
Abstract
Introduction:
The global neonatal death rate was predicted to be 18 per 1000 live births during the first 28 days of life. Ethiopia continues to have one of the highest neonatal mortality rates in the world. Essentially, over 70% of these deaths may have been averted or prevented if proper essential newborn care had been provided. The purpose of this study was to assess the practice of essential newborn care and associated factors among obstetric care providers in public hospitals in Sidama regional state, Ethiopia.
Methods:
This study was conducted from 1 to 30 July 2020, using an institutionally based cross-sectional study design. The study comprised 182 obstetric care professionals from six hospitals chosen at random. EpiData (version 3.1) was used to enter data, which was then exported to SPSS (version 20). Descriptive, bivariable, and multivariable logistic regression were used. Statistical significance of the explanatory variables was declared at p values <0.05.
Results:
The overall prevalence of good practice on essential newborn care was 56.6% (95% confidence interval = 49.4–63.7). Working in the delivery room (adjusted odds ratio = 3.53, 95% confidence interval = 2.04–10.06), having training in essential newborn care (adjusted odds ratio = 3.65, 95% confidence interval = 1.63–8.17), and access to established essential newborn care protocols (adjusted odds ratio = 6.88, 95% confidence interval = 3.10–15.26) were found to be statistically significant factors of essential newborn care practice.
Conclusion:
The study found that having necessary newborn care standards, being interested in working in the delivery room, and having essential newborn care training are all important factors in implementing essential newborn care practices. Important knowledge gaps were noted in key areas of essential newborn care.
Introduction
Essential newborn care (ENC) is comprehensive basic care provided to all neonates immediately after birth by skilled health personnel in order to improve their survival and well-being. It is a series of events that begin with the delivery of a baby on the mother’s abdomen, followed by drying the infant with a clean towel/cloth (wipe eyes, face, head, trunk, arms, and legs thoroughly while drying, assuring breathing), covering the baby with a dry clean cloth, and initiating early breastfeeding, cord care (delayed cord clamping for at least 2–3 min), eye care, 4% chlorhexidine gel on the cord, vitamin K supplementation, wrist/ankle identifying bands, and weighing the baby. 1
The global neonatal death rate was predicted to be 18 per 1000 live births during the first 28 days of life. Essentially, over 70% of these deaths may have been averted or prevented if proper ENC had been provided.1–5
Low-income countries have been observed to have a low coverage of ENC practices. According to a Nepalese study, 58% of newborns were dried, 60% were wrapped, and 25% were bathed on the first day of life, while 64% were breastfed within 1 h. Low implementation of ENC practices, together with other socio-demographic factors, has been recognized as a main cause of newborn mortality in Sub-Saharan Africa. According to a study conducted in rural southern Tanzania, 41% of home-born newborns were dried and 28% were wrapped within 5 min of birth, whereas just 19% were bathed after 6 h.2–4
Despite various government initiatives, such as working in collaboration with the World Health Organization (WHO) as reflected in the Health Sector Development Program IV (HSDP IV) and the Health Sector Transformation Program (HSTP) to improve the quality of ENC in health facilities, Ethiopia continues to have one of the highest neonatal mortality rates in the world. 5 Although newborn mortality has been decreasing for decades, it has recently increased somewhat, rising from 29 to 33 per 1000 live births.5,6
ENC practice was determined to be one of the determinants of neonatal death, which was shown to be 35.5 per 1000 live births in a Jimma, Ethiopia study. 7 Furthermore, newborn death was reported to be 41 per 1000 live births in a study on neonatal survival and predictors of mortality conducted in Sidama, Ethiopia, and ENC was found to be a significant predictor of neonatal survival. 8
The causes of neonatal death are almost consistent across all studies, with the majority of early neonatal fatalities preventable or treatable with simple, low-cost treatments. As a result, timely ENC is critical for a smooth transition from intrauterine to extrauterine function and for lowering neonatal mortality.1,2,7,8
In the Sidama region of Ethiopia, however, the status of obstetric care providers’ practice regarding ENC is uncertain. 8 As a result, we found it is necessary to evaluate obstetric care providers’ newborn care practices and provide comments and recommendations for improvement.
Methods
Study area and period
The Sidama region is an Ethiopian regional state that was founded on 18 June 2020, from the Southern Nations, Nationalities, and Peoples’ Region (SNNPR) and the Sidama Zone transition in 2019.
