
Abstract
Background. Around half of child deaths that occur before the age of 5 are related to newborn-related causes. The advice on caring for newborns may not always match with local traditions and beliefs. That’s why it’s important to understand the current newborn care practices and what influences them. This will help implement efforts to reduce newborn deaths. The goal of this research was to assess essential newborn care practices and the factors associated with them among women who have recently given birth. Methods. A community-based cross-sectional study was conducted in Libo Kemekem District from April 1 to May 1, 2021, among 601 women. Face-to-face interviews using a structured questionnaire were employed for data collection. The completeness of the questionnaires was checked, and errors were manually corrected. The data was then entered into EpiData v3.1 and transferred to SPSS v26.0 for analysis. Descriptive statistics were used to calculate frequencies, percentages, means, and standard deviations of the findings. Bivariate and multivariate analyses were performed to assess the association between variables for early newborn care practices (ENCP). In the bivariable models, independent variables that showed a statistically significant relationship at a P-value less than .2 with the outcome variable were considered candidates for the multivariable logistic regression models. In the multivariate regression, a P-value < .05 was considered statistically significant. Results were presented in text, tables, and graphs. Additionally, we checked for multicollinearity and performed the Hosmer and Lemeshow goodness-of-fit test to ensure the validity of the multivariate logistic regression analysis. Result. The study revealed that 54.2% (95% CI, 50%-58%) of mothers practiced comprehensive ENBC. In the multivariable binary logistic regression analysis, several factors were found to be significantly associated with ENBC. Primary education was associated with a reduced likelihood of practicing essential newborn care, with an adjusted odds ratio (AOR) of 0.34 (95% CI: 0.23-0.78). Similarly, secondary education was also associated with a reduced likelihood, with an AOR of 0.51 (95% CI: 0.34-0.89). On the other hand, mass media exposure was associated with an increased likelihood of practicing essential newborn care, with an AOR of 2.03 (95% CI: 1.35-3.07). The number of ANC visits was also a significant factor, with an AOR of 0.403 (95% CI: 0.237-0.686. Furthermore, knowledge about ENBC and newborn danger signs were both important predictors, with AORs of 3.93 (95% CI: 2.09-7.37) and 0.31 (95% CI: 0.12-0.74), respectively. Conclusion. This study reveals a critically low level of essential newborn care practices in the local community, influenced by education, mass media exposure, ANC visits, mothers’ knowledge, and awareness of newborn danger signs. Addressing these factors through targeted interventions can reduce neonatal mortality rates, emphasizing the need for investments in education, health literacy programs, and healthcare services to enhance mothers’ and newborns’ health outcomes.
Background
Essential newborn care (ENBC) is provided to all newborn infants at birth to optimize their health and survival.1,2 Estimates suggest that up to 75% of neonatal deaths could be prevented through cost-effective interventions. Newborn deaths may be substantially reduced through increased use of simple, low-cost interventions, such as breastfeeding, keeping newborns warm and dry, and treating severe newborn infections. 3 The first 28 days of life of a newborn are the most vulnerable time for a child’s survival; especially the first day, week, and month of life are essential times for the survival of children and therefore newborns need careful attention during these periods to increase their survival rate and to improve their health outcomes by applying essential newborn care practice guidelines properly as needed. 4 Due to a lack of appropriate care given to mothers and neonates 48% and 52% of neonatal deaths are contributing respectively and almost all of those deaths could be prevented through low and effective cost interventions like integrated antenatal care, quality care at birth and postnatal period and essential newborn care practice. 5
Globally, 2.5 million children died within the first month of their life in 2018. About, 98% of these deaths occurred in developing countries. This means that approximately 7000 neonatal deaths occur every day. More importantly, close to 3-quarters of these infants died within the first day of their life, with one-third dying on the same day they were born. 5
More than 90% of neonatal deaths occur in sub-Saharan Africa 27 deaths per 1000 live births in 2017 and about half of the deaths occur at home because of inappropriate care to newborns. Ethiopia is one of the countries with the highest neonatal deaths in sub-Saharan Africa. Among all under-5 and infant children deaths, about 62% of deaths occur during the first month of life.6,7
The 2016 EDHS results show that the neonatal, infant and under-5 mortality rates were 29, 48, and 67 deaths per 1000 live births, respectively. This means, 1 in every 35 children dies within the first month, 1 in every 21 children dies before celebrating their first birthday, and 1 in every 15 children dies before reaching their fifth birthday. 8 According to the United Nations inter-agency group child mortality estimation in 2015, in Ethiopia, the current infant, under five, and the neonatal mortality rate is 41, 59, and 28 deaths per 1000 live births respectively, and the main causes of neonatal deaths were birth asphyxia (31.6%), prematurity (21.8%) and sepsis (18.5%). 9
