
Abstract
Objective:
This study investigates the relationship between vitamin D levels and asthma control in children.
Methods:
A total of 100 Moroccan children (2-16 years) with asthma were assessed for serum vitamin D levels using LC/MS-MS. Asthma control was evaluated according to the GINA guidelines and the C-ACT Test.
Results:
Among the participants, 69% had well-controlled asthma, while 31% exhibited partially controlled or uncontrolled asthma. Despite a high prevalence of vitamin D deficiency, no significant correlation was found between vitamin D levels and asthma control. Multivariate analysis, adjusting for age, BMI, and sex, confirmed that there was no significant association between vitamin D levels and asthma control (OR = 1.02; 95% CI: 0.90-1.16, P = .72).
Conclusions:
Children with asthma have a high incidence of vitamin D deficiency. However, the results are not consistently in favor of a correlation between vitamin D levels and the level of asthma control.
Introduction
Asthma is one of the most common chronic diseases, affecting more than 300 million people worldwide, and it has become a huge burden on health resources 1 and the World Health Organization predicts, the number is projected to increase by more than 100 million by 2025. 2 Asthma is a prevalent chronic illness in children, uncontrolled asthma in children can lead to many health complications such as missed school days, parental work absences, restricted daily activities, emergency visits, and hospitalizations. 3
Approximately 80% of children with asthma experience their first symptoms before preschool age, making it a more common chronic inflammatory airway disorder in childhood. This statistic underscores the prominence of asthma as a prevalent chronic inflammatory airway disorder during the formative years of childhood. 2
Asthma, as a heterogeneous disease, manifests itself through chronic airway inflammation, contributing to its complexity and varied clinical presentations. This respiratory condition is defined by a history of recurring symptoms, including wheezing, shortness of breath, chest tightness, and/or a persistent cough. 4 Importantly, these symptoms exhibit variability over time and intensity, a hallmark of asthma. Asthma phenotypes depend on the nature of the trigger, whether allergic or non-allergic. Additionally, the age of onset, distinguishing between preschoolers and school-age children, further contributes to the heterogeneity of this respiratory disorder. The underlying physiopathology, characterized by high or low T helper (Th)2 cell-mediated responses and eosinophilic or non-eosinophilic patterns, adds another complexity to asthma phenotypes. 5 Genetic predisposition, environmental allergen exposure, and sensitization represent key risk factors that significantly influence the control and severity of asthma. This intricate interplay of genetic and environmental factors underscores the importance of a comprehensive approach to asthma research, diagnosis, and treatment, as it enables a more targeted and personalized approach to address the diverse phenotypic expressions of this prevalent respiratory condition. 6 Vitamin D insufficiency is thought to play a significant role in various pulmonary conditions, including asthma. The widespread prevalence of Vitamin D deficiency worldwide may partly contribute to the recent rise in asthma and allergic diseases observed over the last 5 to 6 decades, 7 and many factors may increase the prevalence of vitamin D deficiency, such as age, sex, skin pigmentation, lifestyle, diet, and exposure to the sun (latitude, season, and time spent outside). Even in locations with plenty of sun, a high prevalence has been reported.8,9
Pediatric asthma is a significant health concern in Morocco, affecting a significant portion of the country’s children. A study conducted in 2009 revealed that approximately 4.4% of children grappled with the challenges of asthma. 10 One potential approach to managing this condition is by monitoring and regulating vitamin D serum levels. This approach has garnered attention in recent years as a potential solution for improving asthma control in children.
