
Abstract
The integration of global health (GH) principles into pediatric emergency medicine (PEM) is essential to addressing disparities in child health outcomes, particularly in low- and middle-income countries (LMICs), where preventable diseases remain a leading cause of mortality. This narrative review explores the intersection of PEM and GH, emphasizing the need for comprehensive training, sustainable infrastructure, and policy frameworks tailored to resource-limited settings. Key barriers, including limited critical care resources, delayed presentation, and workforce shortages, are discussed alongside the transformative potential of strategies such as telemedicine, cultural competence, and international collaboration. The review highlights successful models from both high-resource and low-resource settings, illustrating how innovative training programs, bidirectional partnerships, and equitable resource allocation can enhance pediatric emergency care globally. By advocating for capacity building, evidence-based policymaking, and integration of GH into PEM training, this review provides actionable insights to ensure resilient, inclusive, and high-quality pediatric emergency care systems worldwide.
Keywords
Introduction
The global burden of childhood emergencies remains a significant public health challenge, disproportionately affecting low- and middle-income countries (LMICs), where healthcare resources are limited, and preventable diseases contribute to high mortality rates. While pediatric emergency medicine (PEM) has achieved remarkable advancements in high-income countries, its integration with global health (GH) principles in LMICs has been slower, leaving a critical gap in addressing the unique challenges faced by children in resource-limited settings.1,2
Global health emphasizes health equity, cross-cultural understanding, and interdisciplinary approaches that transcend borders to achieve improved health outcomes worldwide. 3 These principles align seamlessly with the goals of PEM, which aims to deliver timely and life-saving interventions for critically ill or injured children. However, integrating GH concepts into PEM training and practice remains under-explored, particularly in LMICs, where barriers such as delayed presentation, financial constraints, and inadequate infrastructure impede the delivery of effective emergency care. 4
Historically, international emergency medicine (IEM) training has focused on adult care, leaving a substantial gap in pediatric-specific initiatives. Since the establishment of IEM fellowships in 1994, the field has expanded, increasing training programs from 8 in 2005 to 39 by 2012. 5 However, most of these initiatives remain adult-focused, with limited emphasis on pediatrics. Pediatric emergency medicine, recognized as a subspecialty in the early 1980s, has significantly improved child health outcomes worldwide. 6 Yet, disparities persist, with approximately 6.6 million annual child deaths—primarily in LMICs—underscoring the urgent need for targeted interventions. 7
In resource-limited settings, under-five mortality rates are alarmingly high, ranging from 180 deaths per 1000 live births in Somalia to just 5 per 1000 in the UK. 8 While childhood mortality rates have declined globally, progress has slowed in recent years, emphasizing the need for renewed focus on underserved areas. Preventable conditions such as pneumonia, diarrhea, and malaria remain the leading causes of child mortality, despite being amenable to simple, cost-effective treatments. 9
