
Abstract
This article reports a 1-year long yoga education program (YEP) experiment aimed at reducing drug dependency and promoting better asthma control for chronic asthmatic children. Participants were 450 chronic asthmatic children across 4 cities. Two measures were used: Pediatric Asthma Diary (PAD) and Childhood Asthma Control Test (C-ACT). Results indicated that intervention group children had better asthma control in terms of lower average PAD scores and higher C-ACT scores and reduced drug intake vis-à-vis the control group. Within the intervention cohort, asthma symptoms persistence was lower and control was higher for children from Asian cities, boys, Hindus, middle-class children, those whose mothers were their primary caregivers, who lived in standard family setups, who also attended the optional YEP rounds, and regularly self-practiced. The strongest predictor of lower posttest PAD scores and higher C-ACT scores was self-practice. The YEP can be used as an effective complementary treatment for chronic asthmatic children.
Introduction
Asthma is a chronic respiratory condition that is caused by interference in airways due to muscle spasms, secretion of mucus, and inflamed tissues. Children with asthma have inflamed airways, which contribute to discomfort when breathing.1,2 Certain triggers such as dust, smoke, and pollen may contribute to the narrowing of airways, causing difficulties breathing. 3 Asthma is prevalent among 7% to 10% of Asian and African children, with onset generally during the early childhood years. Based on severity of symptoms (coughing, wheezing, chest tightness) during the day and nighttime awakenings due to asthma attacks, as well as spirometry tested biomarkers such as forced expiratory volume in 1 second (FEV1) and peak expiratory flow rate, asthma is clinically classified as mild, moderate, and severe.4,5
Childhood asthma is most commonly managed with bronchodilators, which include both short-acting and long-acting inhalers, used to open up the airways and allow air to move to the lungs. 6 Breathing techniques may have similar benefits for those with asthma as some pharmacological treatments and, moreover, do not result in the side effects that are common with pharmacological treatments. For example, controlled, diaphragmatic breathing that involves focusing on abdominal muscles may assist in increasing asthma control. 7
Yoga is an ancient Indian technique and science, attributed to a group of scholars by the name Patanjali and has 8 limbs: yama or ethical relationships, niyama or discipline, asana or posture, pranayama or regulated breathing, pratyahara or drawing the senses inward, dhyana or meditation, dharana or contemplation, and samadhi or transcendence. 8 Breathing or breath control and regulation is an essential component of yoga. Yoga is essentially a noncompetitive technique with a focus on the individual. The pranayama (the breath) strengthens the diaphragm and intercostal muscles, subsequently strengthening the muscles in a practitioner’s lungs. The breath (pranayama) leads the movements, or the asanas (postures). 9 The yoga practitioner is not focused on the asanas but with their breath. There are 3 different constructs related to meditation and breathing: relaxation response, breath of fire, and bilateral segmented breathing. Relaxation response refers to quiet and natural breathing. Breath of fire is rapid breathing, and bilateral segmented breathing is rhythmic breathing at periodic intervals where the inhaling and exhaling is divided into 8 equal parts. Breath of fire marks the highest increase in heart rate, and the relaxation response and bilateral segmented breathing produce a similar dynamic on the heart rate, mostly low-frequency oscillations and slow breathing. Slow breathing is a fundamental component of these interventions.10-12
Yoga has developmental as well as therapeutic beneficial effects for children such as improving attention and concentration, enabling coping with stress and anxiety, treating ailments such as irritable bowel syndrome, among others.13-26 Yoga impact for children is contingent on several factors including parental involvement27-29 and, most important, child’s own engagement. 30
Different studies have revealed that yoga has significant importance in improving symptoms of asthmatics,31,32 but very few studies have focused on children with asthma. 33 Childhood asthma treatment essentially involves asthma control; however, the desirable pathway is to also reduce drug dependency since drugs have side effects, such as voice hoarseness and throat irritation.34,35 Furthermore, to avoid long-term medication, complementary and alternative therapies as well as breathing techniques are helpful. 36
The Present Study and Hypotheses
Given the clinical and developmental benefits of yoga for children, an experimental investigation is thus needed on the impact of a customized yoga education program (YEP) in controlling childhood asthma and reducing drug dependency. A multicity 1-year long experimental study was conducted with 450 asthmatic children in the intervention group and 450 children in the control group. Apart from assessing drug intake (salbutamol, oral corticosteroids, inhaled corticosteroids) at the pretest and posttest phases as the dependent outcome, 2 scales were used for measuring asthma control as dependent measures—Pediatric Asthma Diary (PAD) and Childhood Asthma Control Test (C-ACT). A 1-year repeated measures design was used.