Research indicates that vitamin D inhibits the growth of airway smooth muscle cells and impact various pathways involved in airway remodeling. This vitamin can also reduce the expression of costimulatory molecules necessary for T-cell receptor signaling and pro-inflammatory cytokines. Moreover, Vitamin D regulates adaptive lymphocyte responses, inhibiting lymphocyte proliferation and cytokine production in pro-inflammatory T helper 1 (Th1) and Th17 responses. It may potentially alleviate the severity of asthma and allergies through multiple mechanisms, including its effects on immune cells, enhanced defense against predisposing infections, reduced inflammatory responses, improved lung function, modulation of airway smooth muscle function, and reversing steroid resistance by modifying glucocorticoid receptor downregulation through interleukin production. 11 Investigating vitamin D serum levels in Moroccan children with asthma may provide valuable insights into the potential role of vitamin D in asthma control. This could lead to the development of targeted interventions, such as vitamin D supplementation, to improve asthma outcomes in this population.
The objective of the present study was to investigate the association between vitamin D status and the level of asthma control among children in Morocco.
Methods
Study Design and Setting
This is a prospective observational study conducted at the Children’s University Hospital of Rabat, Morocco, from January 2020 to October 2023. The study aimed to evaluate the relationship between vitamin D serum levels and asthma control in Moroccan children.
Study Population
A total of 100 asthmatic children (64 males and 36 females) between 2 and 16 years of age were recruited at the Pediatric Pulmonary and Allergic Diseases Unit, Rabat, Morocco. The inclusion criteria of the participants were patients assessed for asthma, with or without other allergic conditions including allergic rhinitis, atopic dermatitis/eczema, allergic conjunctivitis, and food allergies. Patients with chronic respiratory, immunodeficiency or cardiac diseases were not included in the study.
Data Collection
A questionnaire was administered to collect data regarding demographic information (age, sex, place of residence), vitamin D supplementation according the national program of nutritional supplementation immunization health. 12 characteristics of asthma symptoms, current atopy status, skin prick test (SPT) results, medications used to treat asthma, the management and severity of asthma during the previous 3 months, and the number of asthma attacks in the previous 6 months.
To assess asthma control, we used both the Global Initiative for Asthma (GINA) criteria and the Childhood Asthma Control Test (C-ACT) to provide a comprehensive evaluation. The GINA asthma control assessment classifies asthma into 3 categories: well controlled, partially controlled, and uncontrolled, based on the presence or absence of daytime symptoms, activity limitations, and nocturnal symptoms/awakenings. 13
In parallel, children completed the C-ACT questionnaire before their clinical evaluation. The C-ACT is a validated, 7-item self-administered tool that assesses asthma symptoms and their impact on daily functioning. The first 4 questions are answered by the child, using response options ranging from 0 (worst) to 3 (best), while the remaining 3 questions are answered by the parents, with response options ranging from 0 (worst) to 5 (best).14,15 In this study, we used scores ≥20 as controlled asthma and scores <20 as uncontrolled/partially controlled asthma.
We used both GINA and C-ACT to provide a comprehensive view of asthma control, combining objective clinical evaluation with patient-reported outcomes. To maintain consistency and ensure reliable comparisons, all statistical analyses were based solely on the C-ACT scores.
An electronic scale was used to measure weight (kg), and a stadiometer was used to measure height (m). We calculated BMI-for-age Z-scores using the recent World Health Organization (WHO) international growth reference/standard.16,17
Sampling and Vitamin D Assays
Two milliliters of venous blood samples were withdrawn from the peripheral vein of patients under aseptic conditions and collected in gel plus clot activator tubes. The serum was separated by centrifugation at 2000 rpm for 15 minutes at 4°C and stored at −80°C until analysis. In our study, vitamin D levels were measured with liquid chromatography-tandem mass spectrometry (LC-MS/ MS) in multiple reaction monitoring (MRM) mode, with deuterated internal standards, and results were reported in ng/mL. For our study, vitamin D levels were categorized as sufficient (>30 ng/mL), insufficient (20-30 ng/mL), or deficient (<20 ng/mL). 8
Skin Prick Test
A skin prick test was performed using standard methods. 18 Along with histamine and saline controls, the following antigens were applied to the volar surface of the forearm: house dust mite (Dermatophagoides pteronyssinus, Dermatophagoides farina, and Blomia tropicalis), animal dander (cat and dog), mold (Alternaria), mixed grass pollen, and mixed tree pollen, manufactured by ALK, France. When compared to the negative control, The test was considered positive if the mean wheal diameter measured at 15 minutes was ≥3 mm.
