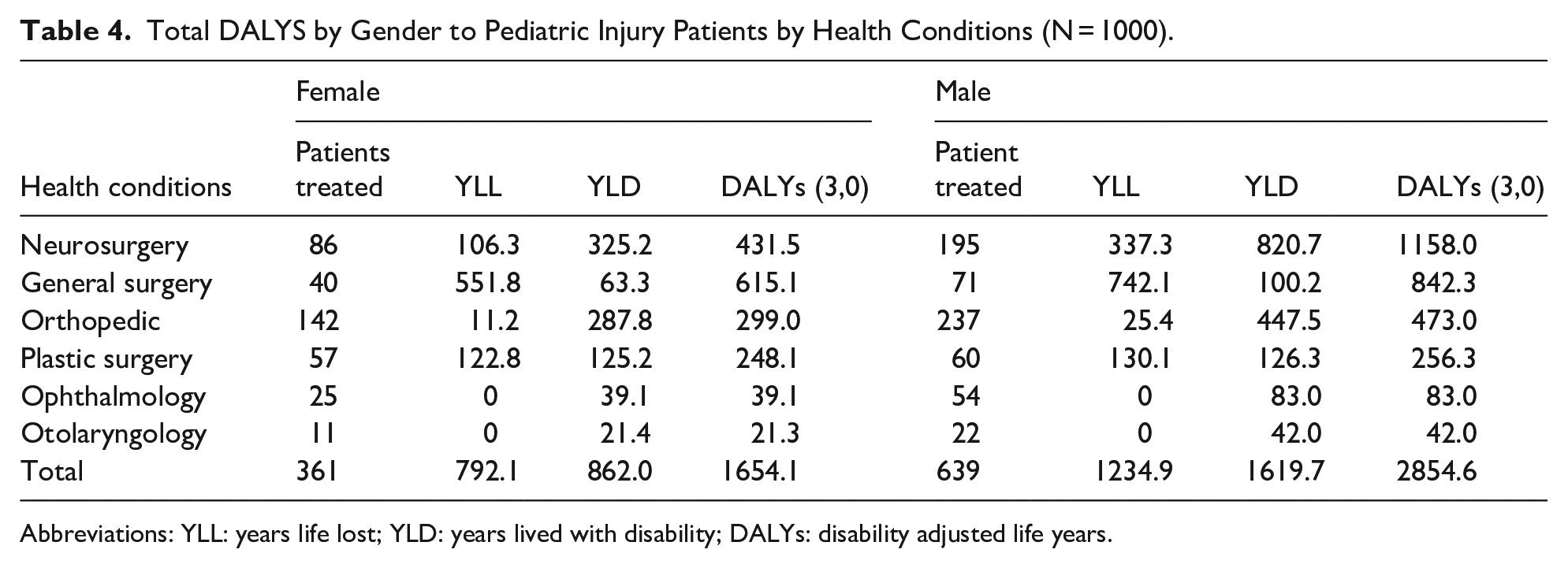
Abbreviations: YLL: years life lost; YLD: years lived with disability; DALYs: disability adjusted life years.

Displays the DALYs to pediatric injury patients at different age groups.
Discussion
The findings of this study highlight the substantial burden of pediatric injuries on the pediatric population, as reflected in the 4500 Disability-Adjusted Life Years (DALYs) lost. These metric underscores not only the premature mortality but also the long-term disability that affects pediatric injury patients. Comparing our findings with DALYs estimates for other diseases reveals that pediatric injuries contribute a greater burden than leukemia in children aged 5 to 14 years. This difference could be attributed to the high incidence of injuries in children, the significant long-term disability they cause, nature of conditions and the limited access to timely and effective rehabilitation services. 21
The DALYs reported in this study exceed the 2970 DALYs associated with delayed surgical access among pediatric patients in Somaliland. 22 This discrepancy may be explained by differences in the types and severity of injuries studied, variations in healthcare systems, or disparities in access to timely and comprehensive rehabilitation services. Additionally, methodological differences in how DALYs were calculated, including the inclusion of distinct disability weights or age distributions, likely contribute to the observed variation.
