
Abstract
Cerebellopontine meningiomas in pediatric patients are exceptionally rare, with cases involving extracranial extension being even less common. These tumors present significant surgical challenges due to their complex anatomical location and potential for extensive involvement of surrounding structures. Imaging is crucial in evaluating the extent of the tumor, assessing cranial nerve involvement, excluding other differential diagnoses, and facilitating optimal treatment planning. Unlike their adult counterparts, pediatric meningiomas often exhibit a more aggressive growth pattern, higher recurrence rates, and poorer prognostic outcomes. We report the case of a 12-year-old boy who presented with progressive hearing loss, vertigo, and ataxia. Imaging revealed a cerebellopontine mass with invasion of the jugular foramen and extension into the parapharyngeal space via the hypoglossal canal. Histopathological analysis confirmed the diagnosis of meningothelial meningioma.
Keywords
Introduction
Meningiomas are extra-axial tumors and the most common neoplasm of the meninges. These non-glial tumors originate from meningocytes or arachnoid cap cells and are typically associated with adults, with a marked rarity in children. In the pediatric population, meningiomas account for less than 5% of all brain tumors, and cerebellopontine angle (CPA) involvement is exceedingly uncommon.1,2
Our case highlights a 12-year-old boy with a rare cerebellopontine meningioma exhibiting extracranial extension into the parapharyngeal space through the hypoglossal canal. Direct extracranial extension of meningiomas is a rarity, with only a limited number of cases documented in the literature. This unusual presentation underscores the complexity of diagnosing and managing these tumors in pediatric patients.2,3
Comprehensive preoperative imaging is essential for accurately assessing tumor extent, involvement of adjacent structures, and differentiating it from other CPA lesions, such as vestibular schwannomas or epidermoid cysts. MRI is particularly critical in defining the tumor’s boundaries and its potential extracranial spread. 3
Given their rarity and complexity, pediatric meningiomas require a multidisciplinary approach for optimal management. This includes careful surgical planning to achieve maximal safe resection while preserving neurological function, supplemented by adjuvant therapies when necessary to address residual or recurrent disease. 3
Case Report
We report the case of a 12-year-old boy with no prior medical history who presented with progressive hearing loss, vertigo, and ataxia. Physical examination revealed multiple café-au-lait spots scattered across his body. Magnetic resonance imaging (MRI) revealed a large mass centered in the right cerebellopontine angle with broad dural-based implantation. The mass exhibited intermediate T2 and FLAIR signal intensities (Figure 1), intense gadolinium enhancement, and diffusion restriction on DWI sequences. It invaded the ipsilateral sigmoid sinus and jugular bulb, encased the internal carotid artery circumferentially, and caused significant mass effect on the brainstem and cerebellar hemispheres, displacing these structures (Figures 1 and 2). Additionally, the lesion infiltrated the internal auditory canal, acoustic-facial nerves, cochleovestibular structures, and extended into the parapharyngeal and retrostyloid spaces via the hypoglossal canal, which was also affected (Figures 2 and 3).

MRI T2 axial sequence demonstrating: (a) voluminous mass exhibiting a intermediate T2 signal, centered on the right cerebellopontine angle (Blue star) exerting a mass effect on the brainstem and cerebellar hemispheres (Blue arrow) and (b) the mass extends to the ipsilateral parapharyngeal space (Blue star).

Axial MRI T1 sequence after Gadolinium administration showing: (a) voluminous mass of the right cerebellopontine angle with homogenous enhancement (Blue star) invading the ipsilateral sigmoid sinus (Blue arrow) and extends to the internal auditory canal (Blue arrow head), (b) the mass infiltrate the jugular bulb (Blue arrow), (c) the mass extends to the parapharygeal and retro styloid space via the hypoglossal canal (Blue arrow), and (d) the mass occupies the cerebello-medullary cistern and the median aperture (Blue arrow).

