
Abstract
Objective
This study was performed to determine predisposing factors of perinatal mortality among deliveries at tertiary hospitals in East Wollega, Western Ethiopia.
Methods
This institutional-based unmatched retrospective case–control study involved 810 samples (270 perinatal deaths and 540 controls) selected from the study hospitals. For each case, two controls were selected. Data were collected using a pretested structured questionnaire. Data were entered into EpiData Version 3.1 and exported to SPSS Version 25 for analysis. Descriptive analysis and logistic regression were performed. The adjusted odds ratio with 95% confidence interval was calculated, and statistical significance was declared at a P-value of <0.05.
Results
The statistical analysis revealed the following independent determinants of perinatal mortality: rural residence, lack of antenatal care, preterm delivery, induction of labor, presence of obstetric complications, breech presentation, shoulder presentation, low birth weight, congenital malformation, and not using a partograph.
Conclusion
Given the determinant factors of perinatal mortality in the study area, health facilities are recommended to implement appropriate antenatal care, intrapartum care, and neonatal care to prevent perinatal mortality. They are also advised to use partographs and ensure better access to antenatal care facilities.
Introduction
Perinatal mortality continues to be problematic worldwide, especially in poorer countries. 1 Estimates indicate that perinatal mortality is five times higher in developing nations than in industrialized ones. 1 According to two studies, approximately 98% of newborn deaths and 97% of stillbirths that were reported globally occurred in developing nations.2,3
Because of deep-rooted poverty and poor access to limited health facilities, Sub-Saharan Africa (SSA) has one of the highest levels of perinatal mortality worldwide. In one study, the estimated incidence of perinatal mortality within SSA was 34.7 per 1000 births. 4 Ethiopia is one of the countries in SSA with the highest perinatal mortality rate. According to the Ethiopian Demographic Health Survey 2016, the perinatal mortality rate was 33 per 1000 births in Ethiopia. It was highest in Somali (50 deaths per 1000 pregnancies) and lowest in the Affar region and in the Southern Nations, Nationalities, and People’s Region (26 deaths per 1000 pregnancies for each region). 2
Most of the perinatal mortality rates in Ethiopia were reported from hospitals instead of from community-based studies. The trend has been stable at about 90 per 1000 total births in hospitals and 40 per 1000 total births in community-based studies.1,2,4–6
According to different studies in Ethiopia, various factors such as women’s sociodemographic characteristics, obstetric history, and medical conditions; health facility-related factors; and newborn factors have been identified as determinants of perinatal mortality.7–11 However, the determinant factors of perinatal mortality in the western part of Ethiopia have not been assessed. Therefore, identifying determinants and implementing evidence-based interventions are crucial to reducing perinatal death. The present study was performed to identify the potential determinants of perinatal mortality.
Methods
Study setting
The study was conducted at tertiary hospitals in East Wollega, which contains two tertiary hospitals and three primary hospitals. The two tertiary hospitals are Wollega University Referral Hospital (WURH) and Nekemte Specialized Hospital (NSH). Both hospitals are in the town of Nekemte, which is the capital of the East Wollega zone, situated in Western Ethiopia, 331 km from Addis Ababa. According to Central Statistics Agency 2005, the town has an estimated total population of 84,506 people (42,121 male and 42,385 female). More than 5 million people in the catchment area are served by the two tertiary hospitals in the town, which also act as referral centers in East Wollega. Both hospitals offer patients services in medicine, surgery, gynecology and obstetrics, pediatrics, radiology, and laboratory medicine. Five gynecologists and 21 midwives work in the obstetrics and gynecology department at WURH. There are 23 midwives and 3 gynecologists at NSH. The average number of monthly deliveries at NSH and WURH is 272 and 256, respectively.
This study was approved by the Research and Ethics Committee of the Institute of Health Science of Wollega University (approval number WU/RD/369/2012). A written permission letter was obtained from administrators at Wollega University Referral Hospital and Nekemte Specialized Hospital. Data were collected after receiving verbal permission from all concerned departments. All patient details have been de-identified. The need for written informed consent was waived by the ethics committee because of the retrospective nature of this study.
Study period
The study was conducted from 1 April 2020 to 10 May 2020. It was performed within the framework of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 12
Study design
This was a retrospective case–control study.
Study population
The study population comprised stillbirths, early neonatal deaths, and selected live births who were discharged alive. The cases were stillbirths and early neonatal deaths, and the controls were selected live births discharged alive from the study hospitals during the specified period. Cases for which the card number was either lost or not recorded in the logbook were excluded.