The findings of this study indicate that road traffic injuries and falls as the leading contributors to injury DALYs, in line with the Global Burden of Injury report, which emphasizes road injuries, self-harm, and falls as significant contributors of injury DALYs, with road injuries significantly driving DALY rates among children worldwide. Moreover, the Global Burden of Injury report attributes a substantial proportion of years lived with disability 46.4% of total DALYs to falls, a pattern similarly reflected in this study. 23
The findings from this study revealed that pediatric patients aged 6 to 11 years contributed the highest proportion of DALYs compared to other age groups. A similar pattern was observed in a study on the burden of childhood asthma, which reported an increase in age-standardized DALYs among children aged 5 to 9 years. 16 This trend may be attributed to the increased activity levels and independence in this age group, making them more susceptible to injuries. Additionally, the physiological and cognitive development during this stage could influence the severity of injuries and their long-term impact on health outcomes.
The fact that male patients contributed the highest DALY burden, accounting for 2855 years, aligns with existing literature that suggests boys are more prone to injuries than girls due to various behavioral and environmental factors. This was also seen at global burden of disease report which shows that in all regions DALYs injury rates are much higher in men than in women. 23
An important observation is that years lived with disability (YLDs) accounted for a substantial portion of the DALYs across all age groups. This indicates that, while mortality is an important outcome, the long-term consequences of non-fatal injuries such as physical impairments and reduced quality of life are major contributors to the overall burden. These findings underscores the importance of both acute trauma care and long-term rehabilitation in mitigating the impact of pediatric injuries. 24 The significant contribution of years lived with disability to the overall DALY burden suggests that the provision of rehabilitation services is essential for reducing the long-term impact of pediatric injuries. Policymakers should prioritize integrating rehabilitation services into pediatric trauma care pathways to address both the immediate and long-term needs of injured children.
Injuries, both fatal and non-fatal, present a substantial health challenge in Sub Saharan Africa (SSA), particularly affecting children. 25 While thousands of injuries in children are non-fatal, they often go underreported, resulting in significant YLD.26,27 Despite its impact on morbidity and mortality, pediatric injuries in SSA are notably absent from global initiatives for child survival, representing the primary cause of death in children beyond the initial 5 years of life. 7 Mortality rates from pediatric injuries in some countries exceed 50%, with over 95% of fatalities occurring in Low middle income countries (LMICs).28,29
In SSA, pediatric injuries emerge as the predominant surgical issue affecting children, constituting the highest percentage of pediatric surgical admissions.30,31 The region experiences the highest number of DALYs lost globally, yet employing only 3% of the global health workforce and allocating less than 1% of the world’s financial resources to health. 32 Tanzania, similar to many other LMICs, faces a scarcity of published data on pediatric injuries, limiting the ability of policymakers to understand the true burden hence prioritization of the problem and designing of targeted interventions. 3
Despite the alarming prevalence of pediatric injuries in sub-Saharan Africa, there is a notable dearth of comprehensive studies on injury morbidity in the region. 25 Existing research in Rwanda highlights significant post-injury disability, emphasizing the need for a clear understanding of long-term impacts. 33
The findings from this study illustrate the profound long-term impact of pediatric injuries on health and functionality. Neurosurgery-related conditions contribute the highest burden underscores the complexity and seriousness of these cases, which demand specialized and often prolonged rehabilitation services. Estimating DALYs for specific conditions helps identify the specialty areas with the highest burden of pediatric injuries, enabling efficient resource allocation and the design of targeted interventions to improve health outcomes. As each specialty condition has unique rehabilitation, prevention, and treatment needs.
Also, the findings from this study underscores the need to integrate early intervention strategies within rehabilitation plans to optimize recovery, prevent secondary complications, and ultimately improve quality of life for affected children. This approach not only addresses the immediate rehabilitation needs but also focuses on the holistic well-being of pediatric injury patients, helping them regain lost functionality and reduce their overall disability burden.
Strengths of the Study
The study provides a detailed assessment of both mortality and morbidity outcomes, offering valuable insights into the burden of pediatric injuries and supporting evidence-based public health policies and resource allocation strategies. With a sample size of 1000 pediatric injury cases, the study has the statistical power to generate reliable estimates and perform detailed subgroup analyses based on factors such as mechanism of injuries, age, and gender. To our knowledge, this is the first study to estimate DALYs to pediatric injury patients in East Africa.