Some of the identified determinants of neonatal mortality were the number of births, place of delivery, frequency of antenatal care use, gestation age at birth, twin delivery, presence of premature rupture of membrane, complication during labor, low birth weight, and neonatal care practice. In addition to these mothers’ ages, the gestational age of the first antenatal care visit and knowledge of the mothers on newborn danger signs and newborn care were factors associated with good neonatal feeding practice.10,11
To reduce neonatal death, the Ethiopian government did many health interventions like training health professionals, enhancing the referral system, integrating health services, and implementing packages of the Health Extension Program and routine immunization. 12 The single most cost-effective intervention to reduce neonatal mortality and morbidity both in developed and developing countries is the promotion of appropriate Essential newborn care practices. Despite this recommendation, there is inadequate adherence to it in middle and low-income countries. 13 To improve the survival of newborns essential newborn care practice is a priority intervention method. These interventions are newborn resuscitation, early identification and management of neonatal infections, identifying barriers to exclusive breastfeeding, applying skin-to-skin contact, appropriate umbilical cord care, and improving the quality of health care during delivery. 14
In Ethiopia, according to the EDHS 2016 report, only 26% of births take place at health institutions and 73% of births are at home. In Libo Kemekem Woreda only 46.9% of births take place at the institution and the rest 53.1% of births were at home.15,16 As a result of home deliveries, mothers receive support from Traditional Birth Attendants (TBAs), relatives, neighbors, and other experienced women from the community. This may lead to maternal and newborn morbidity and mortality, because of a lack of standardized safe delivery and newborn care practices. Traditional practices like pre-lacteal feeding, avoiding first milk (colostrum), swallowing of butter, and application of material like animal dung and other substances on the newborn cord stump were practiced by the community in the study area.
The care of newborns is often complicated by unscientific and unhygienic health practices as well as social taboos, leaving them extremely vulnerable. Past studies have mostly focused on essential newborn care practices in institutional settings, neglecting community settings, especially rural areas with distinct cultural, and socio-economic features. Limited research has addressed the factors influencing essential newborn care practices in these settings. This study is significant as it seeks to evaluate the level of Essential Newborn Care Practice (ENBCP) in a specific region, Libo Kemekm Worda, characterized by unique cultural, topographical, and population attributes. By identifying the associated factors of ENBCP in this particular setting, the study aims to shed light on the challenges and opportunities for improving newborn care practices in the area. The findings of this study can be instrumental in devising targeted interventions and policies to enhance newborn care practices and ultimately improve the health outcomes of newborns in Libo Kemekm Worda.
Methods and Materials
Study Design, Setting, and Period
A community-based cross-sectional study was conducted from April 1 to May 1, 2021, in the Libo Kemekem District. Adiss Zemen is the capital city of the district which is 86 km from Bahirdar.
According to the 2020 population projection provided by the Libo Kemekem Woreda health office, the current population size is 267,848. Out of this, 133 924 are males and 133 924 are females. The population includes 5615 babies under 1 year, 6340 individuals of reproductive age group, and 5808 postnatal care women. There are 17,935 residents in urban areas and 162,606 residents in rural areas. The total number of households in the Woreda is 41,974. For administrative purposes, the Woreda is divided into 32 Kebles, out of which only 4 are urban.
Woreda has 1 primary hospital, 10 health centers, and 28 health posts and each health facility gives health care service to the population of Woreda and nearby populations. The Woreda institutional maternal delivery service coverage was 46.9%. 16
Study Populations, Sample Size Determination, Sampling, and Data Collection Procedures
The study included women aged 15 to 49 who had given birth and lived in selected households within a specific area for at least 6 months. Women who were severely ill and unable to provide information were excluded, as well as infants with caregivers or guardians. The calculated sample size for the study was 601, determined using a single population proportion formula considering the prevalence of 23.1% from a previous study, 95% confidence level, 5% marginal error, 10% non-response rate, and 2.0 design effect. Multi-stage sampling was used to select sampling units, with 10 kebeles selected from a total of 37, and systematic random sampling was applied to select households. Data was collected using structured questionnaires and administered by 6 trained health professionals (Figure 1).