The Oromia Region is bounded on the south by Sidama (save for a short stretch in the middle where it shares a boundary with the Gedeo zone), on the west by the Bilate River (which separates it from the Wolayita zone), and on the north and east by the Oromia Region. Hawassa, located 273 kilometers south of Addis Ababa, is the current capital of both Sidama and SNNPR. In 2017, the population of Sidama was estimated to be around 3.2 million people who spoke the Cushitic language Sidama. The region has 5 town administrative and 31 woredas. It has 1 comprehensive specialized referral hospital, 4 general hospitals, 13 primary hospitals, 134 health centers, and 524 health posts. The total population in the Sidama regional state is 4,369,214. Among total population, 2,201,313 were females. There were 266 midwives, 14 nurses, 28 Integrated Emergency Surgery and Obstetrics (IESO), 10 health officers, 30 general practitioners, and 16 gynecologists, that is, a total of 364 obstetrics health care providers. The study was conducted from 1 to 30 July 2020.9,10
Study design
Institution-based cross-sectional study design was carried out.
Population
Source population
The source population comprised all obstetric care providers in public hospitals of Sidama regional state.
Study population
The study population comprised all obstetric care providers in public hospitals of Sidama regional state who were assigned at delivery ward, and provide ENC.
Inclusion and exclusion criteria
Inclusion criteria
All health professionals who were working in labor, delivery, and immediate postnatal unit in public health facilities at the time of data collection were included in the study.
Exclusion criteria
All health professionals who did not volunteer to participate in the study and were not involved in labor, delivery, or immediate postnatal care at the time of data collection were excluded.
Sample size determination and procedure
Single population proportion formula was used to calculate the sample size by considering the value of p-73%, confidence interval (CI) of 95%, and margin error of 5%.
11
Hence, p-73%, CI = 95%, d = 5%,
The number of obstetric health care providers in the selected hospitals was less than 191. So, 182 study participants were included by non-probability convenience methods.
Sampling technique and procedure
There are 18 hospitals in the study area. Six hospitals were randomly selected to maximize the representativeness of the data: Leku Primary Hospital (LPH), Adare General Hospital (AGH), Tula Primary Hospital (TPH), Yirgalem General Hospital (YGH), Bona General Hospital (BGH), and Aleta Wondo Primary Hospital (AWPH). However, the number of obstetric health care providers in the selected hospitals was less than required or calculated sample size. So, 182 study participants were included by non-probability convenience methods.
Variable of the study
Dependent variable
Dependent variables include ENC practice and knowledge of ENC.
Independent variable
Socio-demographic characteristics include age, sex, marital status, ethnicity, religion, qualification, work experience, and salary.
Personal and facility characteristics include interest to work in delivery room ward, having training, work overload, availability of guidelines, and drug and equipment supply.
Operational definition
Obstetric care provider: Health care professional who provide ENC.
Manageable workload: When the ratio of obstetric care provider to client is less than one.
Knowledge-level ENC: Fourteen knowledge items were employed to assess the ENC, and the mean score was considered to differentiate between participants with good and poor knowledge. Those who score less or equal to mean were considered as having poor knowledge, while those who score greater than mean were considered as having good knowledge. 11
Practice of ENC: Fourteen practice items of observational checklist were employed to assess the ENC practice. Those who score greater or equal to 70% of the procedure were considered as good practice. Those who score less than 70% of the procedure were considered as poor practice.11,12
Data collection tool and procedure
Structured self-administered questionnaire was used to collect the data from the study participants. Observational checklist was used to collect the practical part. Questionnaire was designed in English adapted from Ethiopian Federal Ministry of Health newborn care training participant’s 13 and after reviewing of different literature, peer reviewed article, different published article.4,12,14,15 Despite our best attempts to minimize it, such as interacting confidentially with participants and focusing on word selections from the beginning of the questionnaire construction, social desirability bias was identified as a study flaw despite our best efforts to mitigate it. The data collectors were also recruited from neighbor region to minimize social desirability bias. Six degree midwives (BSc) were selected and trained on data collection, and two degree public health officers (BSc) were selected as supervisors.
Data quality control
Detailed discussion and training of the data collector and pre-test were carried out before actual data collection. The pilot test was done on 10 health professionals who were working in labor, delivery, and immediate postnatal unit in Bansa General Hospital, one of the public hospitals in the region at the time of data collection. Their compositions were two obstetricians, two 3-degree midwives (BSc), three diploma midwives, one general practitioner, and two degree nurses (BSc). Close supervision of the data collector was being undertaken by the supervisors. Data were checked, cleaned for completeness, and accuracy.
