
Abstract
Objectives. To evaluate the interaction between childhood asthma and S. 25(OH) cholecalciferol among Bangladeshi children. Methods. This case control study was conducted in child asthma clinic, Bangladesh Shishu Hospital Institute during March-August 2021. Comparison was made between clinically-diagnosed (following GINA guideline) asthmatic children (2-12 years-old) (cases = 87) and age and sex-matched children having no respiratory illness (controls = 90) using SPSS’ (Statistical Package for Social Science, V.23.0 Windows) software. Results. Serum 25(OH) cholecalciferol was found to be significantly lower among the cases than the controls (P < .01). The cases had 3.4 times higher likelihood of having low vitamin D (combined deficient + insufficient) than the controls (P < .01). Conclusions. The results of the study demonstrate an association of Serum 25 (OH) cholecalciferol with asthma which underscores the importance of potential future trial to evaluate the efficacy of Vitamin-D supplementation for understanding the outcomes of asthmatic Bangladeshi children.
Introduction
Bronchial Asthma- A Global Public Health Issue
Asthma is a major public health problem, affecting an estimated 339 million individuals worldwide with a reported prevalence of 5% to 20% in children aged between 6 and 15 years. 1 Of 7 million people suffering from asthma in Bangladesh, an estimated 4 million remain 5 to 14 year-old children, yielding a prevalence of 7.3% in this age group. 2
Vitamin D (S. 25(OH) Cholecalciferol) and Its Role in Bronchial Asthma
Globally, Vitamin D (S. 25(OH) cholecalciferol) have been stated to play a role in asthma due to its plausible effects on bronchial tree (airway epithelium, bronchial smooth muscle) and immune-modulatory effects on innate and adaptive immune systems that may carb severity of asthma. 3 Most reports suggest low Serum 25(OH) cholecalciferol (circulating levels of Serum 25(OH) cholecalciferol of <30 ng/mL) in children with asthma remains associated with poor control of symptoms, frequent exacerbations, reduced lung function, decreased responsiveness to corticosteroids, increased medication usage and disease severity.4,5
The Knowledge Gap
To our knowledge this is the only study that specifically reported the state of childhood asthma and role of Vitamin D [Serum 25(OH) cholecalciferol] in Bangladeshi children, although there is one study that evaluated the association of asthma with low Vitamin D, without focusing on childhood asthma. 6
State of childhood asthma and role of Vitamin D [S. 25(OH) cholecalciferol] in Bangladeshi children is scarcely reported, if not unknown. The exact situation of childhood asthma and role of vitamin D is yet to be established in Bangladesh, alike other countries across Southeast Asia. We therefore, planned this study to determine if any significant association exists between Serum 25(OH) cholecalciferol and childhood asthma (prevalence and severity), which demands worthy to know toward improved management of childhood asthma.
Rationale of Conducting This Study
Childhood asthma poses significant morbidity but similar studies remain scarce in South East Asian-region, like Bangladesh. Proper documentation on the association between S. Vitamin-D [25(OH)] and asthma in Bangladeshi children lack grossly, which prompted us to conduct this study. Once our findings yield any significant association, further multi-center studies involving larger sample and healthy controls may be planned to better understand the causal relationship between vitamin D and asthma, which will be a step forward in the management of childhood asthma in countries like Bangladesh.
Research Questions
Is serum 25-hydroxycholecalciferol (25(OH) vitamin D) level lower among children with asthma?
General Objective(s) of This Study
The general objective of this study is to assess the clinico-epidemiological features of childhood asthma, aiming to determine if Serum 25(OH) cholecalciferol among asthmatic children (cases) differ from that of non-asthmatic ones (controls).
Methodology
Research Design: Case Control Study (Age- and Sex-Matched)
Study population
Cases
Children suffering from clinically diagnosed asthma recruited from Asthma clinic, department of pediatric medicine, Bangladesh Shishu Hospital & Institute (BSHI).
Controls
Age and sex-matched children having no respiratory illness recruited from other departments of pediatric medicine, BSHI.