Schematic presentation of sampling procedure essential newborn care practice among Mathers in Libo Kemekem Worda.
Data Quality Control
To assure data quality; representative kebeles were taken by randomization technique and a Multi-stage sampling technique was used to select sampling units. Standardized, structured, and pre-tested questionnaires were administered. The questionnaire’s reliability and validity were examined, with a pretest conducted to ensure its reliability. The questionnaire’s validity was evaluated through content, construct, and criterion validity. To ensure content validity, we made sure the questionnaire covered all relevant aspects of essential newborn care practices. Construct validity was determined by checking if the questionnaire accurately measures the theoretical constructs of interest. Criterion validity was assessed by comparing the questionnaire’s results with an established standard to confirm its accuracy. Furthermore, training was given, regular supervision during data collection, and multivariate analysis was done.
Data Processing and Analysis
The collected data were checked for completeness, cleaned, coded, and entered into Epidata version 3.1 then exported to the SPSS version 26. Descriptive statistical analysis was used to compute the frequency, percentages, standard deviations, and mean of the findings. Bivariable and multivariable logistic regression models were used to identify determinant factors linked to ENCP. In the bivariable models, independent variables that showed a statistically significant relationship at a P-value less than .2 with the outcome variable were considered candidate variables for the multivariable logistic regression models. Crude odds ratios and adjusted odds ratios were obtained with their 95% confidence intervals. P-values less than .05 were considered statistically significant in the multivariable regression. Finally, results were presented in the form of texts, tables, and graphs. Multicollinearity and Hosmer and Lesmshow goodness of fit test were done for multivariate logistic regression analysis.
Operational Definitions
Results
Socio-Demographic and Economic Characteristics of the Respondents
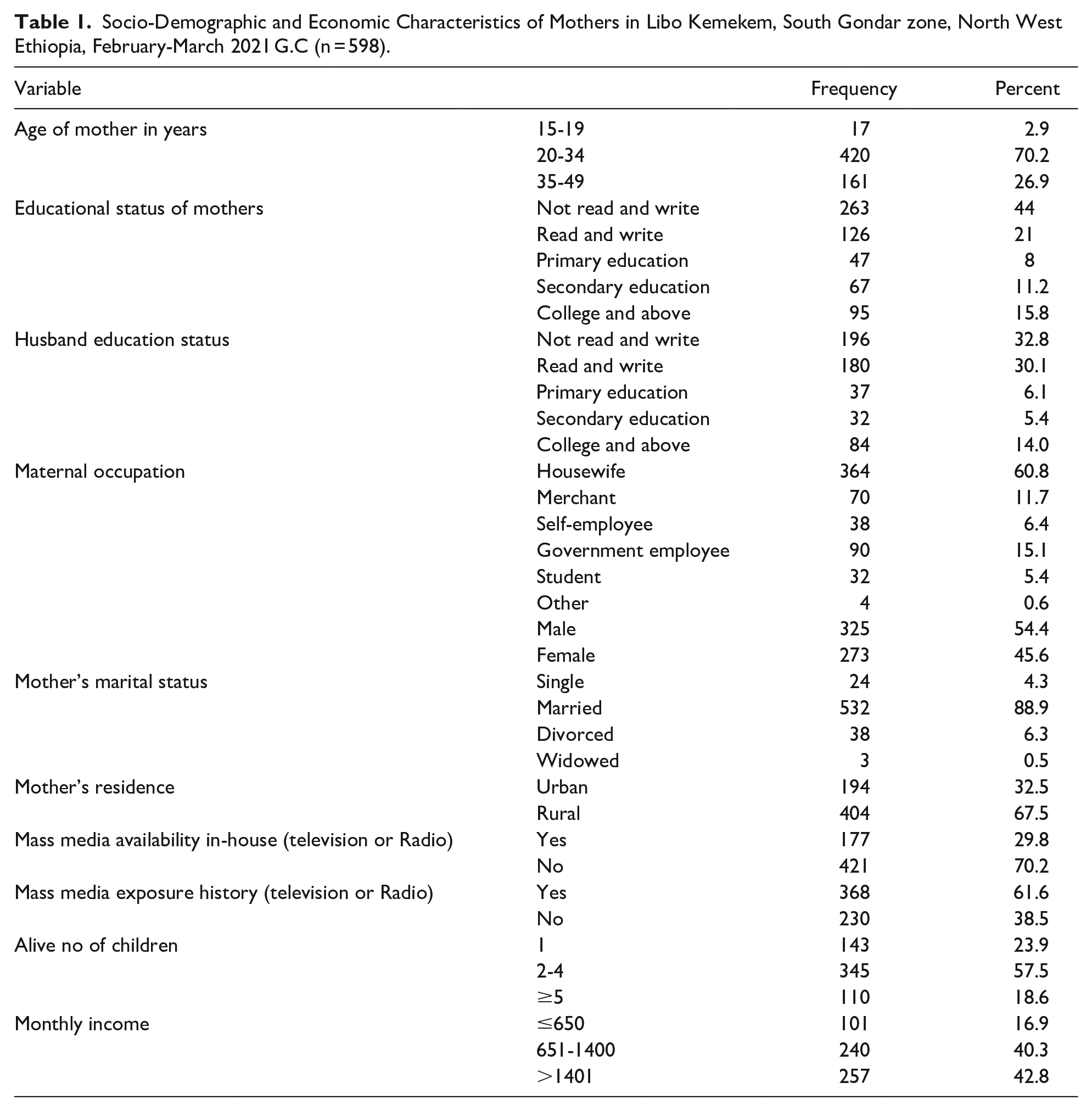
A total of 600 (601) mothers who have under 1 year of children were interviewed which yielded a response rate of 99%. The mean age of the participants was 30 years with an SD of ±6.45) years. Most of the participants (92.4%) were married. Concerning educational status, 259 (43.3%) of mothers cannot read and write. Among all mothers, 364 (60.8%) were housewives, 404 (67.5%) of them were rural dwellers, and 143 (23.9%) of them gave live births for the first time. The majority of participants, 421 (70.2%) had no mass media (television or Radio) in their houses and 368 (61.6%) of them had a mass media exposure history (Table 1).