Sample size determination
The formula for two population proportions was used to calculate the sample size, which was computed by Epi Info Version 7.2.2 assuming a case:control ratio of 1:2, odds ratio of 2.02, and estimated proportion of exposure among controls of 8% with power set at 80% and confidence level of 95%. The sample size was calculated from a similar study conducted in Addis Ababa by taking preterm birth as one of the main exposure variables for perinatal mortality that provided the maximum sample size. 9 Therefore, a total sample size of 780 was calculated (260 cases and 520 controls). After adding a 10% nonresponse rate for incomplete charts, the total sample size was 858 (286 cases and 572 controls).
Sampling procedures
The study was conducted at two tertiary hospitals in East Wollega. The sample size was proportionally assigned to each study hospital based on the average number of monthly deliveries and perinatal deaths that had occurred during the 3 months before data collection. Delivery and neonatal registry books were reviewed. Cases and controls were selected from the card room using the card numbers in the registration books. Cases were randomly selected. For each case, two neonates who had been born on the same day and discharged alive were selected as controls.
Data collection procedures
Data were collected using a pretested structured questionnaire from the mothers’ medical records. The questionnaire was developed after reviewing different pieces of literature.7–11,13–20 It contained sociodemographic factors, obstetrics factors, medical and healthcare-related factors, and newborn-related factors. The admission history, labor follow-up sheet, delivery summary, and antenatal care follow-up sheet were used to gather information for the study variables. Data were collected by six midwives with two supervisors.
Data quality control
To maintain data quality, a pretest was performed on 5% of medical charts at NSH using data from the year 2016 to check the appropriateness of the data collection tool, and any necessary amendments were considered. Six midwives and two supervisors were recruited and trained by the principal investigator. The collected data were reviewed and checked for omissions, completeness, and consistency by the supervisor on daily basis during the data collection period.
Data processing and analysis
The data were checked manually for completeness and entered into EpiData Version 3.1, then cleaned and exported to SPSS Version 25 (IBM Corp., Armonk, NY, USA) for data analysis. Descriptive statistics using measures of central tendency and dispersion, frequencies, and diagrams were used to check the data distribution. Cross tabulation was also performed to determine the distribution of different variables with the outcome variable. Bivariate logistic regression analysis was performed, and variables with a P-value of <0.25 were entered into the multivariate analysis; variables with a P-value of <0.05 were considered statistically significant, and the adjusted odds ratio (AOR) with 95% confidence interval (CI) were used to control for possible confounders and to interpret the results. Model adequacy was assessed using the Hosmer–Lemeshow goodness-of-fit test, and a P-value of <0.05 indicated that the model fit the data. Finally, the results were summarized and presented using tables, graphs, and charts.
Results
Sociodemographic characteristics of mothers
In total, 810 (94.4%) mothers’ data (270 perinatal deaths (cases) and 540 survivors of the perinatal period (controls)) were included in this analysis. The data for 48 (5.6%) mothers were incomplete. Of the total perinatal deaths, 180 (66.7%) were stillbirths and 90 (33.3%) were early neonatal deaths. The mothers’ mean age was 26.3 ± 5.4 years for cases and 25.2 ± 4.6 years for controls. Nearly all mothers (260 (96.3%) of cases and 527 (97.6%) of controls) were married. Most of the mothers of the cases (177 (65.6%)) but a smaller proportion of the mothers of the controls (179 (33.1%)) were from rural areas (Table 1).
Sociodemographic characteristics of mothers who gave birth at tertiary hospitals in East Wollega from 1 January 2017 to 30 December 2019.

Data are presented as n (%).
Obstetric characteristics of mothers
In total, 127 (47.0%) cases and 271 (50.2%) controls were born from nulliparous mothers. Most of the mothers of the cases and controls (208 (77.0%)) and (498 (92.2%)), respectively) had antenatal care follow-up. Nearly three-fourths of all deliveries (586 (72.3%)) were at term. With respect to the duration of labor, more than half of mothers of cases (162 (60.0%)) and controls (343 (63.5%)) gave birth after <12 hours of labor. More than three-fourths of all mothers (629 (77.7%)) gave birth after spontaneous onset of labor. Of all 810 deliveries, nearly three-fourths (586 (72.3%)) occurred by spontaneous vertex vaginal delivery, 18.9% by cesarean section, and 7.5% by instrumental deliveries (forceps or vacuum). In terms of the mothers’ obstetric history, most of the mothers of cases (259 (95.9%)) and controls (480 (88.9%)) had no history of cesarean section. More than half of the cases (142 (52.6%)) and a smaller proportion of controls (99 (18.3%)) were born from mothers who had experienced at least one obstetric complication in their index pregnancy (Table 2). The proportion of mothers who delivered without a partograph follow-up was 208 (77.0%) among cases and 200 (37.0%) among controls (Figure 1).
