
Abstract
Background:
Being able to detect, assess, and manage children with primary hypertension is one of the requirements of the Thai pediatric residency training curriculum. The present study aimed to survey the practice of pediatric primary hypertension care by Thai pediatricians.
Materials and Methods:
Participants’ demographic information, educational background, and practice, including diagnosis, investigation, and treatment in children with primary hypertension at an outpatient setting, were all included in the surveys and were distributed to pediatric residents, general pediatricians, and pediatric subspecialists in Thailand using the online survey. The results were defined as appropriate answers if they were aligned with the guidelines recommended by the American Academy of Pediatrics.
Results:
342 (79 males) with a mean age of 37.6 years and a mean duration since residency training of 10.4 years were included. The proportion of participants who answered appropriately was 188 (55%), 190 (55.6%), and 169 (49.4%) in the diagnosis, investigation, and treatment parts, respectively. However, only 43 (12.6%) participants could answer appropriately for all 3 parts. Compared to the inappropriate group, experience in diagnosis was higher in the appropriate group (44.2% vs 28.4%, P-value = 0.036), but the duration since residency training < 5 years and being a nephrologist were not different between the 2 groups (41.9% vs 43.5%, P = .849 and 7 vs 6%, P = .807, respectively).
Conclusions:
Experience in diagnosis, rather than the duration after the residency training or being a nephrologist, had a favorable impact on the appropriate practices of children with primary hypertension among Thai pediatricians.
Introduction
Over the past decade, there has been an increase in the prevalence of hypertension in children and adolescents. 1 The prevalence was reported to range from 5.15% to 13.8%.2 -5 In general, hypertension is categorized into 2 groups based on the etiologies. Secondary hypertension is defined by having the exact cause of hypertension, such as kidney disease, renovascular disease, and endocrinologic disease. If the etiology is not clearly defined, it is categorized as primary hypertension. Being able to detect, assess, and treat children with primary hypertension is a crucial ability for general pediatricians. Not only is it one of the required skills for the pediatric residency curriculum, but the early diagnosis of hypertension in children may also decrease long-term cardiovascular morbidity in adulthood. 6 In 2017, the American Academy of Pediatrics (AAP) launched a clinical practice guideline for screening and management of children with high blood pressure. 1 The guideline provided a new normative table for blood pressure by removing blood pressure data from children with obesity, and also set new criteria for the diagnosis of hypertension. As there is currently no clinical practice guideline for diagnosing and treating pediatric hypertension in Thailand, therefore the 2017 AAP guideline has been widely used among Thai general pediatricians and pediatric nephrologists.
The previous study in the Netherlands found that most pediatricians did not screen for hypertension and did not compare the blood pressure reading with reference standards. 7 In North America, a survey of pediatric nephrologists surprisingly revealed different blood pressure goals used after initiating treatment among specialists. 8 Similar findings in a study in Japan and Korea, there were various practice patterns in children with hypertension among specialists. 9 Therefore, we hypothesize that such practices vary significantly among Thai pediatricians and pediatric residents. The present study aimed to describe the practice pattern of Thai pediatric residents and pediatricians in screening, diagnosing, investigating, and managing children with high blood pressure suspected of primary hypertension in the out-patient setting.
Materials and Methods
The present study was approved by the Ethics Committee for Human Research of the Faculty of Medicine Ramathibodi Hospital (MURA 2023/499). This cross-sectional study enrolled Thai pediatric residents, general pediatricians, and pediatric subspecialists. The surveys were distributed through social media among the Thai pediatrician community and during the annual general meeting of the Royal College of Pediatricians of Thailand.