Based on the literature, the following are the study hypotheses:
Method
Intervention and Control Group Profile
Table 1 presents the profiles of intervention and control group children.
Intervention Group and Control Group Profile.

Intervention and Control Group Recruitment
Intervention and control group cohorts were recruited stage-wise. At the first stage, 4 cities were selected based on contacts with pediatric chest physicians there. Four pediatric chest physicians having their private clinics were identified in Mumbai, Kathmandu, Pretoria, and Nairobi, and requested to be the nodal personnel for the study. At the second stage, the physicians provided a list of their chronic asthmatic child patients as currently in consultation, in the year 2015-2016. Across 4 cities, a list of 1220 asthmatic children and their parents/primary caregivers were contacted initially, of whom 900 children and their caregivers agreed to participate in the study, and if selected through randomization, also in the YEP. The researcher did randomization using computer-generated random number tables, whereby 450 children were assigned to the intervention group and an equal number to the control group. The intervention group children underwent the customized YEP, during the year 2016. The control group children did not participate in the customized program but were given 2 short lessons in the year on deep breathing and relaxation. Both the intervention and control group children were under medication on SOS basis (ie, as per need felt through symptom severity or otherwise), under the daily supervision of their primary caregivers, and regularly monitored by the pediatric chest physician.
Ethical Approval and Informed Consent
Informed assent was sought from all the participant children, and consent was their caregivers. No risks, arising out of participating in the study, were identified. There is no registered funder to report for this submission. Acknowledgements are due to individual philanthropists who sponsored Amazon and Flipkart gift vouchers for participant and control group cohorts as well as a small stipend for data collectors. Acknowledgements are also due to yoga experts, trainers, and pediatric chest physicians for their honorary participation. The study complies with the independent ethics committee of the University of Mumbai, India, and conforms to the guidelines of the Declaration of Helsinki, 1975, as revised in 2000 and comparable ethical standards (Ref No. 312/4/2014).
Measures
Pretest and posttest data were collected from the intervention and control group cohorts (children and caregivers) through questionnaires administered by the investigators aligned to the 4 clinics in the respective cities. Investigators were master’s degree students in social and psychological sciences and were trained via videoconferencing to collect the data. Two investigators per city worked with city-wise intervention and control group cohorts through the study period. The questionnaire comprised basic child and caregiver demographic details (city, child’s age, age of asthma onset, gender, religion, class, primary caregiver, primary caregiver’s education and occupation, and living arrangement) and asthma and general health details pretest and posttest (general caregiver–rated child health, body mass index [BMI], daily physical activities, specialist-assessed asthma severity, salbutamol, oral and inhaled corticosteroids usage pretest and posttest, and hospital visits, as well as any alternative/complementary treatment sought). Additionally, intervention and control group child cohorts maintained the PAD and the caregivers and children responded to the C-ACT, before and after the YEP. The questionnaire and the diaries were maintained in English language.
The PAD developed by Merck & Company, Inc (1995; Kenilworth, NJ) was used. The PAD is divided into 2 parts: daytime diary and nighttime diary. The daytime diary assesses the frequency and bother of daytime asthma symptoms and how they affect normal daily activities. The daytime diary has 3 questions: How much of the time did you have trouble breathing today? How much did your asthma bother you today? How much of the time did your asthma limit your activities today? Scoring was done on a Likert-type scale ranging from 0 (no symptoms or activity limitations) to 5 (most symptoms or activity limitations). The nighttime diary has 1 question that examines the number of awakenings caused by asthma symptoms on a scale of 0 (no awakenings) to 3 (awake all night). Total score ranges from 0 to 18, with higher scores indicating daily greater trouble breathing, asthma bother, activity limitation, and nighttime awakening. Studies have examined the validity and reliability of PAD for 6- to 11-year-old children and found acceptable clinical validity, construct and concurrent validity, as well as cross-cultural application.37-39 For the present study, intervention and control group children completed the asthma symptom diary twice daily for the 1-year study period. Daily total scores were taken and summed for the entire period and divided by the total number of days (=360). The average scores ranged from 0 to 18, with higher average scores indicating greater persistence of asthma symptoms. For the present study, Cronbach’s α = .92; item-scale intercorrelation = .91; Pearson’s r = .88.