Statistical analysis
Data were checked, cleaned for completeness, accuracy, and coded. The data were entered into statistical software EpiData (version 3.1); then, analysis was made with SPSS (version 20) after exporting the prepared data. Descriptive statistics such as frequency distribution and measure of central tendency and variability (mean and standard deviation) were computed to describe variables of the study. Those variables with p < 0.25 in bivariable analysis were considered for multivariable logistic regression analysis variables. 16 Screened variables were fitted to the multivariable logistic regression model through a backward stepwise method to reduce the effects of confounders and to identify the independent effects of each variable on the outcome variable. Finally, adjusted odds ratios (AORs) with 95% CI were employed to declare statistical significance at p value of <0.05.
Results
Socio-demographic characteristics of the study participants
A total of 182 health care providers took part in the study. The respondents’ mean age was 32 years, with a standard deviation of 5.26 years. Of the respondents, 95 (52.2%) were men (Table 1).
Socio-demographic characteristics of obstetric care providers who participated in the study, Sidama, Ethiopia, 2020 (N = 182).
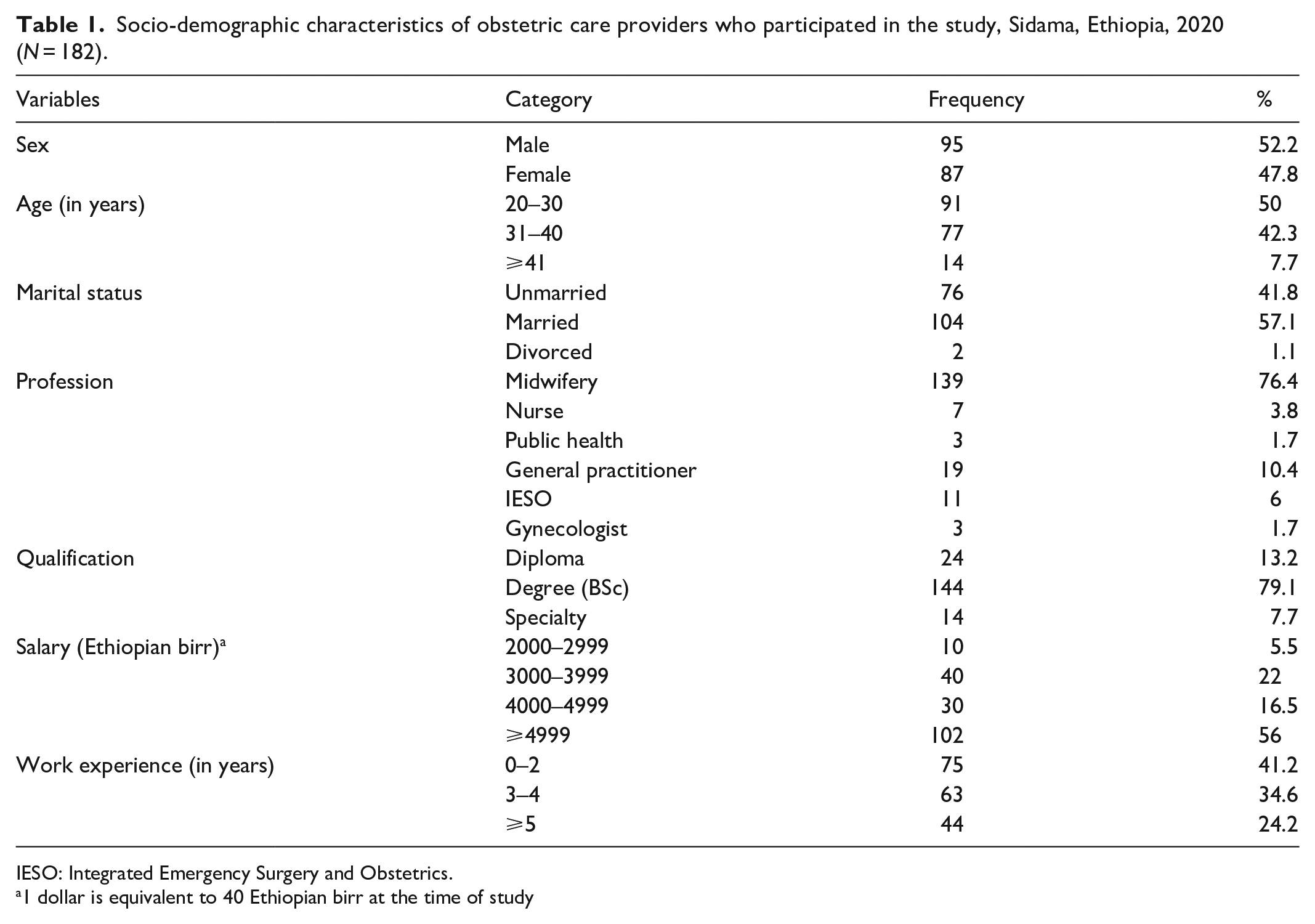
IESO: Integrated Emergency Surgery and Obstetrics.