Sample size calculation
With a proportion of 59.2% vitamin D deficiency among asthma patients having 10% absolute precision on either side of the proportion/confidence limits with a 95% confidence interval, the calculated number of cases was 87. We took 90 controls according to eligibility.
Study period
Six months: March through August 2021.
Sampling design
Asthmatic children, aged 2 to 12 years-old constituted the “cases,” and age & sex matched children having no respiratory illness were enrolled as controls.
Sample size
One hundred seventy-seven (87 cases and 90 control).
Sampling criteria/clinical confirmation/diagnosis
Asthmatic children (cases) were diagnosed based on the GINA guideline with
• History of variable respiratory symptoms (>1 of wheeze, shortness of breath, chest tightness, and cough).
• Symptoms occurring variably over time and varying in intensity.
• Often worse at night or on waking.
• Triggered by exercise, laughter, allergens, or worsen with viral infections.
• History of other allergic disease (atopic dermatitis or allergic rhinitis, food allergy).
• Therapeutic trial with low dose Inhaled Corti-costeroids and as-needed short acting beta agonist (SABA) showing clinical improvement and worsening when treatment with SABA is stopped.
Along with that, age and sex matched children, with none or minor non-respiratory illness, who had no recent or previous respiratory symptoms (within last 3 months prior to this study) were enrolled as controls.
Exclusion criteria
Children with a history and clinical features suggestive of recurrent pneumonia, bronchiolitis, pulmonary tuberculosis, foreign body aspiration, or cystic fibrosis, were discarded from sampling. Moreover, children having chronic illness (chronic kidney disease, malabsorption syndrome, and chronic liver disease), those who received Vitamin D supplementation in the past 6 months, or who were under treatment of clinical rickets and epilepsy (on anti-epileptic drugs eg, carbamazepine, phenytoin, phenobarbitone) that might affect Vitamin D levels were excluded.
Ethical approval and informed consent
Ethical approval was obtained from the Institutional Review Board (IRB) of Bangladesh Shishu Hospital and Institute. The name of the IRB is “Ethical Review Committee” and the approval number of the committee is: No.BICH-ERC: 04-02-2021. A written informed consent was obtained from the parent or legal guardian before the enrollment into the study. Additionally, children aged 5 years and older were required to provide their assent.
Details on data collection procedure
On enrollment, all the guardians were explained on the purpose, nature, aim/objectives and methodology of the study. Followed by that, a face-to-face interview was conducted by using a pre-tested hybrid designed questionnaire (open- and closed-ended/semi-structured questions) once any of the child parents signed on to a written informed consent.
Information was recorded on a questionnaire which was pilot tested on 20 respondents, which accounted for around 20% of study sample to evaluate the validity of each question and address any issues before conducting the full survey. The questionnaire included questions about the socio-demographic profile of the child’s family and information about the household’s economy. Additionally, clinico-epidemiological information was collected using a clinical data-format to record a detailed history of illness, focusing on asthma or other respiratory diseases. Each patient also underwent a thorough physical examination and a chest X-ray was done to rule out any other potential diagnoses.
However, spirometry was not performed because of 2 reasons:
Firstly, the younger children cannot follow proper instructions required for spirometry, and, secondly, to comply with the absolute preventive measure against on-going COVID-19 pandemic caused by the highly contagious severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that transmits through respiratory droplets among close contacts (both doctors/health care workers and patients being at high risk of COVID-19 transmission during most of the procedures). For the younger cohort, a “doctor diagnosis of asthma” was made which was based on an agreed consensus among resident pediatricians and consultants, scrupulously adhering to the GINA guideline. 7 This aided in diagnosis of asthma in the young cohorts and excluded any alternate diagnosis.
Laboratory investigations
All relevant pathological investigations—complete blood count, peripheral blood film, ESR, and serum IgE level were performed along with serum Vitamin D levels.