Additionally, the C-ACT developed by Liu et al 40 and supported by GlaxoSmithKline (Brentford, England) is a child-reported and caregiver-reported questionnaire that has 7 questions, of which 4 are to be answered by the child and 3 by the parent/primary caregiver. The 4 child questions are rated on a 4-point Likert-type system: How was your asthma today? (0 = very bad to 3 = very good); How much of a problem is your asthma when you run, exercise, or play sports? (0 = It’s a big problem, I can’t do what I want to do, to 3 = It’s not a problem); Do you cough because of your asthma? And do you wake up at night because of your asthma? (0 = yes, all of the time, to 3 = no, none of the time). The 3 caregiver questions assess whether the child has asthma symptoms at daytime, wheezing and nighttime awakenings during the past 4 weeks. These are rated from 0 = everyday to 5 = not at all. Total score ranges from 0 to 27, with lower scores indicating poorly controlled asthma and higher scores indicating well-controlled asthma.
Studies have examined the validity and reliability of C-ACT with 6- to 11-year-old children and found acceptable clinical validity, construct and concurrent validity, and cross-cultural application.41,42 For the present study, intervention and control group children and their primary caregivers completed the C-ACT at the pretest and posttest phases. For the present study, Cronbach’s α = .93; item-scale intercorrelation = .92; Pearson’s r = .89.
Yoga Education Program Details
YEP Development
The YEP was developed by 4 yoga experts based in Mumbai, India, and affiliated to a yoga institution having intercountry branches or students based in different countries and practicing yoga there. Four meetings were held during the year 2015 to deliberate on the aims and content of a customized YEP for chronic asthmatic children. The aims of the customized YEP were to promote better asthma control, reduce drug dependency, and thereby contribute to a lifestyle change in chronic asthmatic children. The key features of the YEP as determined through the deliberations were the following: (1) guided breathing interspersed with relaxation; (2) slowness in breathing; (3) continuity; (4) inner watchful awareness; (5) feeling of changes in breathing, heartbeat, blood flow, and the resonance of sound; and (6) recognition of linear, surface, 3-dimensional, and all pervasive awareness.
Content of the YEP
One round of the customized YEP comprised 3-day 30-minute lessons conducted by the yoga trainers. Twelve such rounds were conducted in each of the cities (once a month), of which 8 rounds were considered mandatory and the remaining 4 were optional. The repertoire of each of the lessons in a single round was as follows:
Sitting still, normal breathing, and observing the breath
Slow and rhythmic breathing
Three-part breath—placing one hand on the belly and one on the rib cage and slowly observing all the inhalations and exhalations, then placing one hand on the chest, just below the collarbone and observing all the inhalations and exhalations
Ocean breath—completely filling the lungs while slightly contracting the throat and breathing through the nose
Alternate nostrils breathing—alternating the blockage of each nostril to channel the air in a concentrated flow
Skull brightener breathing—short powerful exhales and passive inhales
Relaxation and normal breathing
Each of the 4 techniques were performed under the guidance of trained instructors and repeated thrice in 1 round. Intervention group children and their parents were then given a picture-illustrated instruction sheet comprising the above-mentioned techniques for regular self-practice, once daily, until the next round. Furthermore, there was no compulsion of goal attainment, and it was emphasized that the participants could do the lessons and practice as per their capacities and pace.
Deliverers and Setting
Four yoga trainers based in each of the 4 cities conducted the yoga lessons at the premises of the pediatric clinics. Yoga trainers were identified based on the recommendations of yoga experts and who had prior training experience with children. YEP was delivered with batches of children: mean batch size = 32.21, SD = 3.67.
Statistical Methods
Pretest and posttest drug usage for the intervention and control group children have been recorded. Pretest and posttest scores of the children on the PAD and C-ACT have been analyzed through 1-way analyses of variance with Scheffe’s post hoc criterion to examine within-group differences. Paired t tests were used to compare pretest and posttest outcome measure scores. Posttest outcome measure scores of the intervention group children were further analyzed through the following: multivariate analysis of variance to examine the multivariate independent effects on the posttest outcomes; Kruskal-Wallis nonparametric tests and Bonferroni’s adjusted α levels to examine the independent, pair-wise, and combined effects of the significant demographic and caregiver variables on the posttest dependent outcomes; and hierarchical regression models to examine the strongest predictor of posttest outcomes.