Structured PEM-GH fellowship programs, such as the first combined Pediatric Emergency Medicine–Global Health (PEM-GH) fellowship introduced in 2005, have attempted to bridge this gap. These programs equip trainees with the necessary skills to address the complexities of global pediatric emergencies effectively. 10 However, structured mentorship and training opportunities specific to global pediatric emergency care remain limited, with existing initiatives often focusing on general pediatrics rather than the unique challenges of resource-constrained settings. 11
This review examines the integration of GH principles into PEM, analyzing the current state of training programs, the impact of IEM and PEM on child health outcomes, and opportunities for further development. It highlights the importance of training physicians especially in low and middle income countries to ensure timely delivered care. This will prevent unnecessary delay of care and improve mortality. This aims are achieved by showcasing successful models and identifying training gaps, this review seeks to offer insights into preparing PEM practitioners to meet global health challenges. As healthcare systems continue to evolve, a comprehensive and integrated approach to PEM rooted in global health principles is becoming increasingly vital
Global Burden of Pediatric Emergencies
Epidemiology of Pediatric Emergencies
According to the Global Burden of Disease (GBD) study, in 2013, approximately 7.7 million children and adolescents died globally, the distribution of their ages in demonstrated in Figure 1. Among children below 5 years old; the leading causes of death were demonstrated in Figure 2. Children older than 5 years old experienced significant mortality from diarrheal diseases (38 325) deaths, while adolescents were most affected by road injuries, with 115 186 deaths in 2013. 12
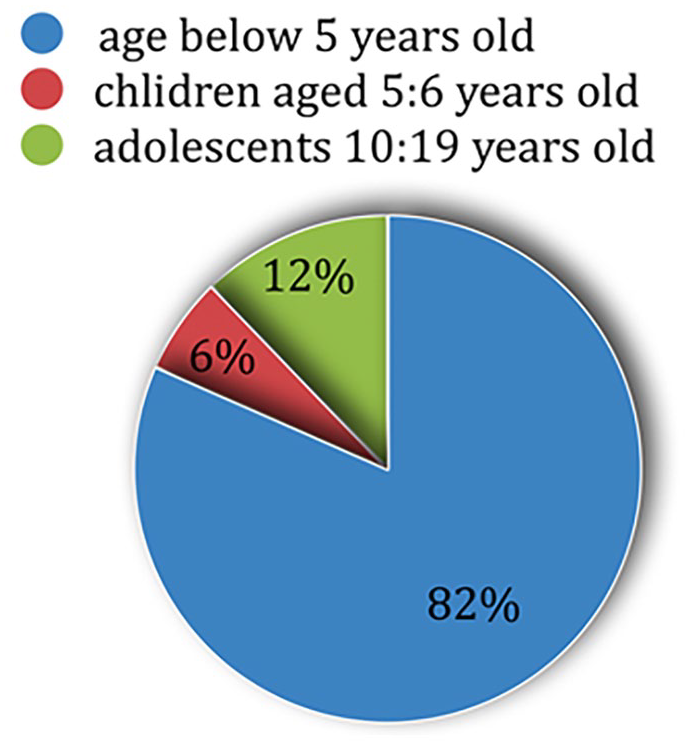
Age distribution of pediatric mortality in 2013. 12
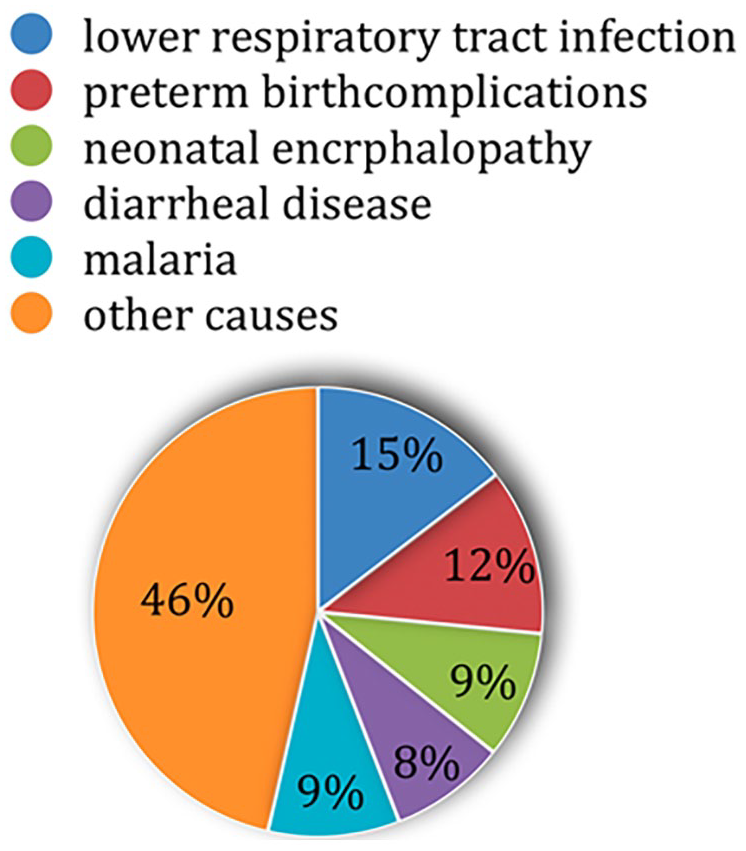
Leading causes of pediatric mortality. 12
Globally, sub-Saharan Africa bore a disproportionate burden, particularly for malaria, which caused 90% of its global deaths. Nigeria accounted for 38% of worldwide malaria deaths and 12% of global deaths from lower respiratory tract infections. Similarly, diarrheal diseases among children and adolescents were concentrated in 5 countries—India, the Democratic Republic of Congo, Pakistan, Nigeria, and Ethiopia—which together accounted for 50% of global deaths from these illnesses. In developed nations, lower respiratory infections and diarrheal illnesses were less prominent causes of death, with preterm birth complications and congenital anomalies contributing more significantly due to improved infectious disease control but continued neonatal health challenges. 12
In terms of morbidity, adolescents (10-19 years) accounted for nearly 60% of the 135.6 million years lived with disability (YLDs) among children and adolescents. Iron deficiency anemia emerged as the leading cause of disability, affecting 619 million children and adolescents globally. These figures underscore significant regional disparities. It highlights the need for targeted interventions to address both mortality and disability, particularly in developing nations where preventable deaths and disabilities remain disproportionately high. 12
Challenges in Resource-Limited Settings
Limited Access to Resources
In low-resource settings, providing effective pediatric emergency care is severely hindered by a lack of critical resources. Approximately 11.9 million children aged 0 to 14 die annually, with 95% of these deaths occurring in low and middle income countries. 13 Up to 70% of these deaths—primarily from treatable conditions. For example; acute respiratory infections, diarrheal diseases, neonatal infections, and malaria—could be prevented with adequate critical care infrastructure. 13 However, essential resources such as equipment, medications, and skilled healthcare professionals are often unavailable or insufficient in these regions.