Socio-Demographic and Economic Characteristics of Mothers in Libo Kemekem, South Gondar zone, North West Ethiopia, February-March 2021 G.C (n = 598).
Mothers Health Care Service Utilization and Obstetric Information
The majority of mothers, 357 (59.7%) had home visits by Health Extention Worker (HEW) in the last 6 weeks (42 days). Among visited mothers health extension workers were given health education on hand washing with soap and clean water before handling their neonate for 353 (98.8%) mothers, on keeping the neonate dry and wrapped for 349 (97.7%) mothers, on breastfeeding immediately after birth within 1 hour for 333 (93.2%) mothers and
on the other hand, the majority of mothers 540 (90.3%) had no history of neonatal death before this delivery but about 58 (9.7%) reported that they had a history of neonatal death. Almost half of the mothers, [327 (54.4%)] were between the age of 25 to 29 years old when they gave first birth. The mean age of the mother at first delivery was 21.02 (SD of ±3.73) years. The majority of mothers 503 (84.1) attended antenatal care (ANC) when they were pregnant of which, 500 (99.4%) had ANC visits at governmental health facilities. Two hundred seventy-eight, 278 (55.27%) mothers attended the first ANC visit 4 months and less than 4 months of gestational age, and 225 (44.73%) mothers attended the first ANC greater than 4 months of gestational age.
Regarding ANC follow-up, 249 (49.5%) mothers had ANC follow-up 4 and above times when they were pregnant with their current baby and 158 (31.4%), 73 (14.5%), 23 (4.57%) of mothers had ANC follow-up 3 times, 2 times, and 1 time during their current pregnancy respectively.
Two hundred sixty-four (44.1%) of mothers attended monthly pregnant mothers meetings when they were pregnant. The majority of mothers, 509 (85.1%) were informed about the care of the newborn particularly cleanliness, 473 (79%) were informed about breastfeeding immediately after birth within 1 hour, 425 (71%) were informed about the delayed bathing of a newborn after 24 hours and 444 (74%) were informed about keeping the cord clean and avoid injuries by a health professional at health institution during ANC visit and delivery. Regarding the place of delivery, 387 (64.6%) gave birth at health facilities, whereas 211 (35.2%) of mothers gave birth at home. Among home-delivered mothers, 159 (75.3%) were delivered due to precipitated labor (Table 2 and Figure 2).