Results
Primary analyses comprised 450 chronic asthmatic children in the intervention group and an equal number in the control group. The YEP was delivered as intended in terms of 12 rounds in the year, of which 8 were mandatory and the remaining 4 were optional. Of the 450 intervention group children, 123 (22.78%) children attended the mandatory 8 rounds only and 417 (77.22%) children attended the optional rounds (83 children attended 9 rounds, 92 children attended 10 rounds, 86 children attended 11 rounds, and 156 children attended all the 12 rounds). The self-practice report indicated that 386 (71.48%) intervention group children regularly self-practiced the yoga lessons and 154 (28.52%) children did so occasionally. Figure 1 illustrates the aforementioned details.

Flow of participants through each stage of the experiment.
The intent-to-treat analyses compare the pre- and post-YEP outcome measure scores of the intervention and control group children. Post-YEP scores of the intervention group children have been further analyzed for significant predictors.
Health and Asthma Conditions and Drug Usage: Pretest and Posttest
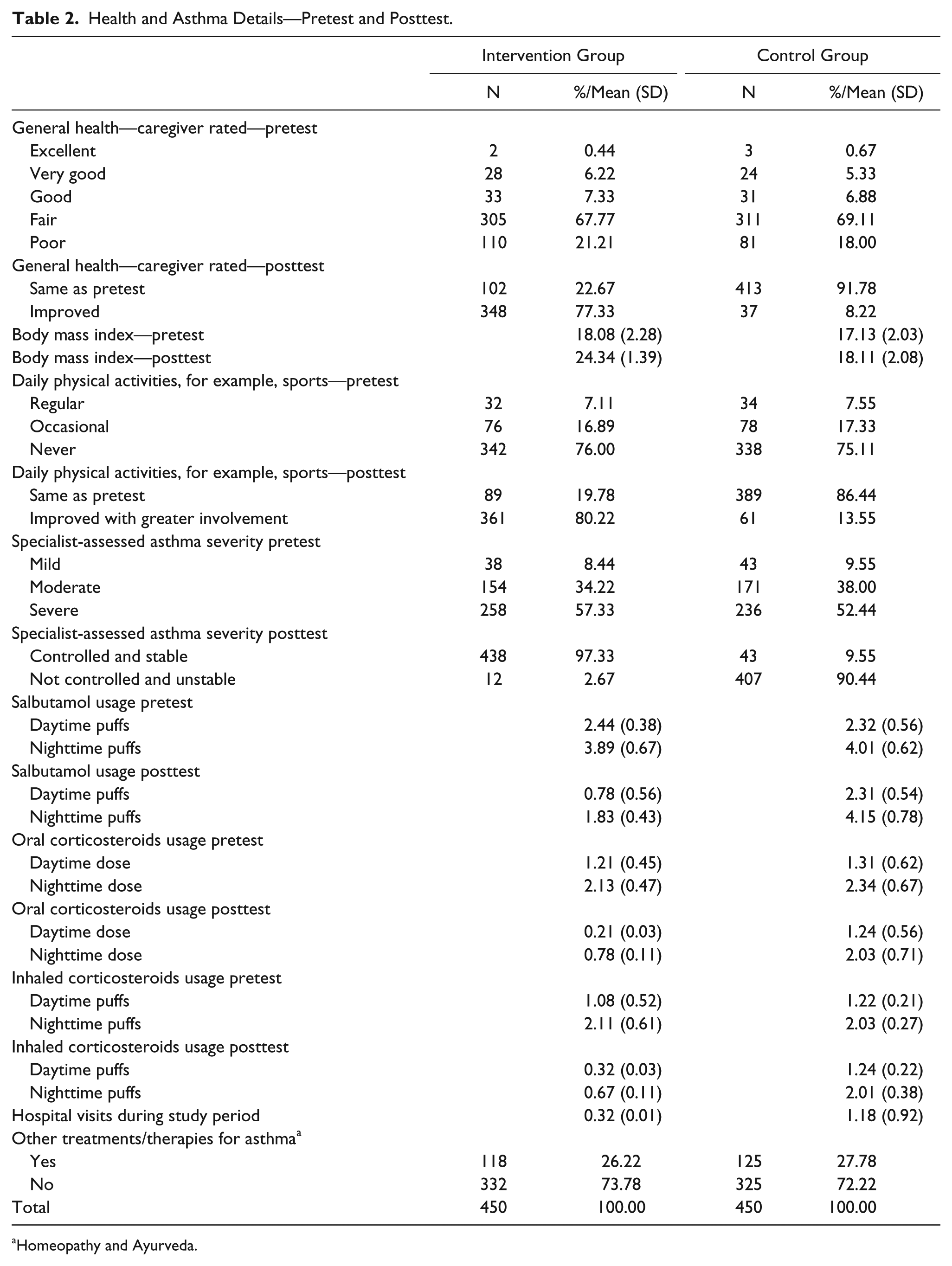
Table 2 depicts the pretest and posttest general health, asthma conditions, and drug usage of the intervention and control group children.