Delayed Presentation and Severity on Arrival
Children in low and middle income countries often present for care only after symptoms persist for more than 24 hours. This delay significantly worsening the severity of illnesses upon arrival. 14 It is compounded by systemic barriers, including malnutrition, unvaccinated statuses, and long travel distances to healthcare facilities. For example, neonatal sepsis and birth asphyxia, common in these settings, require immediate intervention, which is frequently delayed due to the absence of effective triage systems. 6
Financial Barriers and Ethical Decisions
Financial constraints remain a significant impediment to accessing pediatric emergency care. Many low and middle income countries families live on less than $1 per day, making critical care interventions unattainable without catastrophic financial consequences. 15 Pediatric intensive care physicians in such settings often face ethical dilemmas, prioritizing conditions with favorable recovery prospects (eg, treatable malaria or tetanus) over those with poor prognoses (eg, hypoxic-ischemic encephalopathy or fulminant liver failure). 15
Lack of Trained Personnel and Infrastructure
Severe shortages of trained pediatric emergency personnel exacerbate challenges in low and middle income countries. Many ICUs lack pediatric-focused training for doctors and nurses, leading to suboptimal care. Furthermore, critical care units often lack basic equipment such as ventilators or oxygen concentrators. Even when this equipment are available, staff are not always adequately trained to use them. 15
Inadequate Diagnostic and Monitoring Tools
Resource limitations extend to diagnostic capabilities. Advanced imaging technologies and laboratory tests common in high-resource settings are rare in low and middle income countries. Clinical decisions often rely on physical examinations rather than diagnostic data, increasing the likelihood of delays or mismanagement in critical cases. 16
These barriers are more prominent in resource limited settings than resource rich settings which entails the importance of tailoring delivered care to the setting it’s provided to, as demonstrated in Table 1.
Challenges in Pediatric Emergency Medicine Across Resource Settings.

Importance of Global Health in Pediatric Emergency Medicine
Global health is a discipline that prioritizes equity in healthcare and addresses shared health issues requiring interdisciplinary actions that transcend national borders. 17 Its principles are especially pertinent in the context of pediatric emergency medicine (PEM), where disparities in child health outcomes demand urgent attention.
Diseases such as COVID-19 have demonstrated how health challenges easily cross geographical boundaries. 18 Healthcare professionals now frequently encounter children from diverse cultures, including immigrants, refugees, and international adoptees. Additionally, children traveling abroad are exposed to communicable and non-communicable diseases prevalent in other countries, further reinforcing the interconnectedness of global health.
To understand the importance of global health, it is essential to address 3 key components:
1. Diverse Health Needs: The health challenges faced by children globally vary significantly, requiring context-specific interventions.
2. Health Equity: Ensuring fair access to healthcare and minimizing disparities across regions.
3. Cultural Competence: Developing the ability to communicate and provide care effectively to patients from varied sociocultural backgrounds.