1 dollar is equivalent to 40 Ethiopian birr at the time of study
Personal and institutional characteristics of the study respondents
Regarding personal characteristics of the study participants, 107 (58.8%) reported they had interest to work in delivery and 112 (61.5%) reported they had manageable workload. Half, 91 (50%) of the health care professional reported they took training on ENC. Among those who took training on ENC, 10.99% had taken training three times and above, and 54.95% had trained once. Regarding the availability of materials, 54.9% reported the availability of guidelines on ENC, and 88.5% reported that cord tie is available in their health facility. Tetracycline eye ointment (98.40%), vitamin K (97.8%), neonatal “ambu” bag (95.1%), and suction device (94.5%) were sufficient amount of available material in selected health institution (Table 2).
Personal and institutional characteristics of the study respondents.

Knowledge of health care provider regarding specific ENC
Overall, 65.9% (95% CI = 60.3–71.4) of health care providers had good knowledge on ENC, while 34.1% had poor knowledge. Among the variables correctly answered in the knowledge assessments of obstetric care providers in the study areas were preventing newborn hypothermia, preventing neonatal bleeding, and recommended treatment of eye infection, with frequencies of 89.6% for the first two variables and 86% for the third variable, respectively. The elements with the fewest correct responses, 6.6% and 67%, respectively, were the time when to start ENC and clamping and cutting of cord for a well-breathing and crying baby. (Table 3).
Knowledge of health care provider regarding specific ENC in Sidama, Ethiopia, 2020 (N = 182).

LBW: low birth weight; ENC: essential newborn care.
Practice of health care provider regarding ENC
The overall rate of good practice in ENC was 56.6% (95% CI = 49.4–63.7).
Of the observed practice, the commonest parameters that were frequently practiced by the caregivers were applying tetracycline eye ointment within 90 min of delivery (88.5%) followed by giving vitamin K, 1 mg IM (intramuscular) on anterior mid-lateral thigh (within 90 min), which was observed to be practiced in about 85.2%. On the contrary, applying chlorhexidine gel (4%) on the cord within 30 min of delivery and placing the baby identification bands on the wrist and ankle (within 90 min) were found to be the least frequently practiced activities among the obstetric care providers with the observed frequencies of 5.5% and 17%, respectively (Table 4).
Practice of essential newborn care among obstetric care providers in Sidama, Ethiopia, 2020 (N = 182).

IM: intramuscular.
Factors associated with practice of ENC
The odds of good practice of ENC was 4.53 times higher among who had interest to work in delivery room compared to their counterpart (AOR = 3.53, 95% CI = 2.04–10.06). Having training on ENC makes the participants 3.65 times more likely to practice compared to those untrained on it (AOR = 3.65, 95% CI = 1.63–8.17). Those who had guidelines on ENC were 6.88 times more likely to practice compared to those who have not practiced (AOR = 6.88, 95% CI = 3.10–15.26; Table 5).
Factors associated with practice of ENC among obstetric care providers in Sidama, Ethiopia.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; ENC: essential newborn care; 1: reference category.
p < 0.001; **p < 0.05.
Discussion
The purpose of this study was to assess the practice of ENC and associated factors among obstetric care providers in public hospitals in Sidama regional state, Ethiopia.