Health and Asthma Details—Pretest and Posttest.
Homeopathy and Ayurveda.
PAD and C-ACT Scores
Control Group Pretest
The average pretest PAD score of the control group was 14.48 (SD = 2.33). The average pretest C-ACT score of the control group was 11.39 (SD = 4.35). The effects of gender and class were significant. Post hoc analyses using Scheffe post hoc criterion for significance indicated that within the control group, the pretest PAD scores were higher and C-ACT scores were lower for boys vis-à-vis girls and for middle-class children vis-à-vis elite children.
Control Group Posttest
The average posttest PAD score of the control group was 14.17 (SD = 2.42). The average posttest C-ACT score of the control group was 12.03 (SD = 5.11). The effects of gender, class, and living arrangements were significant. Post hoc analyses using Scheffe post hoc criterion for significance indicated that within the control group, the posttest PAD scores were higher and C-ACT scores were lower for boys vis-à-vis girls, middle-class children vis-à-vis elite children, and children living in single parent families vis-à-vis those living in standard family setups.
Intervention Group Pretest
The average pretest PAD score of the intervention group was 14.88 (SD = 3.46). The average pretest C-ACT score of the intervention group was 12.48 (SD = 3.12). The effects of gender and living arrangements were significant. Post hoc analyses using Scheffe post hoc criterion for significance indicated that within the intervention group, the pretest PAD scores were higher and C-ACT scores were lower for boys vis-à-vis girls and children living in single parent families vis-à-vis those living in standard family setups.
Intervention Group Posttest
The average posttest PAD score of the intervention group children was 4.82 (SD = 2.76). The average posttest C-ACT score of the intervention group children was 24.04 (SD = 3.65). The effects of city, gender, religion, class, primary caregiver, living arrangement, rounds of YEP, and self-practice were significant. Post hoc analyses using Scheffe post hoc criterion for significance indicated that within the intervention group, the posttest PAD scores were lower and C-ACT scores were higher for intervention group children from Asian cities vis-à-vis African cities, boys vis-à-vis girls, Hindus vis-à-vis Christians, middle class vis-à-vis elite, those whose mothers were their primary caregivers vis-à-vis those whose fathers or grandparents/kin were their primary caregivers, those who lived in standard family arrangements vis-à-vis in single parent families, those who attended 9 to 12 rounds of the YEP vis-à-vis the mandatory 8 rounds, and those who regularly self-practiced vis-à-vis those who did so occasionally.
Comparison
The intervention and control group children were equal at baseline. Posttest PAD scores of the intervention group children were significantly lower, and C-ACT scores were significantly higher in comparison to the control group. Hence, intervention group children had lesser persistent asthma symptoms and well-controlled asthma after participation in the YEP. Table 3 depicts the paired t test results.
Comparison of Pretest and Posttest PAD and C-ACT Scores of the Intervention and Control Group Children: Paired t Tests.

Abbreviations: PAD, Pediatric Asthma Diary; C-ACT Childhood Asthma Control Test.
Degrees of freedom = 449.
P ≤ .05. **P ≤ .01.
