
Abstract
Objectives. Nocturnal enuresis (NE) is a common problem among school-aged children. Nonetheless, further information on NE prevalence in Thailand is needed. The prevalence of NE and factors associated with it were investigated. Methods. A descriptive study was conducted in schools in Bangkok, Thailand, among children aged 5 to 15 years, using a questionnaire survey between November 2018 and July 2019. Results. The prevalence of primary monosymptomatic, primary nonmonosymptomatic, and secondary NEs was 9.7%, 11.6%, and 8.2%, respectively. Primary NE was associated with a family history of NE (OR = 4.05, P < .001), drinking within 2 hours before bedtime (OR = 1.77, P = .01), and deep sleep (OR = 1.62, P = .001). Conclusion. Primary NE was prevalent in this setting, and the most related factor was a family history of NE. Parents should be aware of NE in their children, especially if a child has a linked factor.
Introduction
Nocturnal enuresis (NE) or enuresis is one of the most common developmental problems in school-aged children worldwide 1 ; however, it might be ignored at home. According to the standard criteria of the International Children’s Incontinence Society (ICCS), 2 NE is an intermittent incontinence occurring exclusively during sleeping periods from the age of over 5 years. It is classified according to lower urinary tract symptoms (LUTS) and divided into monosymptomatic enuresis (MEN), which does not have daytime LUTS, and nonmonosymptomatic enuresis (NMEN), which does have NE and LUTS. The ICCS criteria also categorize MEN and NMEN as primary NE (history of never dryness) or secondary NE (bedwetting after being dry for at least 6 months).
NE is a multifactorial disorder with biological, genetic, and psychiatric or behavioral factors playing important roles in its occurrence. Crucial pathophysiology, nocturnal detrusor overactivity, excessive nocturnal urine production resulting from deficiency in vasopressin level, and difficult to arousing from sleep, particularly obstructive sleep apnea and deep sleep, are well-established mechanisms.1,3 The inherited transmission in the family is also an important factor. Moreover, constipation and attention deficit hyperactivity disorder (ADHD) are linked to NE.4-6 Other new factors, such as vitamin D deficiency, obesity and allergy, can be related to NE.7-9 However, sex, number of siblings, parents’ educational background, and parents’ employment status are also associated with NE in some previous reports.10,11
The prevalence of NE in children over 5 years is 5% to 20%,4,5,10,12 which varies according to age group, definition, and geographic area. However, only 4.2% of children had NE in Thailand, according to a report 15 years ago 13 ; this percentage might not represent the actual burden in modern times. Furthermore, not all potential factors connected to NE were considered in the previous study, particularly the new factors. Therefore, this study aimed to determine NE’s prevalence and associated factors among school-aged children in Bangkok, Thailand.
Methods
From November 2018 to July 2019, a questionnaire-based descriptive study was conducted on 5 to 15 year-old children. The inclusion criteria was healthy students aged 5 to 15 years. Children with underlying disease including diabetes mellitus, diabetes insipidus, epilepsy, congenital anomalies of the kidney and urinary tract, or who had taken diuretics were excluded. NE was defined according to the ICCS criteria. 2
The study included in 11 government or private schools in Bangkok, Thailand. The study sample was selected using multistage sampling. In the first stage, districts were selected using simple random selection. In the second stage, schools were enrolled by simple random and proportionally based on the number of students in government and private schools 1:1. The students at each school were allocated according to the total number of students.
For this study, we developed a questionnaire (Supplemental File). Three pediatricians tested its validity, with an index of item-objective congruence of greater than .6. The questionnaire was modified according to the suggestion. We also conducted a pilot study involving 100 participants to evaluate its reliability, which was demonstrated by a Cronbach’s alpha value of .72. The questionnaire consists of demographics, family income, parents’ educational background, NE events, LUTS, and specific NE-related factors, including potential risk factors such as a family history of NE, allergic history, history of ADHD, constipation, duration of breast milk, drinking a liquid before going to bed, drinking a caffeine-containing beverage, having a bathroom in the bedroom, sleep duration and problems, and stressful events. Social impact and treatment effect were also explored in the questionnaire.
The authors contacted the dean to obtain permission to conduct the study at school and explained the study and how to use the questionnaire to the teacher, who helped with the data collection. The teacher distributed questionnaires to the parents, guardians, or caregivers for self-administrated answers and written informed consent before participation. This study was approved by the Vajira institutional Ethics Committee for Human Research (COA 124/2561).