Obstetrics Factors and Health Service Utilization of Mothers During Pregnancy and the Postpartum Period, Libo Kemekem, South Gondar Zone, North West Ethiopia, 2021.


Reasons for mothers for home delivery at Libo Kemekem, South Gondar Zone, North West Ethiopia, 2021.
Concerning the delivery assistance, among mothers who delivered at home, 93(44%) were assisted by their family members. The remaining were assisted by neighbors 68 (32.2%), Relatives 9 (4.2%), and traditional birth attendants 41 (19.4%). Among mothers who delivered at health institutions 208 (53.7%) were delivered by spontaneous vaginal delivery, 71 (18.3%) were delivered by episiotomy, 79 (20.4%) were instrumental delivery and 29 (7.4%) were cesarean section delivery. Among the study mothers, 354 (59.1%) of mothers vaccinated their newborns immediately after birth. Regarding Post-natal care, 239 (39.9%) of mothers were returned for post-natal care. Among mothers who didn’t return for post-natal care, 205 (57.1%) mothers did not return due to the newborn was not sick (Table 2).
Knowledge of Mothers Regarding Newborn Care and Danger Signs
Three hundred ninety-four (65.8%) of mothers responded that nothing should be applied to the cord immediately after cutting for up to 7 days except ordered medication. Three hundred eight (63.5%) of mothers believed that the umbilical cord be handled after cutting without dressing. About, 471 (78.7%) mothers responded newborn babies were bathed/washed after 24 hours of delivery. Among study mothers, 493 (83.2%) believed newborn babies were breastfed within 1 hour after delivery.
Five hundred sixty-two (94.5%) of mothers believed exclusive breastfeeding is important to newborns. About, 562 (93.9%) of mothers believed that mothers should be fed only breast milk to their newborn babies. Among study mothers, 505 (84.4%) responded they knew about newborn danger signs, and from them, 493 (82.2%) and 459 (76.7%) of the mothers mentioned fast breathing and unconsciousness as danger signs of the newborn baby (Figure 3).

Knowledge of mothers toward newborn danger signs in Libo Kemekem South Gondar Zone, North West Ethiopia, 2021.
There were about 8 knowledge-related questions used to assess the knowledge status of mothers toward essential newborn care practice. Based on this, 526 (87.9%) of mothers had good knowledge of essential newborn care practice and the remaining 72 (12.1%) of mothers had poor knowledge of essential newborn care practice.
Breastfeeding Practice of the Mothers
About 526 (87.9%) of mothers were breastfeeding exclusively. Around 422 (70.5%) of mothers were given the first breast milk (colostrum) for their baby and, 383 (64%) were initiated breast milk within an hour after birth. Among mothers who didn’t give the first breast milk (colostrum) to their baby, 123 (69.8%) were due to the fear of illness to the newborn and 53 (29.8%) were due to the feeling of no importance to a newborn. About 71 (11.8%) of the mothers were given additional feeding (pre-lacteal feeding) other than breastfeeding before 6 months to their newborn, from those 34 (46.6%) of mothers were given cow milk followed by butter 32 (43.8%; Table 3).
Practice of Mothers on Timely Initiation of Breastfeeding Libo Kemekem, South Gondar Zone, North West Ethiopia, 2021.

Safe Cord Care Practice
Among mothers who were delivered at home, 200 (94.7%) used new blades and the remaining 11(7%) of mothers used old or non-boiled blades. About 490 (81.9%) of mothers were uncovered, kept dry, and cleaned the umbilical stump to keep the cord safe and clean. Of them, 94 (87%) of mothers covered their babies with a cloth.
About 305 (51%) of mothers reported that they applied something on the cord, among these 19 (6.2%), 153 (50.2%), 132 (43.3%), and 1 (0.2%) mothers had applied cow dung, butter, vaseline, and ointment/oil respectively. Most of the mothers 562 (94.1%), have reported that they went to a health center if the cord bled or had unpleasant discharge and 20 (3.5%) of mothers had to give home medication, while 16 (2.8%) of mothers reported they have to wait until it heals by itself.
Thermal Care Practice
As stated in the operational definition thermal care practice is a maternal practice to avoid bathing before 24 hours of delivery and well-wrapping neonates’ whole body particularly the head with a dry cloth. About thermal care, the result shows, that 339 (56.6%) of newborns were placed in skin-to-skin contact with their indexed mother, and 426 (71.2%) of newborns were wrapped in cloth immediately after delivery. About 191 (31.5%) of mothers bathed their newborn within 24 hours of delivery (Figure 4).