Pretest and Posttest PAD and C-ACT Scores of the Participant Children
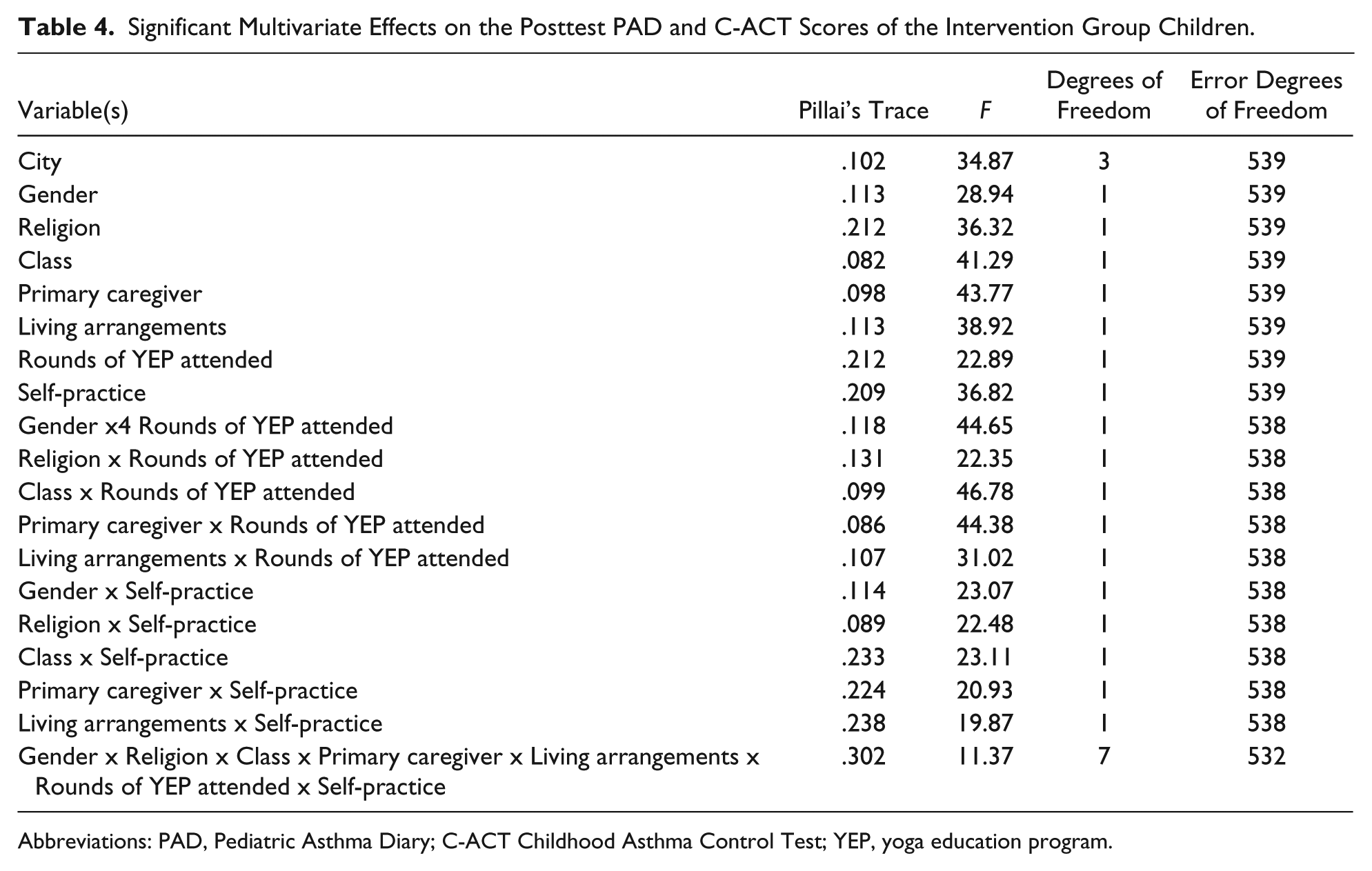
The pretest and posttest PAD and C-ACT scores were further subjected to a multivariate analysis of variance with 8 independent variables: city, gender, religion, class, primary caregiver, living arrangements, rounds of YEP, and self-practice. Significant associations were examined further by nonparametric testing (Kruskal-Wallis). Apart from the individual variables independently affecting the dependent outcomes, the following interaction effects were significant: gender, religion, class, primary caregiver, living arrangements, and rounds of YEP attended; gender, religion, class, primary caregiver, living arrangements and self-practice, and rounds of YEP attended and self-practice. Tests were further conducted using Bonferroni-adjusted α levels of .00625 per test (.05/8). The independent variables and the pairwise interactions were significant. The combined effects were also significant. The average posttest PAD scores were lower under the more significant independent and predictor variables (ie, for intervention group children from Asian cities, boys, Hindus, middle class, those whose mothers were their primary caregivers, those who lived in standard family setups, who voluntarily attended the optional YEP rounds, and regularly self-practiced; mean [M] = 3.04, SD = 1.32) vis-à-vis under the less significant independent and predictor variables (ie, for intervention group children from African cities, girls, Christians, elite, those whose fathers or grandparents/kin were their primary caregivers, those who lived in single parent families, who attended only the mandatory 8 YEP rounds, and who occasionally self-practiced; M = 5.21, SD = 2.02), F(7, 532) = 67.21, P ≤ .01. The average posttest C-ACT scores were higher under the more significant independent and predictor variables (M = 25.01, SD = 1.34) vis-à-vis under the less significant independent and predictor variables (M = 21.36, SD = 2.35), F(7, 532) = 32.14, P ≤ . 001. Table 4 depicts the significant multivariate effects.