Estimation of serum 25(OH) cholecalciferol
With all aseptic precautions, 2 mL of venous blood was collected from both cases and control in plain test tubes and were thawed to settle serum. Serum 25(OH) cholecalciferol was estimated using immunofluorescence technique and mean 25(OH) vitamin D were compared between cases and controls. Serum 25(OH) cholecalciferol estimation was performed using immunofluorescence technique with Getein 1100 Immunofluorescence Quantitative Analyzer (Nanjing, China) following manufacturer provided standard procedure. Serum 25(OH) cholecalciferol level of more than or equal to 30 ng/mL was considered sufficient, level between 20 and less than 30 ng/mL as insufficient, and value less than 20 ng/mL was considered as deficient, according to “The endocrine society clinical practice guideline.” 8 The blood specimens were processed in the internationally accredited in-house microbiology laboratory, in Department of Microbiology, Child Health Research Foundation in Dhaka Shishu Hospital. 9
Data management and their analysis
All collected data were checked visually before entering into IBM computable statistical software “SPSS” (Statistical Package for Social Science, V.23.0 Windows).
While continuous data were summarized in mean and standard deviations, all discrete (categorical or ordinal) data were summarized in frequency and percentages. For end points analysis, Pearson chi-square test was used for analyzing categorical variables, as appropriate and, analysis of variance (One-way ANOVA) and t-tests, for analyzing continuous variables. However, risk estimation analysis was performed to determine impact of each variable on odds ratio (OR) and their 95% confidence intervals (CIs) of the observed variables of interest. A P-value of <.05 was considered statistically significant all through.
Results
Table 1 comparing socio-demographic profile and child’s family income of both asthmatic and non-asthmatic children yielded no significant difference in age, sex, and place of residence, and total family income.
Compound Table Comparing Demographic and Socio-economic Profile of Child’s Family Between Asthmatic and Non-asthmatic Children.

The total family monthly income (in Bangladeshi taka: BDT) of child’s family was categorized according to World Bank (WB) Data Help Desk 2016 (Calculated using USD rate: 1US $ = 84.31 BDT dated 11.06.21).
Findings of Table 2 show that the mean vitamin D level among the asthmatic children were significantly lower than that of non-asthmatic ones.
Mean Serum Vitamin D Level Among the Asthmatic and Non-asthmatic Children.
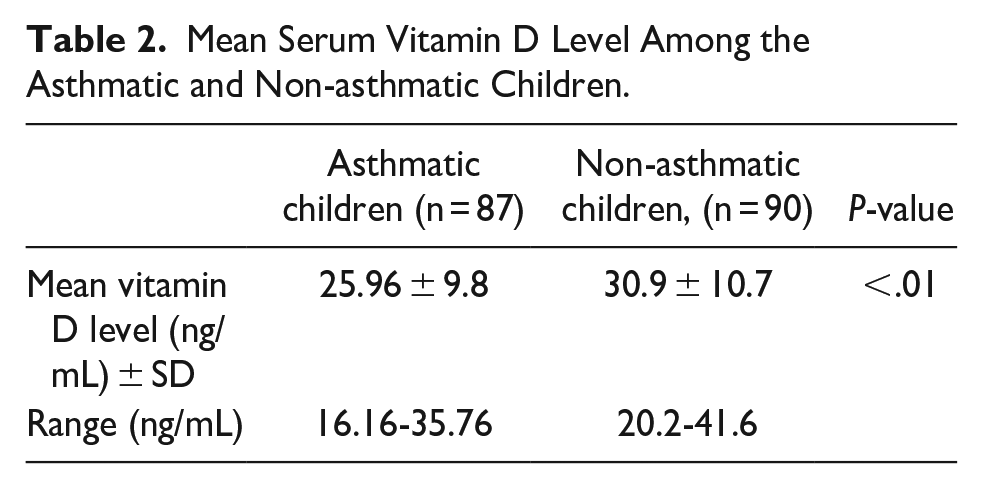
Table 3 describes a logical finding that shows that, out of all 37 vitamin D deficient children, 65% had clinically diagnosed asthma whereas it was 35% in non-asthmatic group. Similarly, among the vitamin D insufficient children, 70 (59%) belonged to asthmatic group compared to 41% in non-asthmatic one. Contrarily, among vitamin D sufficient children, 70 (68.5%) belonged to non-asthmatic (control) group compared to 31% in asthmatic groups. These differences in distribution of children differ significantly in each Vitamin D category.