Impact on Patient Care
Improved Outcomes in Resource-Rich Settings
The incorporation of global health principles into pediatric emergency training has a transformative impact, equipping clinicians with a broader understanding of healthcare systems and diverse health challenges worldwide. Exposure to varied healthcare environments, such as tropical medicine and conditions unfamiliar to Western practitioners, significantly enhances residents’ diagnostic and management skills. Programs like the International Health Program (IHP) illustrate this transformation. According to Dr. Michele Barry, IHP participants return “more sober about health costs, more careful about laboratory utilization, and with greater understanding of cultural differences,” emphasizing the program’s role in shaping cost-effective, culturally aware practitioners.
Training in global health concepts also promotes culturally competent care, improving patient satisfaction and overall experiences. Clinicians trained in cultural competence are better equipped to understand patients as individuals with unique beliefs and values. This fosters effective rapport-building and ensures personalized care plans that address diverse cultural backgrounds. A patient-centered approach, when combined with cultural competence, reduces misunderstandings, builds trust, and promotes equitable care for marginalized populations. Training programs embedding these principles enable clinicians to meet diverse patient needs while improving outcomes and equity in care delivery.
Enhancing Care in Resource-Limited Settings
The integration of global health principles into pediatric emergency care enhances healthcare delivery in resource-limited settings through knowledge transfer and capacity building. Initiatives like the Project of Extension for Community Health Care Outcomes (ECHO) exemplify bidirectional learning, where local providers benefit from the expertise of academic medical centers while sharing valuable on-the-ground insights. This model empowers community emergency departments with evidence-based strategies, fostering improved patient outcomes.
Long-term effectiveness requires sustainable systems. Partnerships between stakeholders, as highlighted by Eckerle et al, illustrate the impact of collaborative efforts in Malawi. By providing acute care expertise, training programs, and investments in research and clinical efforts, these partnerships have reduced pediatric mortality at Kamuzu Central Hospital. The focus on local capacity-building ensures that the benefits of these initiatives extend beyond immediate outcomes, fostering resilience and long-term improvements in healthcare systems.
Curriculum Development for Global Health Integration
Medical education has always been focusing on disease and treatment to the near exclusion of the social and behavioral factors that cause disease or affect the management. That highlights the importance of generating an educational system capable of teaching the physicians how to integrate their knowledge with the population culture to provide the ultimate care with the skills needed for that like asking questions to elicit full understanding, developing different forms of communication styles and negotiation mechanisms, skills of assessing decision making as well as tools to recognize sexuality and gender issues. 18
There has been a great interest in applying global health education and this can be implemented on different levels of education. Starting from medical school to all levels of medical education including the curricula and using E-learning to expand knowledge and access healthcare providers around the world. 19 Other concepts that could be implied is medical anthropology, understanding needs of society, and Holism,inclusion of the whole, which goes beyond that to why people behave the way they do and what influences them. 20
Simulations is another powerful tool that can be applied in such a field to provide case-based scenarios in controlled settings that put the participants under similar circumstances of stresses and emotions they might encounter in real life scenarios. Thus, enabling the learners to build emotional intelligence and their ways of critical thinking and problem-solving skills that would enable them eventually to deal with different difficult scenarios in the real world, especially ethical dilemmas in different cultures. 21
Cultural Competency in Pediatric Emergency Care
While the definition of culture is vague, most define it as the shared beliefs, values, and knowledge of a certain social group. Culture has a significant impact on the definition of health, which varies between different cultural groups. 22 the major steps to achieve cultural competency are demonstrated in Figure 3. Some examples of the training models are listed in Table 2.

Major steps to achieve cultural competency in pediatric emergency care.
Global Pediatric Emergency Medicine Training Models.