Study Limitations
The findings may not be fully generalizable to other settings with different healthcare systems or injury profiles as it excludes cases managed in lower-level health facilities or those who do not seek care. When calculating DALYs, we assigned proxy conditions based on the WHO Global Burden of Disease (GBD) disability weights data to each patient, using their recorded diagnosis, as actual patient-level disability information was not available. This approach may have led to overestimation or underestimation of DALYs. However, the proxy conditions closely matched the recorded diagnoses, indicating that the DALY estimates were reasonably robust.
Conclusion
This study highlights the significant burden of pediatric injuries in terms of mortality, disability, and lost years of healthy life, with road traffic injuries and falls being the leading contributors. The findings underscore the critical need for enhanced injury prevention strategies, improved trauma care, and better access to rehabilitation services. Addressing these gaps will be essential in reducing the long-term impact of pediatric injuries and improving outcomes for affected children.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251365185 – Supplemental material for Estimation of Disability Adjusted Life Years in Pediatric Injury Patients at a Zonal Referral Hospital in Northern Tanzania
Supplemental material, sj-docx-1-gph-10.1177_30502225251365185 for Estimation of Disability Adjusted Life Years in Pediatric Injury Patients at a Zonal Referral Hospital in Northern Tanzania by Baraka Moshi, Elizabeth M. Keating, Blandina T. Mmbaga, Anthony Saxton, Joao Ricardo Nickenig Vissoci, Winfrida C. Mwita, William Nkenguye, Alice Andongolile, Miriam Puschel, Edwin Joseph Shewiyo, Frijenia G. Sumbai, Happiness D. Kajoka, Kajsa Vlasic, Francis Musa Sakita, Frida Shayo, Catherine A. Staton, Michael J. Mahande, Emily R. Smith and Haleluya Moshi in Sage Open Pediatrics
Footnotes
Acknowledgements
We express our gratitude to all individuals who contributed at any capacity to this project, as well as the team responsible for data collection, without forgetting pediatric injured children and their parents/Caretakers whose data contribute to the KCMC pediatric injury Registry.
List of Abbreviations
DALYs: Disability Adjusted Life years
DW’s: Disability Weights
EMD: Emergency Medicine Department
GOSE: Glasgow Outcome Score Extended
HIC’s: High Income Countries
LMIC’s: Low- and Middle-Income Countries
PSFS: Patients Specific Functional Scale
SSA: Sub Saharan Africa
YLD: Years Lived with Disability
YLL: Years of Life Lost
WHO: World Health Organization
ORCID iDs
Ethical Considerations
Ethical approval for this study was granted by the Kilimanjaro Christian Medical University College Research Ethics and Review Committee (CRERC) in Moshi (KCMC/P. I/Vol.XI/2658). Ethical clearance was also secured from the National Health Research Ethics Committee (NatHREC) under the National Institute for Medical Research (NIMR) in Tanzania (NIMR/HQ/R.8a/Vol. IX/4711). Additionally, permission to carry out the study was obtained from the President’s Office, Regional Administration, and Local Government (PO-RALG), along with approvals from the regional administrative secretary, the regional medical officer, and the KCMC administration.
Consent to Participate
Formal consent was not needed, as this process was part of a standard healthcare quality improvement initiative and the observational registry did not influence patient care. As such, consent was implied in the consent to treatment. To maintain anonymity, no identifiable data were collected, and all information was securely stored in a password-protected database with access limited to a designated group of researchers.
Author Contributions
Conceptualization: BTM, HM, MM, EMK, CAS, BM, ES, WN, JVR. Data acquisition: BM, JVR, WN, FGS, MP, EJS. Data analysis and interpretation: BM, AS, HM, MM, EMK. Report writing review and editing: BTM, HM, MM, EMK, CAS, BM, ES, WN, JVR, WM, AA, FMS, FS, KAV.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Trauma Research Capacity Building Program at KCMC, funded by the D43 TRECK grant #D43-TW012205 (Mmbaga, Staton) from the U.S. National Institutes of Health (NIH) and the Duke Department of Emergency Medicine, supports this work. Moshi, Nkenguye, Miriam, Edwin, Frijenia, Happiness, Alice and Winfrida’s time are funded by the NIH through the TRECK D43 program. Data for this study was sourced from a pediatric trauma registry, with additional support for EMK provided by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant K23 HD112548).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are available from the Kilimanjaro Clinical Research Institute (KCRI) upon reasonable request from the corresponding author (Email:
Patients and Public Involvement
Patients and the public were not involved in the design or development of this study. The findings will be shared through open-access publications and made available through other publicly accessible channels.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.