Serum vitamin D Status Between Asthmatic and Non-asthmatic (Control) Children.

Children of both deficient (n = 37) and insufficient (n = 70) levels of serum vitamin D status were combined to recode and categorize as children with “Low” vitamin D status (n = 107) (Table 4).
Recoded Vitamin D Status Between Asthmatic and Non-asthmatic Control Children.

Children of both deficient (n = 37) and insufficient (n = 70) levels of serum vitamin D status were combined to recode and categorize as children with “Low” vitamin D status (n = 107).
Thus these 107 children with “Low” vitamin D status when statistically crossed with 70 children having sufficient vitamin D status and it yielded that, of asthmatic children, majority (60.7%) had “Low” vitamin D status compared to only 31.4% who had sufficient Vitamin D status (Table 4).
Contrarily, among non-asthmatic children, 68.6% had Vitamin D sufficiency against 39.3% with “Low vitamin D status.” Thus, the analysis revealed a significantly low Vitamin D status among asthmatics compared to non-asthmatic children (Table 4).
Thus, findings of Tables 3 and 4, being individual, and combined, evidenced that serum vitamin D status among asthmatic children remains significantly lower than that of non-asthmatic ones.
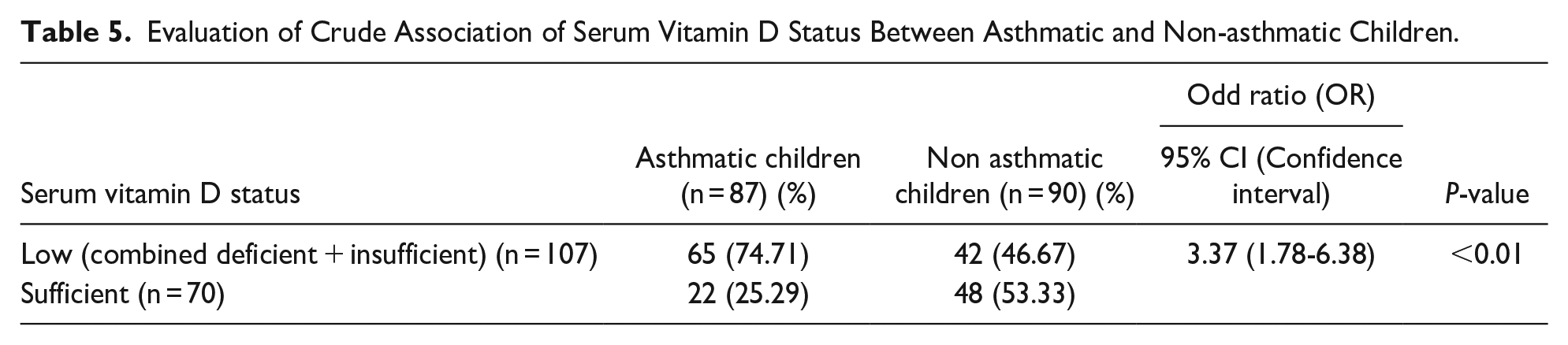
Table 5, finally, demonstrates that the likelihood of having low serum vitamin D (combined deficient + insufficient) is 3.4 times higher in the asthmatic patients than the non-asthmatic matched controls (75% vs 47%).
Evaluation of Crude Association of Serum Vitamin D Status Between Asthmatic and Non-asthmatic Children.
Discussion
The study design (case-control) that we followed to conduct this study remains like many others. This design was used in similar studies looking into the relationship between Vitamin D and asthma, conducted in Qatar, 5 USA, 10 Egypt, 11 Iran,12-14 and India.15,16 Age of both asthmatic (n = 87: cases) and non-asthmatic (n = 90: controls) ranged between 2 and 12 years, with a mean age of 6.05 ±2.05 in cases and 6.75±3.09 in controls which remains consistent to other studies in Iran,12,14 India,15,16 Turkey, 17 Israel, 18 USA, 10 and Bangladesh, 6 though we purposively excluded <2 years-old children since they reportedly suffer more from bronchiolitis as reported by Hassan et al 2 Bangladesh.