International Collaboration and Partnerships
Equitable and mutually beneficial partnerships are key for the development of pediatric global health programs, which, in the long term, can ensure a healthy future generation. 33 Global health electives and exchanges are impactful examples of such partnerships and have been universally shown to positively contribute to advancing global health and pediatric emergency care. Unidirectional global health rotations typically entail the travel of students from high- to limited-resourced settings. 33 Students participating in global health electives have reported developments in their knowledge of global health, burden of disease, differences in health care systems, and in their understanding of international health. 34
Concerns have emerged over potential exploitation in global health rotations involving the travel from high income countries (HICs) to low and middle-income countries (LMICs), as inequities in LMICs stem from colonial histories. Moreover, travelers from HICs might lack an understanding the local cultural and socioeconomic environment. 35 On the other hand, bidirectional global health exchanges also offer similar benefits to those of global health electives. However, bidirectional exchanges support the 2 participating institutions learning from each other, rather than one institution being relied on as the teaching institution. 36 A prominent example of a successful bidirectional global health exchange program is that between University Teaching Hospitals (UTH) of Lusaka, Zambia and the University of Maryland, Baltimore (UMB). By offering pre-departure and onsite training for UMB trainees, they have addressed some concerns of global health electives. 37 Another example of a successful global health exchange is a virtual exchange between students at Stanford University in the US, and Modern University of Business & Science in Lebanon, using an online platform. 38
Collaborative research initiatives further solidify international partnerships by addressing pressing global pediatric emergency issues. They aim to bring together diverse perspectives, and advance pediatric emergency healthcare. 39 High-quality research on global pediatric emergency issues provides updated information for healthcare workers on various patient presentations, patient volume, and serious outcomes. Nationally and regionally focused research networks have overcome numerous challenges in the areas they serve. However, certain research gaps persisted, along with an expanding need for implementing published evidence. 40 One prominent global research initiative is the Pediatric Emergency Research Network (PERN). Founded in October 2009, the initiative initially included 5 pediatric emergency research networks from the United States, Canada, Australia, New Zealand, Europe, and the Middle East. PERN has supported the formation of a further 3 pediatric emergency research networks in Europe and Latin America and has led to the recognition and establishment of pediatric emergency as a subspecialty in some countries. 41
Data-sharing platforms complement the progress made by pediatric emergency research initiatives and facilitate further research efforts. Data-sharing platforms, or registries, organize, and preserve data and are hosted on platforms enabling interactions between the platforms and the researchers. Deidentified patient data, drawn from patient electronic health records (EHRs), are valuable for conducting research in pediatric emergency care, and drawing conclusions based on analyzed trends. 42 Sharing individual participant data from clinical trials also improves transparency and allows for data reuse in future studies. Data-sharing platforms are particularly valuable in pediatric research, due to the potential ethical, regulatory, and financial challenges of conducting pediatric clinical trials. 43 Notable data-sharing platforms include the Pediatric Emergency Care Applied Research Network (PECARN) Registry, the Swiss PedData Project, the National Institute of Health (NIH), and the TriNetX Platform. 44
In many resource-limited countries, primary health care facilities are often the first point of contact for patients seeking care. However, these facilities experience numerous barriers, including limited resources, lack of knowledge of emergency healthcare, and delay in referral to other levels of care. 45 Moreover, in countries with established emergency departments, pediatric mortality rates were significantly higher than adult mortality rates (4.8% vs 0.7%). 46 Training in pediatric emergency care, in addition to the establishment of emergency departments, are key for addressing this issue. Capacity building has been shown to be beneficial even for non-emergency healthcare workers. Training of healthcare workers in primary care centers on the management of pediatric emergencies has been shown to improve outcomes. 51 Online platforms are also potentially valuable tools for capacity building. The WHO advocates the use of digital learning in emergencies capacity building, due to its success during the Covid-19 pandemic, in addition, it utilizes case studies. 47 Other initiatives, such as Emergency Capacity Building Project (ECBP), have successfully implemented a mixed-methods approach, using a combination of simulations, open discussions, and periodic evaluations. As a result, the ECBP has successfully conducted training on emergency care during disasters in 5 different areas. 48