Sample Size Calculation and Statistical Analysis
The sample size was calculated using the formula (n =
The prevalence of NE is expressed as a percentage. The participants were classified into 2 groups: students with primary NE and students without NE. Because secondary NE involves complicated hypothetical factors, such as stress and psychological issues, in order to establish the contributing factors, we excluded them to identify the associated factors. The variables were compared between the groups. Continuous variables were compared by student t-test and expressed as mean and standard deviation (SD). The categorical variables were compared with the chi-square test and expressed as a percentage. The potential predictors associated with NE were identified with univariate logistic regression analysis. Furthermore, the significance of the associated factors and primary NE was determined using multiple logistic regression analysis. The final model was selected using enter method of theoretically NE-related variables with a P value of less than .1 from the univariate analysis and factor association by theory as the retention criterion. All statistical data were analyzed using SPSS version 23.0 (IBM Corp., NY, USA). A P value of less than .05 was considered statistically significant.
Results
Prevalence of NE
A total of 3009 participants returned with a completed questionnaire. Most of the participants were parents (mother [69.2%], father [19.3%], guardian/caregiver [11.5%]). The mean ± SD student age was 8.7 ± 2.4 years, and 63.1% of them were male. Primary NMEN exhibited the most prevalent rate, followed by primary MEN and secondary NE (11.6%; 95% CI, 10.5-12.8; 9.7%; 95% CI, 8.5-11.1, and 8.2%; 95% CI, 7.2-9.2, respectively). The highest prevalence of primary NE was in 7 year-olds (21.2%), and the lowest rate was observed in 15-year-olds (0.3%). Similarly, secondary NE was the most common among the 7 year-olds (24.0%) and was least common in the students aged 12 and 15 (0.4%).
Factors Associated With Primary NE
Table 1 summarizes the potential factors related to NE. Regarding the familial factors, a family member with a history of NE (P value <.01) was related to NE. However, the groups did not differ in parent’s age, family income, parents’ education, family status, or number of siblings.
Factors Associated With Primary Nocturnal Enuresis.

Abbreviations: ADHD, attention deficit hyperactive disorder; BMI, body mass index; CI, confidence interval; NE, nocturnal enuresis; OR, odds ratio.
Mean ± SD.
P value <.05.
To compare between primary NE and no NE children, male students had a lower proportion of NE (54.2%) than children without NE (64.3%) (P value <.001). In terms of sleep behavior, factors, including deep sleep, drinking water less than 2 hours before going to bed, and sharing a bedroom with their parents, were associated with NE (P value <.001, .008, and .006, respectively). Interestingly, the history of snoring was lower in children with primary NE than those without NE (P value = .03). However, neither getting fewer than 8 hours of sleep nor having a bathroom in the bedroom was related to NE. Furthermore, age, body mass index (BMI), a history of constipation, ADHD, and allergic illness were not associated with NE.
Risk Factors of Primary NE
The multiple logistic regression analysis revealed 3 significant factors related to the increased rate of primary NE. These risk factors included deep sleep (OR = 1.62; 95% CI, 1.22-2.16, P value = .001), a history of drinking fewer than 2 hours before bedtime (OR = 1.77; 95% CI, 1.13-2.80, P value = .01), and NE history in family members (OR = 4.05; 95% CI, 2.88-5.69, P value <.001). Conversely, being a male (OR = 0.62; 95% CI, 0.47-0.83, P value = .001) was statistically a protective factor. Table 2 summarizes the analysis of the associated factors.
Multiple Logistic Regression Factors Associated With Primary Nocturnal Enuresis.
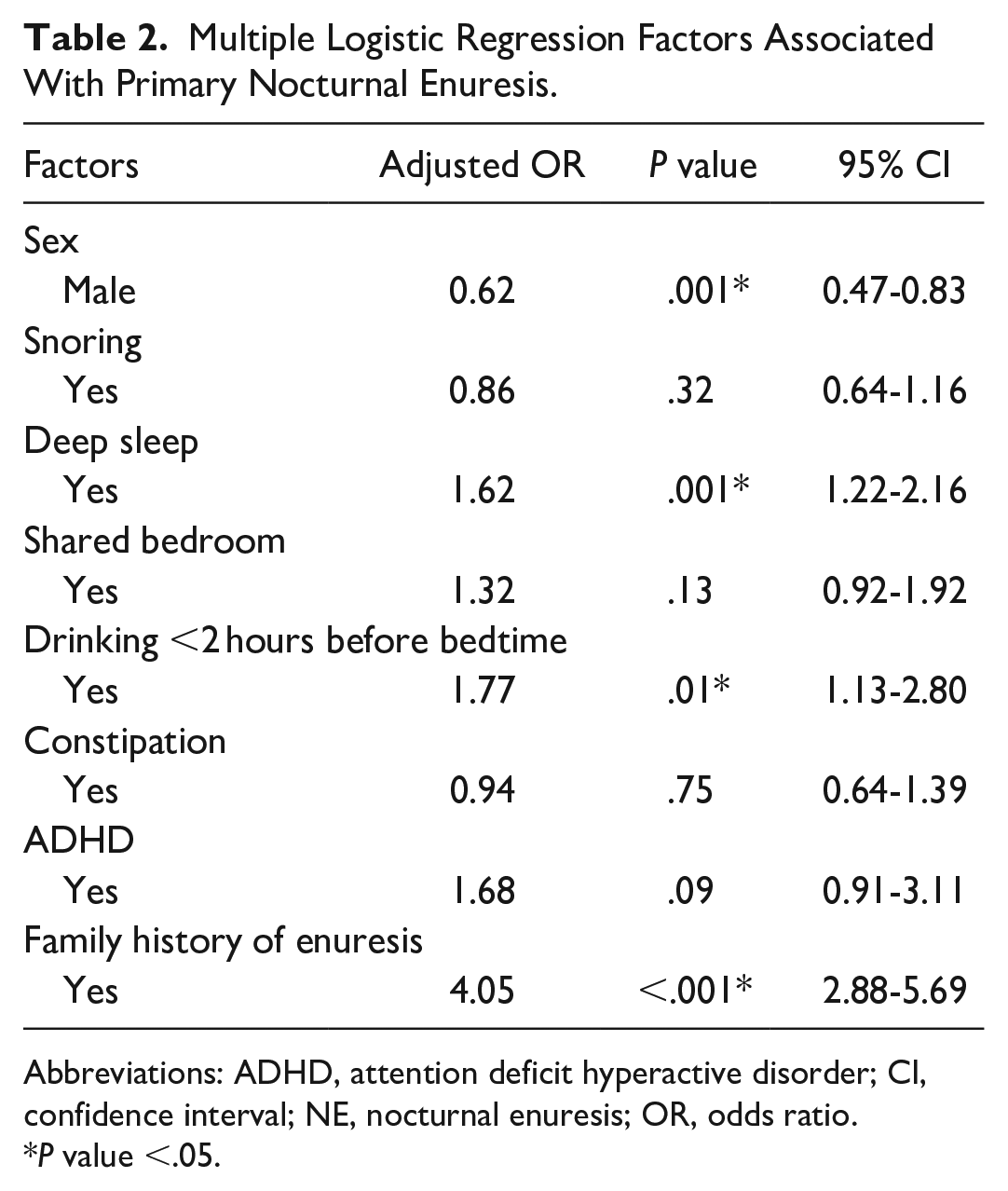
Abbreviations: ADHD, attention deficit hyperactive disorder; CI, confidence interval; NE, nocturnal enuresis; OR, odds ratio.