Our main findings revealed mean serum Vitamin D (25(OH) level in our asthmatic children was significantly lower than that of non-asthmatic ones. In addition, a significantly higher proportion of asthmatic children were found to have deficient or insufficient Serum Vitamin D status compared to their counterpart. This finding remains consistent to that of a finding by Sharif et al 13 reporting a low mean serum 25(OH) Vitamin D of (25.57 ± 16.62 ng/mL) among Iranian asthmatics in contrast to high serum 25(OH) Vitamin D (31.40 ± 16.76 ng/mL) in non-asthmatics ones being significantly different. 13
While, similar findings were reported by Hatami et al 12 and Alyasin et al, 14 from Iran, and Martuza et al 6 from Bangladesh it was opposed by the finding of case-control study from USA 10 showing no significant difference in Serum 25(OH) Vitamin D between asthmatic (28.64 ng/mL) and non-asthmatic controls (28.42 ng/mL) concluding that both cases and controls had subnormal Vitamin D, the difference was not significant.
Our findings demonstrate that the likelihood of having low vitamin D (combined deficient + insufficient) is more than 3 times higher in the asthmatic patients than the non-asthmatic controls.
In addition, the findings reflected in studies by Bener et al 19 and Litonjua 20 showed that there is a possibility that children with Vitamin D deficiency may be at increased the risk for developing asthma via multiple mechanisms, including poor lung growth and lung function development, sub-optimal immune system function, enhanced response to respiratory infections, and modulation of inflammation.
These aforementioned findings in Serum 25(OH) cholecalciferol level among asthmatic children remains significantly lower than that of non-asthmatic children, evidencing a probable association of Serum 25(OH) cholecalciferol level and childhood asthma- a finding that remains in agreement with the report from several studies by Hatami et al 12 (Iran), Alyasin et al 14 (Iran), Bener et al 19 (Qatar), and Kolokotroni et al 21 (Cyprus).
Though the exact reason(s) for low Serum 25(OH) cholecalciferol level in asthma is not known but may result from spending much less time outdoors to avoid asthma triggers and thus being less exposed to sunlight. In addition, many asthmatic children remain allergic to food rich in 25(OH) Vitamin D (eg, eggs, cow’s milk, cheese, red meat etc.), thus restricting themselves to diets lacking 25(OH) Vitamin D.
It is also speculated that Western lifestyle (decreased sun exposure due to increased time spent indoors and restricted physical activity) might be responsible for insufficient 25(OH) Vitamin D levels even in non-asthmatic children in addition to asthmatic ones. 22 Studies have also revealed that the inflammation associated with episodes of asthma results in depletion of 25(OH) Vitamin D and concluded that hypovitaminosis-D may be the consequence rather than cause of chronic inflammatory diseases. 23 On the contrary, in some other studies, mean 25(OH) Vitamin D levels were not significantly different between the 2 groups (cases and control).
Additional important limitations may be when comparing studies relate to differences in study design, cut off values for vitamin D deficiency and criteria for selecting the controls, the season or months in which blood samples were taken, geographic latitude of the population under study, and the age range, ethnicity and sex of the study populations as pointed out by Hilger et al. 24
Our study highlights that despite living in a tropical region receiving substantial amounts of sunlight, vitamin D insufficiency and deficiency is common in both the groups, with and without asthma, and this finding was similar to other hospital-based studies in India.16,25 In our study, among the asthmatic children, 64.8% were deficient in vitamin D, compared to only to 35% among non-asthmatics, and the difference was significant. Similar observations were noted in studies by, Awasthi and Vikram, 25 Bener et al, 19 Sharif et al, 13 and Brehm et al. 22
However, vitamin D deficiency among our cohort of asthmatic children was considerably higher than studies in Costa Rican population in 2009 showing only 28% had a deficient level. 22 Litonjua 20 found that 35% of American children were vitamin D deficient and these children were at a greater risk of severe asthma attacks. All these epidemiological studies suggest in most of the cases there is a possible association between vitamin D deficiency and asthma that support our current observations.