Thermal care practice of mothers to neonates in Libo Kemekem, South Gondar Zone, North West Ethiopia, 2021.
The Overall Essential Newborn Care Practice
Overall, 323 (54%) of mothers had good newborn care practice on the 4 composite variables (initiation of breastfeeding, cord care, bathing of a newborn, and thermal care (skin-to-skin contact), and 275 (46%) of mothers had poor newborn care practice on those 4 composite variables (Figure 5).

Overall essential newborn care practice in Libo Kemekem, South Gondar Zone, North West Ethiopia, 2021.
Factors Associated With Essential Newborn Care Practice
Among the total variables included in the bi-variable binary logistic regression analysis, fourteen variables (age of mother, educational status of mothers, residence, number of alive children, mass media availability, mass media exposure history, monthly income, HEW visit, age at first delivery, ANC visit, Attending monthly mothers group meeting, place of delivery, of the mother, Knowledge about danger Signs of newborn and Knowledge about newborn care practice) were associated with essential newborn practices at P-value < .2. Then multivariable logistic regression analysis was performed using those candidate variables. In the multivariable binary logistic regression analysis, the educational status of mothers, mass media exposure history, ANC visit, Knowledge about dangerous Signs of newborns, and Knowledge about newborn care practice) were found to be significantly associated with essential newborn practices.
Mothers who attended primary and secondary educational levels were less likely to practice essential newborn care by 66% and 49% compared with mothers who attended college and above respectively ([AOR = 0.34, 95% CI (0.23, 0.78)] and [AOR = 0.51, 95% CI (0.34, 0.89)).
The odds of ENBC practice were twofold higher among mothers who had mass media exposure as compared to those who had no mass media exposure history [AOR = 2.03 (1.35, 3.07)]. Mothers who had no ANC follow-up were less likely to practice ENBC by 60% compared to mothers who had ANC follow-up [AOR = 0.403, 95% CI (0.237, 0.686)]. The odds of ENBC practice were 4 folds higher among mothers who had good knowledge of essential newborn care as compared to those who had poor knowledge of essential newborn care [AOR = 3.93, 95% CI (2.09, 7.37)]. Similarly, knowledge of mothers on newborn danger signs was found to be associated with ENBC practice. Those mothers who had poor knowledge of newborn danger signs were less likely to practice ENBC by 70% compared to those mothers who had good knowledge of newborn danger signs [AOR = 0.31, 95% CI (0.12, 0.74)] (Table 4).
Factors associated with essential newborn care practice in Libo Kemekem, South Gondar zone, North West Ethiopia, February- March 2021 (n = 601).

The mode is adequate at a P-value of .947.
Significant Associations of Bi variable with P < .2* and Multivariable analysis with P < .05**.
Discussions
This study found that 54.2% of newborn care practices, including initiation of breastfeeding, cord care, thermal care, and delayed bathing, were adhered to, while 45.8% of mothers exhibited poor practices in these areas.
This percentage is higher compared to studies conducted in East Gojjam Awabel district (23.1%), 17 Damot pulasa woreda (24%), 18 Madura district (40.6%), 19 Lawura District of Ghana (15.8%), 20 rural districts of Gedeo Zone, Southern Ethiopia (24.1%). 21 The variation in findings could be attributed to improved health services coverage, increased awareness, and access to mothers’ health services facilitated by the availability of health facilities and the expansion of health extension programs. Stakeholders need to promote and integrate essential newborn care practices to enhance their implementation in the community.
Regarding cord care, 49.3% of mothers practiced safe cord care by maintaining cleanliness and dryness without applying any substances. This finding is consistent with a study in Aksum town (42.8%) and a study in Bangladesh where nearly half of the participants followed safe cord care practices.22,23 However, it is higher than a study in Damot Pulasa woreda (36%). 18 The variation in results may be due to increased health services coverage, improved mothers’ awareness, and access to mothers’ health services.
In this study, approximately 50.7% of mothers reported using various traditional substances on the umbilical cord stump, such as cow dung (6.2%), butter (50.2%), oil (0.2%), and Vaseline (43.3%). This percentage is lower compared to studies conducted in Damot Pulsa Woreda, Enderta, Tigray,18,24 and higher than studies in Dessie Referral Hospital and Awabel District. 17 The variance in findings could be attributed to increased awareness among mothers regarding the potentially harmful effects of traditional substances applied to the umbilical cord stump or differences in study settings.