Questionnaires
The questionnaires were adapted and created by three Thai pediatric nephrologists. Validity testing was performed by calculating the index of item objective congruence (IOC). The IOC of all questions was more than 0.7, which means there was high content validity. Afterward, we used a test-retest method for testing survey reliability by administering the same questionnaire to the same group of 30 respondents at two different time points (2 weeks apart) and calculating the correlation between the two sets of scores. The Pearson correlation result was .638, which was an acceptable reliability. The questionnaires contained 5 parts, including general information, experience, practice in diagnosis, investigation, and treatment, as shown in Table 1. The questionnaire was developed and adapted from the previous studies.7 -9 The appropriate answers were defined when they were aligned with the recommendations from the 2017 clinical practice guidelines for screening and management of high blood pressure in children and adolescents by the American Academy of Pediatrics. 1
Information in the Questionnaire.

Statistical Analysis
All analyses were conducted using SPSS 29.0 (SPSS Inc, Chicago, USA). The normality test was assessed by the Kolmogorov-Smirnov test. Descriptive statistics are presented as mean (SD) for normally distributed continuous variables and median (IQR) for non-normally distributed continuous variables. Differences in continuous variables between the 2 groups were compared using the Student-t test or Wilcoxon rank-sum test, as appropriate. Differences in categorical variables between the two groups were compared using the chi-square or Fisher’s exact test. A P-value ≤ .05 was considered statistically significant.
Results
There were 370 participants who responded to the survey, with 9 individuals not meeting the inclusion criteria as they were not pediatricians, 5 individuals refusing to participate, and 14 individuals providing duplicate responses. Therefore, a total of 342 participants were included in the present study, with the majority being female (263, 76.9%), with a mean age of 37.6 years and a mean duration since residency training of 10.4 years (Table 2). Pediatric sub-specialists (185, 54.1%) responded to the survey, with 21 (6.14%) being nephrologists. Most participants worked in facilities with more than 200 beds, accounting for 70.2%. The participants worked in all regions of Thailand, with the highest number (157, 45.9%) from the capital city (Bangkok). The most used device for measuring blood pressure was the oscillometric device in 93.6% of participants. About 246 (72%) used the 95th percentile as the cut-off for hypertension, 153 participants (56.4%) screened for blood pressure at the age of 3 to 4 years, and only 139 (40.7%) made a diagnosis of hypertension when high blood pressure persisted for 3 visits.
Demographic Data.

Regarding the last 3 parts of the questionnaire, the proportions of participants who answered appropriately were 188 (55%), 190 (55.6%), and 169 (49.4%) in the diagnosis, investigation, and treatment parts, respectively (Supplemental Tables S1-S3). However, only 43 (12.6%) participants answered all 3 parts appropriately. Table 3 shows the data between the 2 groups, comparing those who answered appropriately and those who did not. There were no differences between age, duration since residency training, the proportion of nephrologists, and workplaces between the two groups. However, having experience in diagnosing hypertension showed a significantly higher proportion in the appropriate group than the inappropriate group (44.2% vs 28.4%, P-value = .036).
Data Comparing the Group of Participants Who Answered Appropriately for All 3 Parts and the Group Who Did Not.