The strength of our study is that it was conducted at the department of pediatric medicine, BSHI which is the country’s largest tertiary care academic pediatric institution of global repute, having high quality academic and research reputation. 26 Moreover, a set of highly experienced investigators in pediatric research involving this age and sex matched case-control design made this study robust.
The use of a case-control study design in our study has several limitations. One of the main limitations is recall bias, which was influenced by the parents’ ability to accurately remember past asthma episodes and treatment. Moreover, there is a risk of selection bias. Furthermore, power analysis of our stipulated study population was not carried out and we acknowledge this as a limitation in our study.
Although age and sex-matched controls were used, while comparing the cohorts, the age category comparison has a p-value of .06, and place of residence, p = .07. Therefore, the control cohort differed significantly from the asthma case cohort at the 10% level though not at the 5% level. This is a possible limitation and need to be taken into consideration before interpretation of results.
Since serum vitamin D status and asthma is associated, further multi-center studies involving larger sample size, including children from different regions of the country should be conducted to reinforce our findings before agreeing or refuting. Furthermore, well planned randomized controlled trials should be conducted with vitamin D supplementation on children with asthma to assess its role in improving asthma symptom which will yield a prudent control strategy against childhood asthma.
Conclusions
Our findings yielded serum vitamin-D status was lower among asthmatic children compared to that of age and sex matched relatively healthy controls. The results of the study demonstrate a correlation of Serum 25(OH) cholecalciferol and asthma. Our data also attest that identification of low vitamin D status plausibly remain a predictive factor for developing childhood asthma and routine screening of vitamin D at least in children with repeated attack of wheeze may help early prediction of childhood asthma and take necessary preventive measures in minimizing the burden and morbidity of childhood asthma in low and middle income-countries, like Bangladesh. However, prior to nation-wide scale-up of the screening, a multi-center and multi-country study with larger sample size is imperative to accept or refute our observation.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241240574 – Supplemental material for Vitamin D [Serum 25(OH) cholecalciferol] Insufficiency is Associated With Childhood Asthma: Recent Case-Control Findings From Bangladesh
Supplemental material, sj-docx-1-gph-10.1177_2333794X241240574 for Vitamin D [Serum 25(OH) cholecalciferol] Insufficiency is Associated With Childhood Asthma: Recent Case-Control Findings From Bangladesh by Nabila Tabassum, Kazi Selim Anwar, Probir Kumar Sarkar, A. R. M. Luthful Kabir, Md. Abid Hossain Mollah, Dipa Saha, Md. Jahangir Alam and Mohammod Jobayer Chisti in Global Pediatric Health
Footnotes
Acknowledgements
We would like to express our sincere thanks to all parents/care-givers of the patients, physicians, nurses, members of feeding team and cleaners of the hospital for their invaluable support and contribution in patient care.
Author Contributions
NT and MAHM conceptualized the study. NT, KSA, MAHM, DS, MJA, and MJC contributed in overall design of the study. NT was involved in the collection and cleaning of data. NT, KSA, and MAHM analyzed the data. NT, KSA, MAHM, DS, MJA, and MJC interpreted the data. MJC provided the succinct support for data interpretation. NT wrote the first draft. NT, KSA, MAHM, DS, MJA, and MJC reviewed the manuscript. All the authors approved the final version of the manuscript. MJC, KSA, MAHM supervised and approved the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethical approval was obtained from the Institutional Review Board (IRB) of Bangladesh Shishu Hospital and Institute. The name of the IRB is “Ethical Review Committee” and the approval number of the committee is: No.BICH-ERC: 04-02-2021. A written informed consent was obtained from the parent or legal guardian before the enrollment in to the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.