P value <.05.
Intervention for Primary NE
Only 3.4% (12/349) of children with NE received an intervention. The most common intervention was voiding before going to bed (10.3%). Other common interventions included waking up for voiding during sleep time (6.6%) and reducing the fluid volume consumed before bedtime (2%). The parents’ support and encourage to their children, taking medication, washing of bed linens by the child, and treating constipation were the rest methods.
Discussion
A large sample size questionnaire survey of NE in Bangkok, Thailand, showed that the prevalence of primary MEN, primary NMEN, and secondary NE was 9.7, 11.6, and 8.2%, respectively. The associated factors linked to primary NE were family history, drinking water before bedtime, and difficulty waking up at nighttime.
The prevalence of primary NE in the present study was similar to that found in studies conducted in Iran (10.2%) 12 and Pakistan (10%). 4 In addition, our study found the prevalence to be lower than that in studies conducted in the Dominican Republic (27.9%), 6 Nigeria (21.3%), 11 and Egypt (18%) 10 but higher than that found in Italy (7.2%) 14 and China (3.99%). 5 The disparate prevalence of NE worldwide could be attributed to the difference in age groups, the definition of the condition, and socioeconomic status discrepancies between developed and developing countries. Hansakunachai et al 13 reported that the prevalence of primary NE in Thailand, is 4.2% in urban areas. Sociocultural changes and higher educational levels of parents may have significantly contributed to the increase in prevalence. In contrast to a previous study, which found that mothers and fathers of children with enuresis had primary school graduation rates of 68.7% and 53.7%, respectively, the current study revealed a higher educational degree (at least bachelor degree) of mothers and fathers in 69.6% and 61.4% of the cases, respectively. Higher education may cause parents to be anxious about their children’s problems. However, parental education remains controversial with regard to NE.4,5,10
In terms of classified primary NE, this study identified primary NE as primary NMNE more frequently than primary MNE according to the parent reported any symptom of bladder disorder, such as voiding postponement, or holding maneuver, increased urinary frequency, similar to the previous study by Ferrara et al 14 and Savaser et al 15 ; however, the bladder diary and dysfunctional voiding symptom score are important tools to help diagnose concurrent LUTS. In the present study secondary NE was determined to be 8.2% which was close to the past reported in Pakistan (8.7%) 4 and Nigeria (13.6%). 11 The present study also revealed that the older age group had a reduced prevalence of NE, it could be related to brain–bladder control maturation, as found in other studies.5,10
The mechanism of NE is multifactorial, with genetic factors playing a major role. Our study demonstrated that children with family members having a history of NE were associated with an increased rate of NE, and the rate was 4.05 times, similarly found in previous studies.5,6,12 Moreover, regarding supporting evidence in a European study, 2 genetic loci at chromosome 6 and chromosome 13 were found to be significantly associated with NE. 16 In terms of sleep behavior, children with a history of deep sleep were associated with an increased rate of NE, reaching 1.62 times higher than those children without such a history in the present study, which was also found in studies by Mejias and Ramphul, 6 Hamed et al, 10 and Ferrara et al. 14 The reason why enuretic children with deep sleep may have difficult arousal, which affects incomplete stimulation and bladder relaxation, was reported by Yeung et al. 17 Our study showed an association between NE in children and a history of drinking a liquid within 2 hours of going to bed. However, this factor was not reported in a previous study. 5 Intriguingly, the male gender was a protective factor in this study, in contrast to China 5 and Nigeria. 11 In terms of sex, it was not mentioned in the pathophysiological theory to develop NE because the genes of NE are autosomes. One of the hypotheses, which differ from the present study’s finding, is that males are sleep deeper than females, 3 which must be supported by future study.