The level of timely initiation of breastfeeding within 1 hour in the study area was (63.7%). This is higher than the study done in Mandura district (48.1%), 19 Damot Pulusa Woreda (45.8%), 18 Awabel District (41.6%), 17 India (38.2%), 25 and Bangladesh (40%), 23 This higher result may be due to awareness about the advantage of early initiation of breastfeeding to ensure that the baby had received colostrum. However, the finding of this study is lower than the study done in the Dessie referral hospital (97.1%). 26 The variation in awareness levels regarding the benefits of exclusive and early initiation of breastfeeding could be attributed to differences in study settings. Interestingly, our findings align with a previous study conducted in Aksum town (63.1%), suggesting a consistent trend in this regard. 22
Ideally, a newborn should not be bathed until 24 hours after delivery to maintain body temperature and minimize the risk of hypothermia. In this study, 68.2% of mothers bathed their newborns after 24 hours of birth. The finding of this study is higher than the studies done in Damot Pulusa Woreda, 18 Mandura District, 19 and Awabel District (34.4%). 17 The discrepancy might be due to awareness about the importance of delayed bathing to prevent hypothermia and to ensure optimum thermal care practice. On the other way, the finding of the study was found to be lower than the studies conducted in the Dessie referral hospital, 26 Mekelle City, 27 and Bangladesh. 23 This difference might be due to a relative lack of proper advice before, during, and after birth about the importance of delayed bathing and the study area variation. Another potential reason for the variation could be the presence of specific cultural beliefs within the current study area that impact the practice of newborn bathing soon after birth. Certain communities may consider the vernix and blood covering the newborn’s body as unclean, prompting an immediate need for cleansing due to concerns for the baby’s well-being.
In the current study, Mothers who attended primary and secondary educational levels were less likely to practice essential newborn care by 66% and 49% compared with mothers who attended college and above respectively. The finding of this study is consistent with a study conducted on Mekelle City and Awabel District.17,20 The possible reason might be that less educated mothers may have not a better understanding of the ENBC practices.
In this study, the odds of ENBC practice were 2 folds higher among mothers who had mass media exposure as compared to those of had no mass media exposure history. On the other hand, Mothers who had no ANC follow-up were less likely to practice ENBC by 60% compared to mothers who had ANC follow-up. The finding of this research is consistent with studies conducted in Mandura District, Damot Pulusa Woreda, Mekelle City, and Chencha District.18-20,28 This might be due to women who had not attended ANC having less chance of getting information about the components and the less importance of newborn care practice from health care providers.
The odds of ENBC practice were 4 folds higher among mothers who had good knowledge of essential newborn care as compared to those who had poor knowledge of essential newborn care. The study is consistent with a study conducted in Mandura District and Chencha District.19,28 The possible explanation for this could be knowing essential newborn care makes them practice it.
Similarly, those mothers who had poor knowledge of newborn danger signs were less likely to practice ENBC by 70% compared to those mothers who had good knowledge of newborn danger signs. The finding of this study was supported by other studies.18,27 This could be because most mothers may not have adequate knowledge about newborn care and might be due to inadequate messages about newborn care during antenatal care follow-up.
Limitation of the study: There could be recall bias because the data were collected from those mothers who gave birth within 12 months preceding the study. The study could have a risk of social desirability bias as mothers may not report what they practiced.
Future researchers need to take into consideration the sources of their data and strategies to address potential biases. In this section, we have provided our recommendations on how to overcome 2 types of bias that may arise when studying essential newborn care practices.
Recall bias is when participants may have difficulty remembering past events or behaviors accurately, which may lead to incomplete or incorrect responses. To address this issue, researchers can provide prompts or aids to help participants remember specific details, conduct interviews or surveys shortly after the event to improve recall accuracy and use objective measures or records to verify reported information.
Social desirability bias is when participants may feel pressured to provide socially acceptable or desirable responses, rather than reflecting their true behaviors or beliefs related to essential newborn care practices. To overcome this bias, researchers should ensure confidentiality and anonymity of responses to encourage honest and open communication, use indirect or implicit measures to assess behaviors and build rapport and trust with participants to reduce the likelihood of bias.