Efficient emergency medicine care in a hospital can have profound effects on emergency department outcomes, including minimized triage times. 49 Efficient emergency care systems must be accessible, provide essential medicines, ensure equitable distribution of goods and services, and adopt and implement national public health strategy. 50 Establishing emergency medical services (EMS) in LMICs is a challenge, and requires requiring solutions adapted to a country’s conditions and local demands. Needs assessments are also important for assessing the country’s strengths and weaknesses in healthcare. Creating efficient EMS in LMICs can be achieved through interdisciplinary collaboration, involving government officials, policymakers, and the existing healthcare system. 51
Impact on Patient Care
Improved Outcomes in Resource-Rich Settings
The incorporation of global health concepts into pediatric emergency training offers a transformative effect by equipping clinicians with a cross-cultural understanding of health care systems and a widened perspective on health challenges worldwide. Exposure of medical residents to a wide variety of healthcare environments, tropical medicine, and the management of conditions unfamiliar to Western practitioners enhances the residents’ clinical diagnostic skills. Such aims are achieved by programs as the International Health Program (IHP). Eckerle et al 52 states that participants in the IHP return “more sober about health costs, more careful about laboratory utilization, and with more understanding of cultural differences,” emphasizing the program’s role in shaping thoughtful, cost-effective practitioners. Exposing clinicians to international health enables them to manage a diverse range of cases effectively and to adapt their practice to a variety of patient populations as their exposure to international health fosters adaptability, cultural sensitivity, and humanistic qualities. 52
The integration of international health into pediatric emergency medicine training also improves patient satisfaction by promoting culturally competent care, which is crucial for improving the overall patient experience. Clinicians with cultural competence are better equipped to visualize patients as unique individuals, establish effective rapport, and consider their personal beliefs and values that influence patients’ understanding and views on illness and treatment. By embracing a patient-centered approach that goes hand in hand with cultural competence principles, healthcare providers are more likely to be able to tailor care plans that take into consideration the diverse cultural backgrounds, minimizing misunderstandings, and building trust. This approach not only improves the quality of care but also promotes equity by ensuring the delivery of personalized and fair treatment for disadvantaged populations. Prioritizing comfort, effective communication, and shared decision which occurs as a result of the integration of patient-centeredness and cultural competence contribute to a more positive healthcare experience and an improved overall patient satisfaction. Training programs that embed global health principles equip clinicians to meet the needs of diverse patient populations while promoting improved outcomes and equity in care. 53
Enhancing Care in Resource-Limited Settings
By facilitating knowledge transfer, the application of global health concepts into pediatric emergency medicine can remarkably enhance care in resource-limited settings. Programs like Project of Extension for Community Health Care Outcomes (ECHO) have proven the value of bidirectional learning, allowing community emergency departments (CEDs) to access specialized knowledge from academic medical centers (AMCs). This approach improves the implementation of pediatric emergency care strategies, providing local providers with best practices to ensure the delivery of better patient outcomes. 54
Establishing systems that can maintain long-term effectiveness is integral for achieving sustainable improvements in pediatric emergency care. Initiatives should concentrate on building local capacity through the implementation of social determinants of health interventions and the development of partnerships to enhance pediatric care. For instance, Eckerle et al 52 highlighted that the development of a novel partnership between relevant stakeholders in Malawi and US-based partners with expertise in pediatrics emergency medicine (PEM) should be of aid to further reduce pediatric mortality. This partnership focuses on the collaborative provision of acute care expertise, training, as well as investments in the development of educational, research, and clinical efforts in pediatrics emergency medicine (PEM) at Kamuzu Central Hospital. Such initiatives ensure not only that improvements are immediate but are also enduring, supporting long lasting enhancements in healthcare systems and ensuring resilience and continuity in resource-constrained settings. 54
Case Studies From Low-Resource Countries
Emergency Care Development in Tanzania
Tanzania has historically faced high child mortality rates due to limited emergency medical services and inadequate infrastructure. Addressing these challenges has involved collaborations between local hospitals and international organizations to establish pediatric emergency units and train healthcare workers. The Child Nursing Practice Development Initiative (CNPDI) at the University of Cape Town is one such program that has boosted local capacities. Through partnerships with hospitals across sub-Saharan Africa, the program has successfully trained pediatric and critical care specialists, developed training hubs in Malawi and Tanzania, and laid the groundwork for comprehensive pediatric emergency services.
The impact has been transformative, with reductions in pediatric mortality and strengthened tertiary care facilities. These partnerships underscore the importance of sustained international support and workforce development for addressing healthcare disparities in low-resource settings.