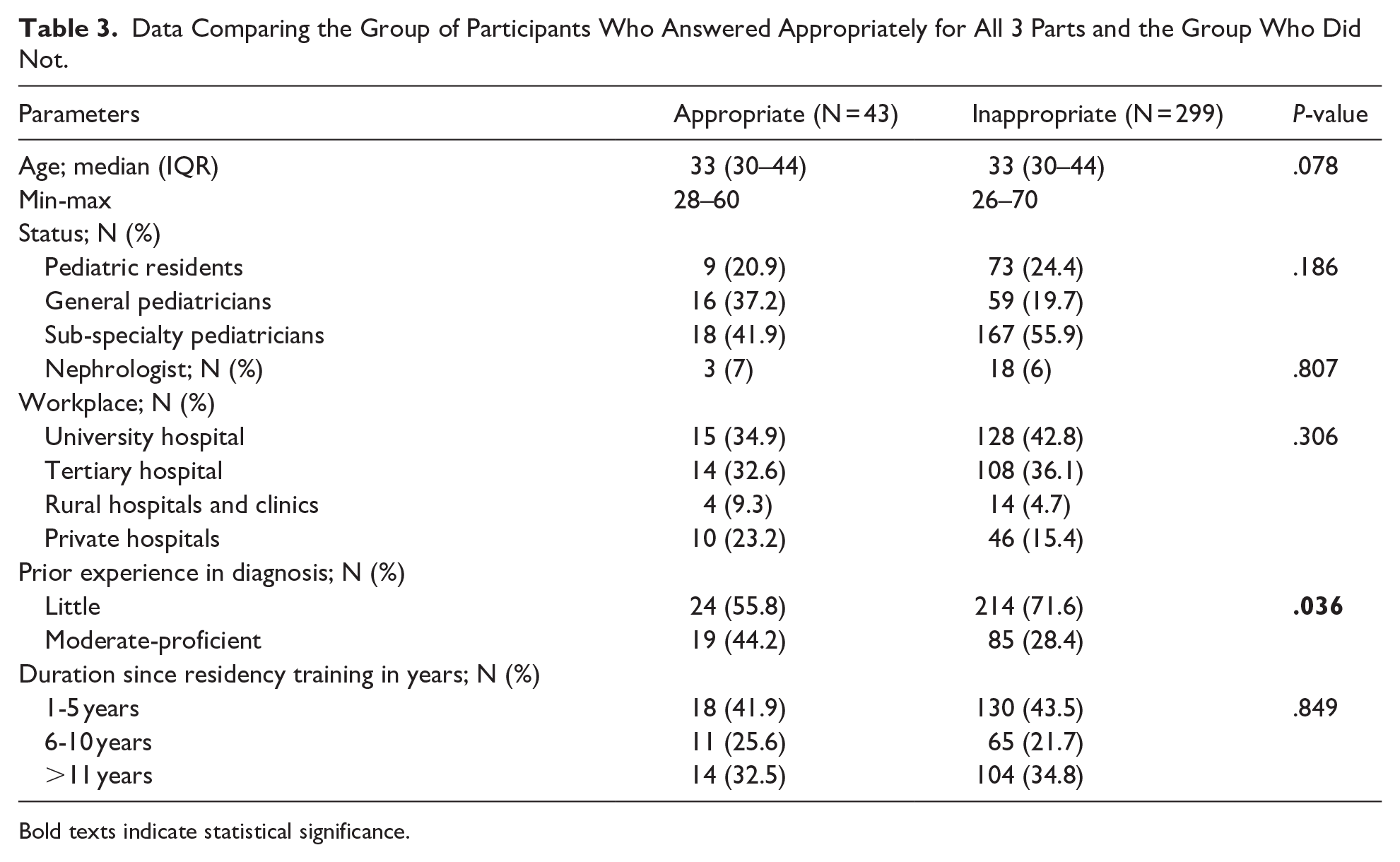
Bold texts indicate statistical significance.
Discussion
The present study revealed that about half of the participants answered appropriately in each part of the survey, while only 12.6% answered all 3 parts appropriately. Being a nephrologist or having a short duration since residency training was not shown to be favorable in answering appropriately, but having experience in diagnosing hypertension was beneficial to appropriate practice.
In contrast to the previous study that reported a higher proportion (69%) of using either mercury or aneroid sphygmomanometer 9 ; the present study and the study from North America 8 reported that 70% to 93% used the oscillometric devices. The higher proportion of sphygmomanometers in Japan and Korea could be due to the limited availability of oscillometric devices in 2010, when the study was conducted. Regarding blood pressure screening, the previous study in the Netherlands reported that 71% of physicians did not screen blood pressure in healthy children but only in those at risk of hypertension. 7 This was consistent with another study in Japan and Korea that showed 77% to 80% of respondents did not check for blood pressure routinely 9 while the present study revealed that only half of the participants were screened for blood pressure at 3 to 4 years old. These findings are concerning as many hypertensive children may not be aware of their blood pressure status, and this would result in a delay in diagnosis and put these children at risk for end-organ damage later in adulthood.