Coronal MRI T1 sequence after Gadolinium administration showing: (a) Homogeneous enhancing mass exerting a mass effect on the ipsilateral cerebellar tent (Blue arrow) and (b) mass extending to the parapharygeal space through the hypoglossal canal (Blue arrow).
MRI also identified a second enhancing lesion in the contralateral auditory canal, consistent with another meningioma (Figure 4) . Biopsy of the right cerebellopontine mass confirmed a meningoepithelial meningioma (Figure 5). Laboratory investigations subsequently diagnosed neurofibromatosis type 2 (NF2). The patient was hospitalized and underwent a partial surgical resection of the mass through a posterior occipital approach, with the patient positioned in the Concorde position to facilitate access to the tumor. A postoperative CT scan was performed, revealing a residual tumor predominantly located in the parapharyngeal space, along with hemorrhagic changes and evidence of subarachnoid hemorrhage at the level of the ipsilateral tentorium cerebelli (Figure 6). Additionally, ischemic lesions were noted in the cerebellum.

(a) Axial T2 CISS sequence showing a small mass within the left internal auditory canal and (b) Axial T1 after administration of Gadolinium showing an enhancing mass of the left auditory canal compatible with a meningioma.
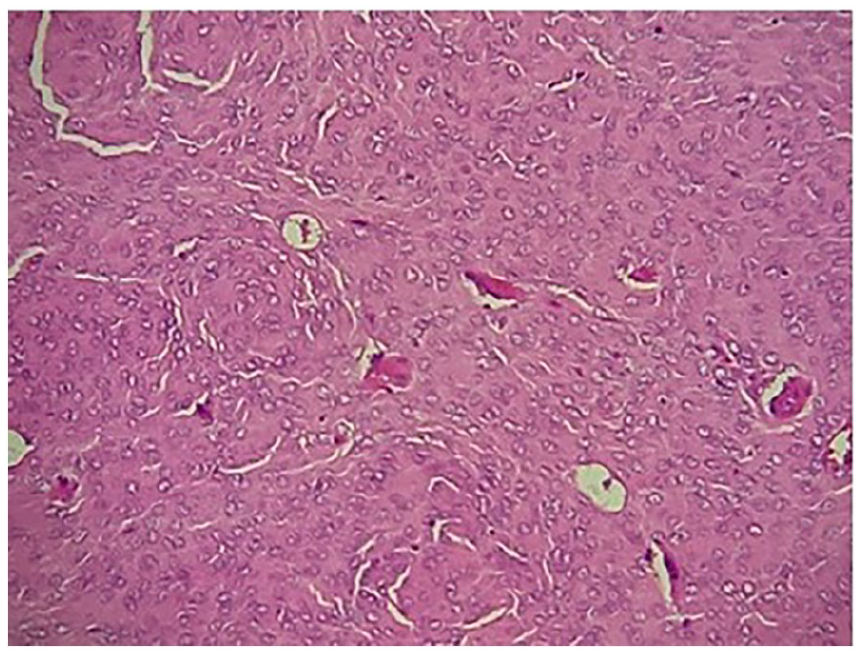
Histopathological examination showing a Meningothelial meningioma with lobulated architecture and syncytial cells with indistinct cell membranes, eosinophilic cytoplasm.