Pediatric Emergency Training Programs in Nepal
Nepal’s under-5 child mortality rate of 39 deaths per 1000 live births reflects significant gaps in pediatric emergency care. The absence of residency programs and limited emergency health service providers contribute to the high mortality rates. Establishing emergency medicine residency programs within the country could train a new generation of specialists, equipping them to manage critical conditions effectively. Comprehensive training and certification programs are essential for building sustainable healthcare systems aligned with global best practices. By investing in local training initiatives, Nepal can improve pediatric outcomes and elevate healthcare standards nationwide. 55
Telemedicine Initiatives in Sub-Saharan Africa
Healthcare access, particularly specialized care, remains a significant challenge in sub-Saharan Africa. According to the 2006 World Health Report, Africa accounts for 24% of the global disease burden but only 3% of the healthcare workforce and less than 1% of global health spending. Compounding the issue, 43% of the population lives on less than US$1 per day, and rural areas, where 60% of the population resides, face the greatest healthcare access disparities. Additionally, the population’s median age of 18 years and rapid growth outpace the rate of healthcare workforce expansion, further straining the already fragile system. 56
Telemedicine has emerged as a transformative solution to these challenges. By enabling remote consultations between local healthcare providers and global specialists, telemedicine addresses critical workforce shortages and ensures timely care for underserved populations. This technology eliminates the need for patients to travel long distances for specialized care, provides ongoing support for rural providers, and facilitates medical education. It also strengthens research efforts by making expert resources readily accessible, ultimately improving healthcare delivery and quality. 57
A prominent example is the Pediatric Telemedicine Connecting Hospitals (Peds-TECH) program. Developed in Ontario, this initiative connects a community hospital with a tertiary care pediatric hospital using real-time audio-visual communication. The program has proven invaluable, particularly in facilitating telemedicine-based resuscitations for critically ill pediatric patients. Parents and caregivers have expressed gratitude for the reassurance and rapid specialist intervention enabled by Peds-TECH. By providing visualization tools crucial for assessing pediatric conditions and enabling immediate connection to specialized care, this model significantly enhances communication and care quality. 58
Some examples of successful low income countries pediatric emergency medicine initiatives is listed in Table 3.

Resource Constraints and Ethical Considerations
Resource Constraints
Financial Limitations
Pediatric emergency care in low- and middle-income countries (LMICs) faces severe funding challenges. Limited resources for essential medical supplies, diagnostic tools, and workforce recruitment hinder effective care. Furthermore, underfunded training programs lead to suboptimal clinical protocol implementation. Partnerships between governments, private sectors, and international organizations are crucial for sustainable financial models. 67
Infrastructure Deficits
The lack of well-equipped emergency departments and intensive care units (ICUs) compromises pediatric emergency care. Basic tools such as ventilators, defibrillators, and blood gas analyzers are often unavailable, delaying care and worsening outcomes. Addressing these gaps requires cost-effective solutions like modular emergency units and mobile clinics. Strategic investment in infrastructure development can substantially improve healthcare delivery. 68
Ethical Considerations
Cultural Sensitivity
Cultural practices and beliefs often conflict with medical protocols, creating ethical dilemmas for healthcare providers. For instance, parental refusal of treatments like blood transfusions due to religious beliefs complicates decision-making. Training healthcare workers to navigate these scenarios respectfully and adopting patient-centered approaches can help bridge cultural divides. 69
Volunteerism Risks
International volunteer programs risk undermining local healthcare systems if not well-coordinated. Temporary solutions from foreign volunteers may lead to inefficiencies and dependency. Effective volunteer programs must focus on strengthening local capacities through training and collaboration. 70
Sustainability Issues
Dependency Risks
Excessive reliance on external funding and expertise threatens program sustainability. Many initiatives collapse once donor support ends. Building local ownership through workforce training and infrastructure investment is key to creating self-sustaining systems. 71
Staff Retention
The emigration of skilled healthcare professionals, or “brain drain,” exacerbates staff shortages in LMICs. Policies offering competitive salaries, professional development opportunities, and safe work environments are essential to retaining talent locally. 72
Strategies for Effective Implementation
Policy and Advocacy
Government policies that prioritize pediatric health in national strategies are vital for sustainable programs. Aligning initiatives with global frameworks like the Sustainable Development Goals (SDGs) attracts funding and facilitates international collaboration. Early engagement with policymakers ensures integrated resource allocation and infrastructure development. 73
Funding and Resource Allocation
Grants and Donations
International grants, public-private partnerships, and innovative models like crowdfunding can provide essential financial support. These funds should be directed toward improving infrastructure, training programs, and medical supply chains. 74
Efficient Resource Use
Task-shifting, mobile clinics, and telemedicine maximize resource efficiency in underserved regions. Streamlining procurement processes and reducing waste further optimize healthcare delivery. 74
Monitoring and Evaluation