In the present study, only 55%, 55.6%, and 49.4% of the participants could appropriately answer the questions regarding diagnosis, investigation, and treatment, respectively. Being a nephrologist benefited the diagnosis, but not the investigation and treatment parts. A short duration since the residency training also did not show any benefit. However, having experience in the diagnosis of hypertension had a positive effect. There is no explanation for why being a nephrologist or having recent residency training did not show a positive impact, but it is possible that having experience with hypertensive patients would be more knowledge-retaining than learning from textbooks or lectures. Therefore, the evaluation method recommended by the World Federation of Medical Education (WFME), using the entrustable professional activity (EPA) in diagnosing and managing pediatric patients with high blood pressure, should be integrated into the pediatric residency curriculum.
For the treatment part, ACEI and ARB were the two most common anti-hypertensive medications used for primary hypertension. It accounted for 44.2% and 5.2% in the present study compared with 47% and 5% in the survey by Woroniecki and Flynn, 8 respectively. Another study by Yim et al also reported a high percentage (43%-54%) of using ACEI in the cases of primary hypertension. 9 This practice was recommended in the 2017 AAP guideline and the 2023 Joint Statement of the HyperChildNET and the European Academy of Pediatrics. 10 However, long-acting calcium channel blockers may also be used to treat hypertension in children with primary hypertension, as it was not shown to worsen metabolic complications compared to beta-blockers.
Apart from blood pressure screening, there are other parameters used to screen cardiometabolic risk, 11 such as the insulin resistance index, the triglyceride glucose index, the visceral adiposity index, etc. These parameters have been shown to predict cardiovascular outcomes later in adulthood. We believe that if the clinical practice guidelines for the screening of these parameters are simplified and easy to use, it would help pediatricians to screen, make the diagnosis, and treat early in high-risk children to mitigate the cardiovascular risk.
The strength of the present study is that the number of participants was more than 340, and it focused on questions related to the various aspects of the clinical practice in children with high blood pressure, including diagnosis, investigation, and treatment. The study involved assorted groups of healthcare providers, including pediatric residents, general pediatricians, and subspecialists. While each group had different opportunities to care for children with high blood pressure, experience in diagnosing hypertension affected the appropriate clinical practice for all 3 parts. However, the present study has some limitations. Firstly, about 10% of Thai pediatricians participated in the survey. Secondly, experience in diagnosing hypertension was self-reported, and this response may not be comparable between participants. Finally, most participants worked in the capital city of Thailand and large medical facilities with more than 200 beds. These data may not represent private practices or practices in rural areas of Thailand.
Conclusion
The present study revealed that having experience in diagnosing hypertensive children, rather than being a nephrologist or recent graduation from residency training, showed a positive effect on appropriate clinical practice in diagnosing, investigating, and treating children with primary hypertension.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251355916 – Supplemental material for Current Practice of Children With Primary Hypertension: A Survey of Pediatricians in Thailand
Supplemental material, sj-docx-1-gph-10.1177_30502225251355916 for Current Practice of Children With Primary Hypertension: A Survey of Pediatricians in Thailand by Suvaree Saelee and Kwanchai Pirojsakul in Sage Open Pediatrics
Footnotes
Acknowledgements
The authors are grateful to the Royal College of Pediatricians of Thailand for survey distribution.
Ethical Considerations
This study was approved by the ethics committee for human research (MURA 2023/499) of the Faculty of Medicine Ramathibodi Hospital, Mahidol University.
Consent to Participate
Informed consent was obtained for each participant before recruitment.
Author Contributions
SS and KP contributed substantially to the conception and design, acquisition of data, or analysis and interpretation of data; SS and KP contributed significantly to drafting the article and revising it critically for important intellectual content; SS and KP approved the manuscript of the version to be published.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.