Obstetric characteristics of mothers who gave birth at tertiary hospitals in East Wollega from 1 January 2017 to 30 December 2019.

#Hypertensive disorders of pregnancy, obstetrics hemorrhage, labor abnormalities, cord prolapse.
ANC, antenatal care; TT, tetanus toxoid; PM, perinatal mortality.
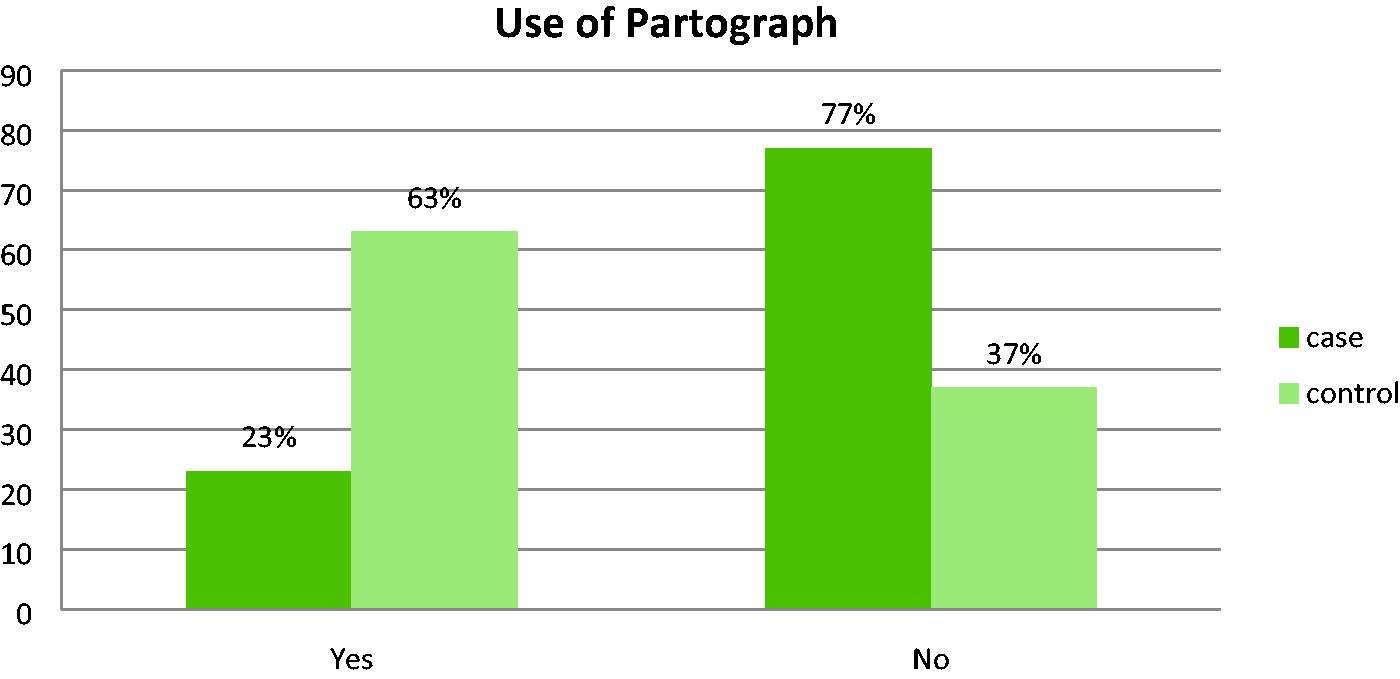
Partograph utilization among mothers who gave birth at tertiary hospitals in East Wollega from 1 January 2017 to 30 December 2019.
Newborn characteristics
Regarding fetal presentations, vertex presentation occurred in 202 (74.8%) cases and 483 (89.4%) controls. Breech and transverse presentations accounted for 18.9% and 3.7% of cases and for 6.9% and 0.6% of controls, respectively. Most of the mothers gave birth to a single fetus (92.2% of cases and 95.6% of controls). Of the total births, more than half (466 (57.5%)) were male and 344 (42.5%) were female. The proportion of infants with low birth weight was 40.4% in the case group and 7.6% in the control group. The congenital malformation rate was 11.9% in the case group and 0.9% in the control group. Among the total births, 198 (24.4%) had a very low 1-minute Apgar score (0–3). Of these, 197 (73.0%) were among the cases (Table 3). The most common causes of early neonatal death were neonatal asphyxia (35.6%), prematurity (34.4%), neonatal sepsis (20.0%), and respiratory distress syndrome (8.9%) (Figure 2).