Performance Indicators
Metrics such as patient response times, morbidity rates, and care accessibility provide critical insights into program success. Continuous monitoring enables healthcare systems to adapt and improve based on observed trends. 75
Feedback Mechanisms
Involving healthcare workers, patients, and community members in regular feedback loops promotes adaptive learning. Surveys, focus groups, and staff meetings can identify strengths and areas for improvement, ensuring program relevance and effectiveness 76
Future Considerations
1. Expanding Specialized Training Programs Establishing Pediatric Emergency Medicine-Global Health (PEM-GH) fellowship programs and incorporating global health curricula into medical education are critical steps toward addressing disparities in pediatric emergency care. These programs should emphasize cultural competence, ethics, and the unique challenges of resource-limited settings. Additionally, expanding opportunities for healthcare providers to engage in hands-on training through simulations and fieldwork ensures that theoretical knowledge translates into practical expertise. Partnerships with international organizations, such as WHO and UNICEF, can support these training programs with resources and expertise. 77
2. Strengthening Global Partnerships International collaborations should focus on fostering equitable and sustainable partnerships. Programs like the Pediatric Emergency Research Network (PERN) and Project ECHO exemplify how knowledge exchange and capacity-building initiatives can strengthen healthcare systems worldwide. A global network dedicated to pediatric emergency care would streamline communication and ensure uniform care standards globally. Additionally, fostering bidirectional exchanges between low- and high-resource settings encourages mutual learning, enabling countries to adopt the most effective practices. 78
3. Leveraging Technology Technological advancements such as telemedicine, e-learning platforms, and artificial intelligence (AI) hold immense potential to bridge healthcare gaps in remote and underserved regions. For example, telemedicine can provide real-time guidance to local providers, while AI-driven tools can enhance diagnostic accuracy and patient management. E-learning platforms enable healthcare professionals to access high-quality educational resources regardless of their location. Governments and healthcare institutions should integrate these technologies into their systems to improve outcomes and ensure accessibility. 79
4. Focus on Research and Data Sharing Increased investment in pediatric emergency care research, along with the development of robust data-sharing platforms, is essential for advancing evidence-based practices. Initiatives like the Pediatric Emergency Care Applied Research Network (PECARN) Registry and TriNetX facilitate data analysis and trend identification, enabling the development of targeted interventions. Such platforms also promote transparency and encourage collaboration among researchers globally. Prioritizing research funding and establishing cross-border data-sharing agreements can further strengthen these efforts. 80
Conclusion
The integration of global health concepts into pediatric emergency medicine is a crucial step toward addressing disparities in child health outcomes worldwide. This effort arises from the significant burden of pediatric emergencies, the lack of specialized healthcare settings, and inadequate infrastructure in both high-resource and low-resource settings.
This comprehensive review underscores the importance of merging pediatric emergency medicine and global health concepts to ensure equitable and effective care for vulnerable populations. The critical need for specialized training, sustainable infrastructure, and cultural competence is evident, as these factors collectively improve care delivery in diverse settings. By fostering cultural sensitivity, promoting equitable access, and building resilient healthcare systems, Pediatric Emergency Medicine (PEM) practitioners can significantly enhance patient outcomes and satisfaction.
International collaboration and bidirectional partnerships have demonstrated success in advancing pediatric emergency care globally. However, achieving these outcomes requires active government engagement, sustainable financial support, and continuous performance assessment based on standardized indicators. The challenges, particularly in low- and middle-income countries, necessitate multi-sectoral efforts to ensure that every child—regardless of location, ethnicity, or socio-economic status—receives timely and high-quality emergency care.
By emphasizing the importance of technology, research, and global collaboration, this review advocates for a unified approach to improving pediatric emergency care. The continued integration of global health concepts into training and practice will not only address current disparities but also pave the way for a healthier, more equitable future for children worldwide.
Footnotes
Abbreviations
● AI: Artificial Intelligence ● AMC: Academic Medical Center ● CED: Community Emergency Department ● COVID-19: Coronavirus Disease 2019 ● DALYs: Disability-Adjusted Life Years ● ECHO: Extension for Community Healthcare Outcomes ● EHR: Electronic Health Record ● HIC: High-Income Country ● ICU: Intensive Care Unit ● IHE: International Health Elective ● LMICs: Low- and Middle-Income Countries ● PEM: Pediatric Emergency Medicine ● PEM-GH: Pediatric Emergency Medicine-Global Health ● PECARN: Pediatric Emergency Care Applied Research Network ● PERN: Pediatric Emergency Research Network ● SDGs: Sustainable Development Goals ● WHO: World Health Organization.
Authors’ Note
I declare that the work presented in this manus is original and hasn’t been submitted, in whole or in part, for publication elsewhere.
Author Contributions
All authors have contributed significantly to the conception, design, execution, and interpretation of the work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset supporting the conclusions of this article is included within the article.