The identified factors—educational status of mothers, mass media exposure history, ANC visits, knowledge about dangerous signs of newborns, and knowledge about newborn care practices—all play significant roles in influencing essential newborn care practices in the local community.
Mothers with higher education levels are more likely to adhere to WHO-recommended newborn care practices. Mass media exposure helps in disseminating crucial information on newborn care. ANC visits offer education on essential care practices, while knowledge about danger signs in newborns facilitates early intervention. Lastly, mothers’ knowledge about newborn care practices directly impacts the quality of care provided to newborns.
In summary, addressing these factors through targeted interventions can lead to improved mothers and newborn health outcomes, ultimately contributing to a reduction in preventable newborn deaths in the community.
Conclusions and Recommendation
Overall, the level of comprehensive essential newborn care practice of mothers was considerably low against all composite variables (initiation of BF, cord care, thermal care, and delayed bathing), and 45.8% of mothers had poor practice on the above-listed composite variables. Educational status of mothers (primary and secondary), mass media exposure history, ANC visit, knowledge about essential newborn care, and newborn danger signs were statistically significant predictors of essential newborn care practices. Therefore, it’s important to strengthen health facilities and health posts linkage to increase ANC service utilization, and promotion of essential newborn care practice through awareness creation, provision of counseling, and education about essential newborn care, and
The results of this study have significant implications for both maternal and child health policies and practices. The study found that almost half of the mothers had poor practice when it came to the 4 essential components of newborn care as defined by the WHO. This highlights the need for better education and training for mothers and healthcare providers. Maternal and child health policies should prioritize the provision of accessible and affordable mothers and newborn healthcare services that include education on ENCP (essential newborn care practices). Healthcare providers should be trained on how to effectively communicate and educate mothers on ENCP to ensure that they are implemented correctly.
Moreover, there is a need for community-based interventions to improve mothers’ and newborns’ health outcomes. These interventions should focus on enhancing the knowledge and practice of ENCP among mothers, families, and communities.
Overall, the findings of this study underscore the importance of investing in maternal and newborn health policies and practices that prioritize education, training, and community-based interventions to improve maternal and newborn health outcomes.
List of Abbreviations and Acronyms
ANC: Antenatal Care; CSA: Central Statistical Agency; EBF: Exclusive breastfeeding; E.C.: Ethiopian Calendar; EDHS: Ethiopian demographic health survey; ENBC: Essential new born care; ENBCP: Essential new born care practice; ETB: Ethiopian Birr; HAD: Health development army; HEW: Health extension worker; MDG: Millenium development goal; SDG: Sustainable development goal; TBA: Traditional birth attendant; UN: United Nation; WHO: World Health Organization: RH: Reproductive Health
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241279193 – Supplemental material for Assessing Maternal Adherence to WHO’s Essential Newborn Care Practices in Libo Kemekem District: A Community-Based Study
Supplemental material, sj-docx-1-gph-10.1177_2333794X241279193 for Assessing Maternal Adherence to WHO’s Essential Newborn Care Practices in Libo Kemekem District: A Community-Based Study by Hailemariam Mekonnen Workie, Habtamu Tadele Esey, Birhanu Melaku Shiferaw and Fetlework Workineh Asress in Global Pediatric Health
Footnotes
Acknowledgements
We would like to thank Amhara Public Health Institute for permitting us to conduct this research. Our sincere gratitude and appreciation are forwarded to Libo Kemekm Worda health office, Deber Tabor zonal office, participants, data collectors, and facilitators for their kind cooperation in providing the appropriate information required for this thesis work. We would also like to extend our sincere gratitude to the BMC journal for providing preprint access to our manuscript. 29
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Data Availability Statement
The data used in this manuscript is available upon reasonable request by contacting one of the corresponding authors via email.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The relevant guidelines and regulations of the Declaration of Helsinki carried out all methods. First, ethical approval and permission to conduct this study were obtained from the Institutional Review Board (IRB) of Amhara Public Health Institute with Ethical approval number 10/1068. Then, Officials at different levels were communicated through letters, and permission was taken from each selected kebeles to collect data. Written informed consent was taken from each study subject before the interview after the purpose of the study was explained to them. If participants were under 16 years old, informed consent was obtained from the parents/guardians. Confidentiality of the information was assured and privacy of the respondent was maintained throughout the study process.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.