Significant Multivariate Effects on the Posttest PAD and C-ACT Scores of the Intervention Group Children.
Abbreviations: PAD, Pediatric Asthma Diary; C-ACT Childhood Asthma Control Test; YEP, yoga education program.
Table 5 depicts the 5-step hierarchical regression model of the variables predicting the posttest PAD scores of intervention group children. At step 1, domicile city of the intervention group children contributed significantly to the regression model, F(3, 539) = 28.91, P ≤ .01, and accounted for 4% of the variation in the posttest PAD scores of the intervention group children. Introducing the variables gender and religion explained an additional 15.1% of the variation in the posttest PAD scores, and this change in R2Ç was significant, F(2, 537) = 18.32, P ≤ .01. Adding class, primary caregiver and living arrangements to the regression model further explained an additional 23.2% of the variation in the regression model, and this change in R2 was significant, F(3, 534) = 31.91, P = .02. At step 4, adding the mediator variable, viz, rounds of YEP attended explained 11% of the variation in the posttest PAD scores, and this change in R2 was also significant, F(1, 533) = 28.23, P ≤ .01. At step 5, adding the variable self-practice explained an additional 17% of the variation in the posttest PAD scores of the intervention group children, and this change in R2 was significant, F(1, 532) = 2.09, P ≤ .001. When all the 8 variables were included in step 5 of the regression model, self-practice emerged as the most important predictor, which uniquely explained 17% of the variation in the posttest PAD scores. Together, all the 8 independent and predictor variables accounted for 70.3% variation in the posttest PAD scores of the intervention group children.
Summary of Hierarchical Regression Analysis for Variables Predicting Intervention Group Children’s Posttest PAD Scores (N = 450).

Abbreviations: PAD, Pediatric Asthma Diary; YEP, yoga education program.
P ≤ .05. **P ≤ .01. ***P ≤ .001.
Table 6 depicts the 5-step hierarchical regression model of the variables predicting the posttest C-ACT scores of intervention group children. At step 1, domicile city of the intervention group children contributed significantly to the regression model, F (3, 539) = 26.43, P ≤ .01, and accounted for 5.2% of the variation in the posttest C-ACT scores of the intervention group children. Introducing the variables gender and religion explained an additional 14% of the variation in the posttest C-ACT scores, and this change in R2 was significant, F(2, 537) = 23.83, P ≤ .01. Adding class, primary caregiver and living arrangements to the regression model further explained an additional 24% of the variation in the regression model, and this change in R2 was significant, F(3, 534) = 37.22, P = .02. At step 4, adding the mediator variable, viz, rounds of YEP attended explained 12% of the variation in the posttest C-ACT scores, and this change in R2 was also significant, F(1, 533) = 17.29, P ≤ .01. At step 5, adding the variable self-practice explained an additional 18% of the variation in the posttest C-ACT scores of the intervention group children, and this change in R2 was significant, F(1, 532) = 3.45, P ≤ .001. When all the 8 variables were included in step 5 of the regression model, self-practice emerged as the most important predictor, which uniquely explained 18% of the variation in the posttest PAD scores. Together, all the 8 independent and predictor variables accounted for 73.2% variation in the posttest C-ACT scores of the intervention group children.
Summary of Hierarchical Regression Analysis for Variables Predicting Intervention Group Children’s Posttest C-ACT Scores (N = 450).

Abbreviations: C-ACT Childhood Asthma Control Test; YEP, yoga education program.
P ≤ .05. **P ≤ .01. ***P ≤ .001.
Discussion and Conclusion
Results support the initial hypotheses. Intervention group children who underwent the YEP had better asthma control in terms of lower average PAD scores and higher C-ACT scores and reduced drug intake vis-à-vis the control group. The extent of YEP impact varied based on intervention group children’s demographic and biographical variables, caregiver variables, and YEP-related variables such as rounds of YEP attended and self-practice regularity. The strongest predictor of YEP impact on the dependent outcomes was intervention group children’s own engagement with the program through self-practice.