The overall rate of good practice in ENC was 56.6% (95% CI = 49.4–63.7). The finding was almost comparable with previous studies conducted at Khartoum State Teaching Hospital (58.9%), 15 Karbala Teaching Hospital (52.4%), 17 Tigray Central Zone (52.4%), 18 Jimma (51.1%), 7 North Western Tigray (59.8%),7,12 Bahir Dar City (59.7%), 19 and Afar (62.7%). 20
These comparable results could be due to similar parameters used for the evaluation of the practice of ENC in all the studies. In addition, it could also be because of the similarities in study design. Supporting this is the comparable training of all obstetric care providers both scientifically and practically, using nationally and globally recognized standards.21,22 The finding, on the contrary, was lower than the study conducted in Eastern zone public health facilities, Tigray (72.77%) 11 and Addis Ababa (80.7%). 23 The difference could be attributed to the study period, differences in study participants, and the availability of ENC guidelines.24,25
The desire to work in the delivery room was discovered to be a predictor of the practice of ENC at the (AOR = 3.53, 95% CI = 2.04–10.06). It is consistent with Jimma’s and North Western Tigray’s research.12,26 One possible explanation is that they are making their workplace more appealing to their employees. Those who had received training in ENC were more likely to practice good ENC than those who had not with the (AOR = 3.65, 95% CI = 1.63–8.17). This finding is similar to that of a study conducted in North Western Tigray, which found that those who had been trained were more than twice as likely to practice good ENC as those who had not been trained. 12 This comparable result may result from the fact that training can empower health care providers’ skills and improve their performance. Because of the training, caregivers’ abilities will improve, resulting in higher survival rates and better newborn care, as well as a greater desire to work in the delivery room.24,25,27
Those who had access to ENC guidelines were shown to be more likely than those who did not have access to ENC guidelines to practice good ENC (AOR = 6.88, 95% CI = 3.10–15.26). The finding is almost comparable with previous research conducted in Eastern Tigray, 11 North Western Tigray, 12 and Jimma. 26 The similarity may be due to the fact that guidelines provide the health care provider with up-to-date information and instructions on how to perform the activity.1,24,27
Strengths and limitations
Strengths
The practical component of the study included an observational checklist. Furthermore, the study was conducted at six different hospitals, which will increase the representativeness of the data.
Limitations
Despite the fact that private hospitals and health centers provide ENC, the study only included health professionals who worked in public institutions.
The final sample size (182) was smaller than the calculated +10% non-respondent rate (191), and we were unable to include additional hospitals because the study was done during the COVID-19 epidemic, which had a substantial impact on our activities. The social desirability bias, which we sought to eliminate as much as possible, will still exist, and the results of the present study should be interpreted with caution.
Conclusion
The study found that having necessary newborn care standards, being interested in working in the delivery room, and having ENC training are all important factors in implementing ENC practices. Important knowledge gaps were noted in key areas of ENC.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221085840 – Supplemental material for Essential newborn care practice and associated factors among obstetric care providers of public hospitals in Sidama regional state, Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221085840 for Essential newborn care practice and associated factors among obstetric care providers of public hospitals in Sidama regional state, Ethiopia by Dejene Negesse Gonfa, Aberash Eifa Dadhi, Andargachew Kassa, Gemechu Gelan Bekele, Amare Tesfaye Yami, Berhane Ejara Moti and Worku Ketema Bededa in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our heartfelt gratitude to Hawassa University College of Medicine and Health Sciences for funding this study. We would also like to acknowledge Sidama National Regional State Health Bureau for providing us necessary information and their cooperation. We would also extend our special thanks to data collectors, study participants, and hospital administrative, and our friends those who help us in the success of this work.
Author contributions
All authors contributed to data analysis, revising the article, gave final approval of the version to be published, agreed to the submitted journal, and agree to be accountable for all aspects of the work.
Availability of data and material
Full data of the article will be available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Hawassa University and the funder had no role with designing, analysis, and interpretation.
Ethical approval
The Institutional Review Board of Hawassa University College of Medicine and Health Sciences granted ethical approval. A letter of support was also obtained from the Sidama Region Health Bureau and delivered to each hospital. Informed consent was obtained from each study participant before the data collection process proceeded. During the data collection process, data collectors informed each study participant about the research project’s objective and anticipated benefits, and study participants were also informed of their full right to refuse, withdraw, or completely reject part or all of their participation in the study. The investigators were given access to the data, which were collected anonymously. Board (Approval Number/ID): Ref No. IRB/096/12.
Informed consent
A written Informed consent was obtained from each study participant before the data collection process proceeded, following a permission letter that was obtained from Hawassa University College of Health Sciences Institutional Review Board.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.