Statistical Analysis
Data were presented as the mean ± standard deviation for continuous variables (Normal-variables), median and interquartile range for non-normal variables, and frequencies and percentages for categorical variables. The statistical tests, chi-square test (χ2) or Fisher`s exact test for categorical variables, independent sample t test, One-Way ANOVA, and Kruskal-Wallis tests for continuous variables were used for analysis. The correlation of vitamin D levels and asthma control test (C-ACT) scores was analyzed by Spearman’s correlation analysis. The logistic regression models were used to explore the association between vitamin D levels and asthma control. Multivariate adjusted odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were estimated, adjusting for age, sex, and BMI. In all statistical analyses, P-values were 2-sided and considered statistically significant if lower than 0.05. Data analysis was performed using Jamovi (Version 2.3) software.
Ethical Considerations
The study protocol was approved by the Ethics Committee for Biomedical Research (CERB) of the Faculty of Medicine and Pharmacy of our institution and performed in accordance with the Declaration of Helsinki, good clinical practice, and all relevant international and national legislations (No. 87/18). Written informed consent was obtained from the parents and/or legal guardians of all participants.
Results
Demographic and Clinical Characteristics According to level of Asthma Control
In this study, we included a total of 100 asthmatic children. The distribution of demographic and clinical characteristics of participants according to the level of asthma control are presented in Table 1. For all children, the median age (IQR) of participants was 8 (5.9) years. There were 64% males, and most of the participants (87%) resided in urban areas. More than half of the participants (74%) had normal BMI, whereas only 10% were underweight and 16% were overweight.
Characteristics of Uncontrolled and Controlled Asthma (Numbers and Percentages; Mean Values and Standard Deviations; or Median and IQR).

Abbreviations: FP/S+M, fluticasone propionate/salmeterol+montelukast.
Skin prick test results were 63% positive for house dust mites, 20% positive for cats, 26% positive for dogs, 25% positive for mold (Alternaria Alternata), and 30% positive for pollen. The assessment of the level of asthma control revealed that 69% of children were categorized as controlled asthma and 31% as having partly controlled/uncontrolled asthma.
The mean serum vitamin D levels of the, partly controlled\uncontrolled, and controlled groups were 18.33 ± 7.36 and 16.76 ± 5.37 ng/mL, respectively (P = 0234; Figure 1).

Box plot of serum vitamin D levels in children with uncontrolled/partly controlled, and controlled asthma.
Sociodemographic and Clinical Characteristics According to Vitamin D Levels
Table 2 presents selected sociodemographic and clinical characteristics according to vitamin D levels. The 3 groups of participants did not show any differences in age, sex. However, BMI was different in 3 groups (P = .018). No correlation was present between vitamin D serum levels and C-ACT scores (P > 0.05; Figure 2).
Selected Characteristics According to Vitamin D Status (Numbers and Percentages; Mean Values and Standard Deviations; or Median and IQR).