Axial brain CT scan showing: (a) large hypodense lesions of the cerebellum compatible with ischemic lesions (Blue arrow) subarachnoid hemorrhage of the right tentorium cerebelli (White arrow), (b) residual tumor with hemorrhagic changes (Blue arrow), and (c) residual tumor in the right parapharyngeal space (Blue arrow) with hemorrhagic changes (Blue star).
Discussion
Cerebellopontine angle (CPA) meningiomas originate from arachnoid villi located near structures such as the sigmoid sinus, jugular foramen, torcula, and the superior or inferior petrosal sinuses. Meningiomas are rare in the pediatric population, accounting for less than 5% of all pediatric brain tumors, with the CPA being an exceedingly uncommon location.1,2
Pediatric meningiomas exhibit distinct clinical and biological characteristics, including a rapid growth pattern, larger tumor size at diagnosis, higher rates of recurrence and malignant transformations, and poorer outcomes, particularly in children under 6 years old. Symptoms vary depending on tumor location and commonly include hearing loss, tinnitus, vertigo, headaches, balance difficulties, trigeminal nerve symptoms, and ataxia if the cerebellum is compressed. Clinical presentations may also include difficulty with chewing, swallowing, and speaking when the hypoglossal nerve is affected.2,3
Imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI) are essential for diagnosis. On CT, CPA meningiomas typically appear as hyperdense lesions with possible calcifications, bone hyperostosis, or skull base erosion. MRI findings typically show sessile, homogeneously enhancing tumors along the petrous ridge with a characteristic dural tail. Rarely, CPA meningiomas infiltrate the temporal bone, vestibule, or cochlea. Involvement of structures such as the clivus, jugular foramen, Meckel’s cave, cavernous sinus, or middle fossa strongly supports the diagnosis of meningioma. Principal Differential diagnoses include Schwannoma, paraganglioma, metastasis, and Primary bone tumors.2,3
Meningiomas involving neural foramina, venous sinuses, or adjacent structures pose significant surgical challenges. They can compromise multiple cranial nerves and have a higher risk of recurrence. Advanced imaging techniques are critical for evaluating tumor extent, cranial nerve involvement, and surgical planning, which helps minimize postoperative morbidity. 4
The Hoye classification system categorizes extracranial meningiomas based on their etiology 5 :
➢ Secondary: Extracranial extension of an intracranial meningioma.
➢ Primary: Extracranial meningioma originating in a neural foramen.
➢ Primary: Ectopic meningioma without connection to cranial nerve foramina or intracranial structures.
➢ Secondary: Extracranial metastasis from an intracranial meningioma.
Histopathologically, pediatric meningiomas more frequently exhibit atypical features, including clear cell or papillary variants, although fibrous and meningothelial types remain the most common.2,4
Surgery is the primary treatment for pediatric CPA meningiomas and is often performed aggressively. Preoperative embolization is less commonly employed in children due to smaller vascular calibers, and chemotherapy has shown limited efficacy in this population. However, radiation has been shown to improve local control and prolongs overall survival.6,7
Some studies suggest that optimal nonradical resection of large cerebellopontine angle (CPA) meningiomas achieves favorable long-term tumor control while preserving neurological function. Additionally, adjuvant Gamma Knife Surgery (GKS) is a safe and effective supplementary treatment, as it does not introduce additional morbidity. 8
Our case involves a 12-year-old boy with a posterior fossa meningioma extending to the parapharyngeal space via the hypoglossal canal. Compared to Ozdil Baskan’s case of a 54-year-old woman, which described a large posterior fossa mass extending into the sphenoid sinus and parapharyngeal space, the pediatric case is unique due to its rapid growth, and association with Neurofibromatosis Type 2 (NF2). Michel Neeff’s case of a 28-year-old man presented a parapharyngeal mass with intracranial components and aggressive surgical intervention (Table 1).3,6
Comparative Table Summarizing Our Case Alongside 2 Similar Cases, Focusing on Demographics, Tumor Extension, Cranial and Vascular Involvement, Surgical Approach, Complications, and Outcomes.

Both adult cases featured extensive tumor encasement of the internal carotid artery. In Michel Neeff’s case, the artery was occluded preoperatively, with aggressive resection sacrificing major vessels and lower cranial nerves. Postoperative recovery required extensive rehabilitation, highlighting the complexity of managing such tumors (Table 1).3,6
Our case case presents several unique aspects, including a pediatric presentation characterized by faster tumor progression and higher recurrence rates compared to adult meningiomas. Additionally, the patient has Neurofibromatosis Type 2 (NF2), which involves systemic findings such as bilateral auditory canal lesions, requiring long-term multidisciplinary care. The surgical approach is more conservative, with a focus on partial resection to preserve neurological function, in contrast to the aggressive resections typically performed in adult cases.7,8
Conclusion
Pediatric cerebellopontine angle (CPA) meningiomas with extracranial extension are rare and pose significant diagnostic and therapeutic challenges due to their complex anatomical involvement. These tumors require advanced imaging for accurate assessment of their extent and to guide surgical planning. Despite aggressive surgical intervention, the prognosis remains guarded, emphasizing the importance of early detection and a multidisciplinary approach to treatment.7,8
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.