Intervention and control group children were equal at baseline on all the parameters. Pretest caregiver-rated general health of majority of the intervention and control group children was fair. Posttest general health of the intervention group exhibited improvement. Intervention and control group children had lower BMI at the pretest phase. At the posttest phase, intervention group children attained normal weight and BMI. Majority of the intervention and control group children did not participate in daily physical activities such as sports at the pretest phase. Posttest report indicated improved and greater involvement of the intervention group children in daily physical activities. Intervention group children’s asthma as assessed by specialists was better controlled and stable. This reflected in lower daytime and nighttime usage of salbutamol, oral corticosteroids, inhaled corticosteroids, and very few or no hospital visits by intervention group children during the study period.
Within the control group, boys and middle-class children as well as those who lived in single-parent families had greater persistence of asthma symptoms and poorer asthma control vis-à-vis girls and elite children and those who lived in standard family setups. At the posttest phase, control group children’s scores exhibited no significant difference. Within the intervention group, at the pretest phase, boys and those who lived in single parent families had greater persistence of asthma symptoms and poorer asthma control.
Overall, the posttest scores of the intervention group exhibited lower persistence of asthma symptoms and better asthma control. However, within the intervention group, posttest PAD scores were lower and C-ACT scores were higher for intervention group children from Mumbai and Kathmandu, boys, Hindus, middle-class children, those whose mothers were their primary caregivers, those who lived in standard family setups, who also attended the optional YEP rounds, and regularly self-practiced. Multivariate analyses indicated that girls, Hindus, middle-class participants, those whose mothers were their primary caregivers, and those who lived in standard family arrangements were more likely to also attend the optional YEP rounds and regularly self-practice. The strongest predictor of lower posttest PAD scores and higher C-ACT scores was self-practice.
Results indicated that whereas overall the YEP was effective in reducing persistence of asthma symptoms and promoting asthma control among participants, within-participant group differences in impact were seen. The YEP was more effective for intervention group children from Mumbai and Kathmandu (Asian cities) vis-à-vis Nairobi and Pretoria (African cities) as well as for Hindu children vis-à-vis Christian participants. Though more research is required to draw definitive conclusions, these differences in program impact due to ethnicity and religious affiliation/belonging reflect the need for more a culturally attuned and diversity incorporating YEP, which could take into account these differences and have a more universal appeal.
Gender differences were distinctive; boys exhibited greater persistence of asthma symptoms and poorly controlled asthma pretest vis-à-vis girls, corroborating earlier research on gender differences in childhood asthma and the possibility of underdiagnosed asthma among girls.43-45 However, boys were also more responsive to the YEP intervention, which adds a dimension to childhood asthma treatment literature. Furthermore, stable family environments and caregiver involvement in the treatment process were significant predictors. Specifically mothers’ involvement was a significant determinant of enhanced program impact in asthma treatment and control, which corroborates earlier research.46-49
Economic class was another significant demographic factor in treatment response. Middle-class children were more responsive to the YEP vis-à-vis elite children. Though more class-specific research is required, this could signify that elite children need more intensive interventions or that the YEP may need some modifications to appeal to that cohort.
Two significant YEP-related predictors that determined outcome measure effects were rounds of YEP attended and self-practice. Participant children’s own involvement in the program through voluntary attendance in optional rounds and regular self-practice were critical to program impact. This corroborates yoga technique literature that places a premium on self-engagement for enhancing impact as its distinctive trait. 8
This study has some of the following limitations. Intervening life course events, seasonal and psychosomatic triggers, which may affect asthma symptoms and severity or lead to fluctuations, have not been considered in the present study. Data need to be gathered at shorter intervals to examine YEP efficacy in an iterative and intensive manner. Other parental/primary caregiver variables, such as changes in marital status, data related to siblings and siblings’ behavior toward asthma attacks and symptoms, and corresponding care, also need to be considered in future investigations. Furthermore, since asthma symptoms and breathing discomfort experiences can be quite unique and individual-specific, it is also essential to capture qualitative narratives of post-YEP experiences of being able to breathe freely and have lesser distress.
Results have the following practical applications. The YEP can be used as an effective complementary treatment to reduce drug dependency, lower persistence of asthma symptoms, and promote better asthma control among chronic asthmatic children. Some variations would be needed in the program tenets or instructions to accommodate ethnic diversities and indigenous belief systems and cultures. Factors that support and bolster YEP effectiveness for asthmatic children would also need to be cultivated, such as parental involvement, stable family environments, and children’s own engagement with the program.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.