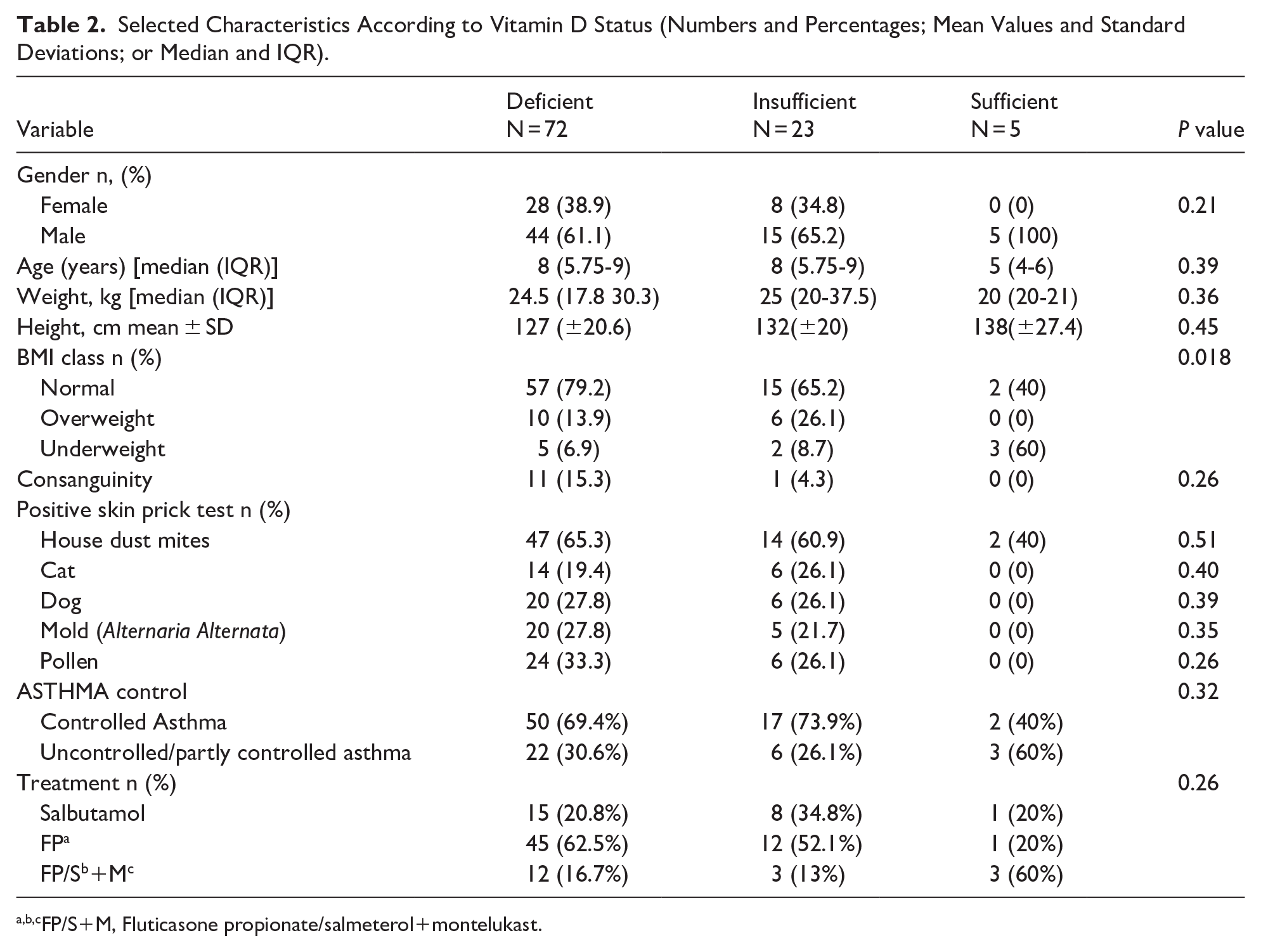
FP/S+M, Fluticasone propionate/salmeterol+montelukast.

The scatter plot shows the relationship between vitamin D serum levels and C-ACT scores.
Table 3 presents multivariate analyses of the relationship between asthma control and vitamin D levels after adjustment for age, sex, and BMI. No significant relationship between vitamin D levels and asthma control was observed in multivariate analysis (OR = 1.02 and P = 0.72). We continue with the restricted cubic spline regression model, the relationship between vitamin D serum level and asthma control seems linear (Figure 3).
Multivariate Logistic Regression Analysis to Determine the Association Between Asthma Control and Serum Levels of Vitamin D.

Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index.

Association between asthma control and Vitamin D serum levels using a restricted cubic spline. Regression model: Graphs show ORs for asthma control according to vitamin D serum levels adjusted for Sex, BMI, Age. Data were fitted by a logistic regression model, and the model was conducted with 4 knots at the 5th, 35th, 65th, 95th percentiles of vitamin D serum levels (reference is the fifth percentile). Solid lines indicate ORs, and shadow shape indicate 95% CIs.
Discussion
Vitamin D plays a critical role in immune modulation and respiratory health, with studies suggesting its involvement in asthma development and exacerbation. However, the relationship between vitamin D levels and asthma control remains inconsistent across research. 7
In Morocco, the 2019 National Nutrition Survey highlighted a significant prevalence of vitamin D deficiency and insufficiency among children, with 8% deficient and 23.4% insufficient in children aged 6 to 59 months, and 3.1% deficient and 27.3% insufficient in those aged 6 to 12 years. 12 These findings underscore vitamin D insufficiency as a public health concern, potentially influenced by limited sun exposure, dietary factors, or genetic variations in the vitamin D receptor (VDR) gene.
In our study, a high prevalence of vitamin D deficiency and insufficiency was observed in children (72% and 23%, respectively). Accordingly, only 5% of participants had sufficient vitamin D levels. These results are consistent with the findings of Esfandiar et al in Tehran, where 73.9% of asthmatic children were vitamin D deficient. 19 Another study conducted in Thailand also found that 64% of children with asthma had vitamin D deficiency. 20 However, in the present study, there were no significant differences in serum vitamin D levels between the levels of asthma control. Moreover, this study shows no significant association between vitamin D levels in pediatric asthmatic patients and acute asthma control, after adjustment for age, sex, and BMI. Al-Qerem et al reported no association between vitamin D serum levels and asthma control in children, 21 which aligns closely with our findings. Another research study conducted by Malheiro et al also found that there is no correlation between serum vitamin D levels and the control of asthma in children. 22 A systematic review and meta-analysis of randomized controlled trials by Kumar et al suggests that vitamin D supplementation might not have any protective effect in childhood asthma, further highlighting the inconsistency in findings across studies. 23
In contrast, a study carried out by Kaur et al demonstrated a significant association between low serum vitamin D3 levels and asthma in children, including a correlation between vitamin D3 levels and asthma severity and control. 24 A cross-Sectional study by Chakkamadathil et al noted that a significant proportion of children with asthma and allergic rhinitis in North Kerala had low or insufficient levels of Vitamin D. 25
Chinellato et al. examined the relationship between serum vitamin D levels and asthma control, finding a positive correlation between vitamin D levels and the management of asthma symptoms. Nevertheless, the prevalence of vitamin D deficiency/insufficiency was high in asthmatic children, with only 9.4% of children having sufficient vitamin D levels. 26
The ongoing investigation aims to better understand the complex mechanisms behind why some individuals with extremely low levels of 25-OH vitamin D remain asymptomatic, while others experience exacerbated asthma symptoms. 27 This paradox has contributed to conflicting results in studies exploring the relationship between vitamin D levels and asthma severity. 28 One possible explanation for the absence of a clear association between vitamin D status and asthma control scores in our study could be the characteristics of our study population. The majority of participants had mild asthma, characterized by infrequent exacerbations, which may have limited our ability to detect significant differences related to vitamin D levels.