The behavioral and psychological factors related to enuresis are constipation and ADHD,11,18,19 which were not demonstrated in the present study. Additionally, it was not revealed that allergic diseases were associated with primary NE, as found by Tsai et al 20 and Yilmaz-Durmus et al 21 because most students in urban areas have a history of allergies. Regarding the relation of obesity and primary NE, the previous studies revealed conflicting results. Although Ma et al 7 and Karaci 22 found the association between obesity and primary NE, we did not found the significant relation about this issue that was similar to Wang et al 23 reported.
Only 3.4% of children with NE received interventions to improve their condition. The rate of treatment was relatively low, similar to a previous report in developing countries. 11 More importantly, we found no reports of daytime intervention that can be helpful for children with NE and daytime LUTS. Furthermore, despite the past study suggesting that lowering caffeine consumption in children lessened NE severity, the parent did not reported this in the present finding. 24
Our study has a few limitations. The study included only the participants from urban area, so generalizations can only be made within this setting. In addition, self-reporting from the participants might have affected the prevalence and associated factors with NE. The study design resulted in some recall bias, and the observed related factors may be challenging to interpret; therefore, the linked factors of secondary NE did not express. Therefore, a prospective study with questionnaires administered by researchers with bowel bladder diary and sleep quality, which aims to define the associated conditions, should be conducted in the future.
Conclusion
Primary NE is prevalent in Bangkok, Thailand. The most important contributing factor to primary NE was family history. Parents should be encouraged to report concerns about NE in their children, and significant risk factors amenable to interventions should be addressed.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X231189675 – Supplemental material for The Prevalence of Nocturnal Enuresis in Bangkok, Thailand: A Descriptive and Questionnaire Survey of 5 to 15 Year-Old School Students
Supplemental material, sj-docx-1-gph-10.1177_2333794X231189675 for The Prevalence of Nocturnal Enuresis in Bangkok, Thailand: A Descriptive and Questionnaire Survey of 5 to 15 Year-Old School Students by Ornatcha Sirimongkolchaiyakul, Chanon Sutheparank and Yupaporn Amornchaicharoensuk in Global Pediatric Health
Supplemental Material
sj-docx-2-gph-10.1177_2333794X231189675 – Supplemental material for The Prevalence of Nocturnal Enuresis in Bangkok, Thailand: A Descriptive and Questionnaire Survey of 5 to 15 Year-Old School Students
Supplemental material, sj-docx-2-gph-10.1177_2333794X231189675 for The Prevalence of Nocturnal Enuresis in Bangkok, Thailand: A Descriptive and Questionnaire Survey of 5 to 15 Year-Old School Students by Ornatcha Sirimongkolchaiyakul, Chanon Sutheparank and Yupaporn Amornchaicharoensuk in Global Pediatric Health
Footnotes
Acknowledgements
The authors thank all teachers for allowing and sending the questionnaire to all parents of participants.
Author Contributions
O.S. (correspondence) concepted and designed the study, collected and analyzed the data, wrote the manuscript, and was involved in all aspects of the paper generation. C.S. designed the study, wrote the first draft of proposal and collected the data. Y.A. added intellectual input to the paper and edited language the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Navamindradhiraj University Research Fund, Bangkok, Thailand.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.