Moreover, all subjects in our study presented with suboptimal 25-OH vitamin D levels, leading to a lack of contrast between groups, which might have further masked potential associations. Genetic predisposition is another critical factor that could influence indivi-dual responses to vitamin D deficiency, with certain genetic polymorphisms possibly modulating vitamin D metabolism or its impact on the immune system. 29 In addition to genetic factors, several confounding variables could have influenced the results. Environmental factors such as diet, sun exposure, and physical activity play vital roles in determining serum vitamin D levels and may also affect asthma severity. 30 Seasonal variations, often overlooked, can further complicate the interpretation of vitamin D measurements. 31 Furthermore, the heterogeneity of asthma itself must be considered. Different asthma endotypes and phenotypes—such as eosinophilic, neutrophilic, or mixed inflammation—may respond differently to vitamin D status, impacting the observed relationship. 32
Our study has some limitations. First, no control subjects were included in the study. Second, the absence of an a priori sample size calculation may have affected the statistical power of our analyses. Future studies based on a sample size computed from a specific hypothesis would help further refine these findings. Third, we did not collect detailed information about diet, sun exposure, genetics, or the effect of seasonal variation, nor did we measure serum IgE levels. Finally, the GINA and C-ACT questionnaires were not pilot-tested in the study population. Although these tools are standardized and validated, the absence of a pilot test may have limited the assessment of cultural or linguistic appropriateness, potentially affecting some responses.
This study has several strengths, including a prospective recruitment design and the use of validated tools and guidelines. Moreover, this is the first epidemiological study to investigate the relationship between vitamin D status and the level of control of asthma among children in Morocco.
It is important to note that the relationship between vitamin D and asthma control is complex and may be influenced by various factors, such as genetics, environmental exposures, and other comorbidities. Thus, it is crucial to consider these factors in future research to better understand the potential role of vitamin D in asthma management.
Conclusion
In summary, our findings suggest that there is no notable correlation between serum vitamin D levels and asthma among Moroccan children patients. We propose that additional multicenter research involving a larger cohort of patients is imperative to confirm and extend our findings. Furthermore, future investigations should explore beyond just vitamin D concentration to include the examination of vitamin D receptor expression. This comprehensive approach will offer a more nuanced understanding of the potential role of vitamin D in asthma control.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251343142 – Supplemental material for Pediatric Asthma Control: A Focus on Vitamin D Serum Levels in Moroccan Children
Supplemental material, sj-docx-1-gph-10.1177_30502225251343142 for Pediatric Asthma Control: A Focus on Vitamin D Serum Levels in Moroccan Children by Boutaina Elgharbaoui, Zhor Zeghari, Housna Arrouchi, Mohamed Khalis, Amal Thimou Izgua, Rachid Eljaoudi, Lahcen Belyamani, Azeddine Ibrahimi, Redouane Abouqal and Naima Elhafidi in Global Pediatric Health
Footnotes
Ethical Considerations
The study protocol was approved by the Ethics Committee for Biomedical Research (CERB) of the Faculty of Medicine and Pharmacy of Rabat and performed in accordance with the Declaration of Helsinki, good clinical practice, and all relevant international and national legislations (No. 87/18).
Consent to Participate
Written informed consent was obtained from the parents and/or legal guardians of all participants.
Author Contributions
[Boutaina Elgharbaoui]: Study design, data collection, statistical analysis, interpretation of results, manuscript drafting.
[Zhor Zeghari]: statistical analysis, interpretation of results.
[Housna Arrouchi]: Study design, revision of the manuscript.
[Mohamed Khalis]: Critical manuscript revision and contribution to scientific discussions.
[Amal Thimou Izgua]: Critical manuscript revision and contribution to scientific discussions.
[Rachid Eljaoudi]: Critical manuscript revision and contribution to scientific discussions.
[Lahcen Belyamani]: Overall project supervision, final validation of results, manuscript revision, and final approval.
[Azeddine Ibrahimi]: Overall project supervision, final validation of results, manuscript revision, and final approval.
[Redouane Abouqal]: Overall project supervision, final validation of results, manuscript revision, and final approval.
[Naima Elhafidi]: Overall project supervision, final validation of results, manuscript revision, and final approval.
All authors read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CNRST-PPR2 program provided financial support for this study. The authors express their gratitude toward these funding sources.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.