Newborn characteristics at tertiary hospitals in East Wollega from 1 January 2017 to 30 December 2019.
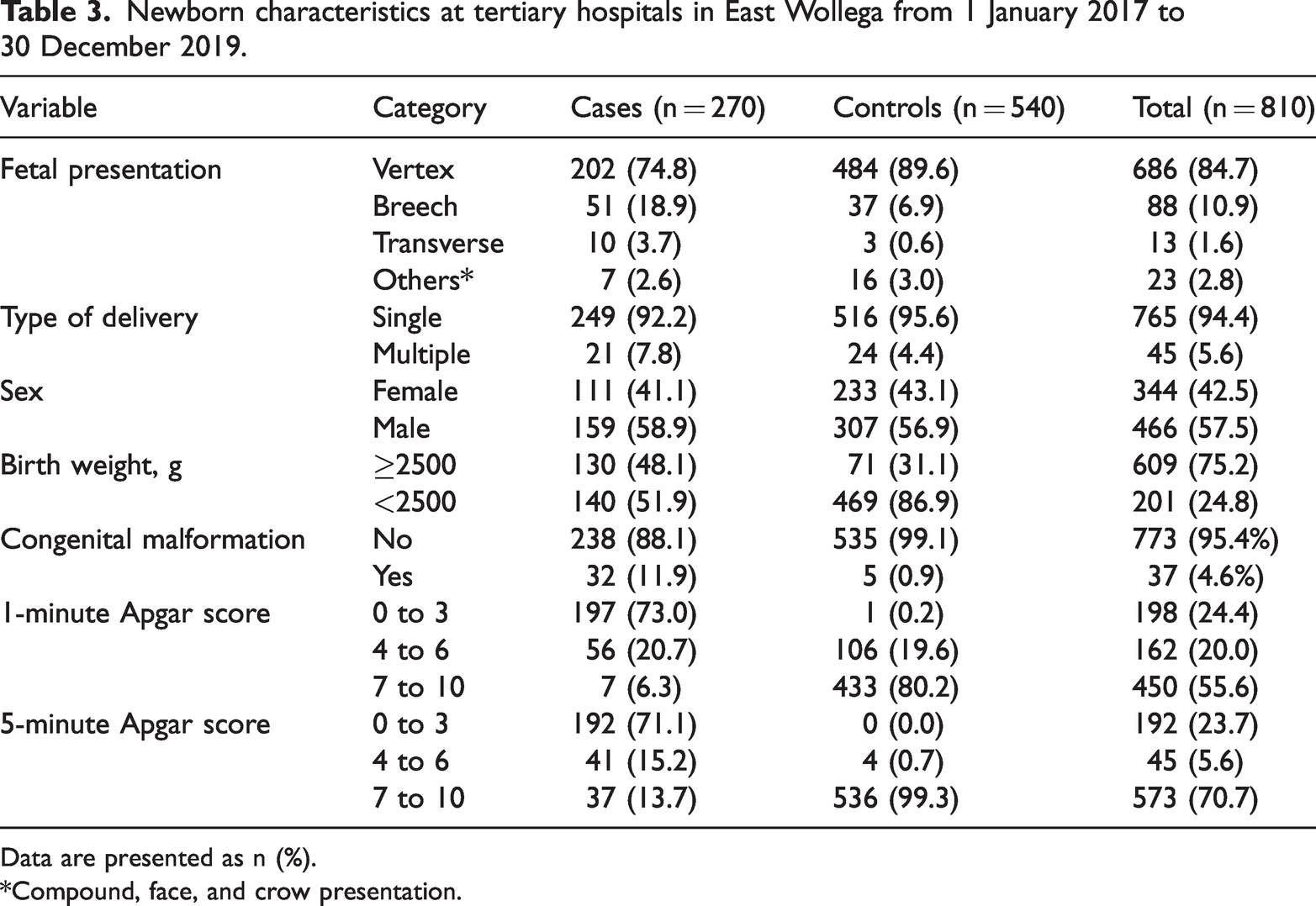
Data are presented as n (%).
*Compound, face, and crow presentation.

Causes of early neonatal deaths at tertiary hospitals in East Wollega from 1 January 2017 to 30 December 2019.
Determinants of perinatal mortality
In the multivariable logistic regression analysis, the following sociodemographic factors were identified as independent determinants of perinatal mortality: rural residence; obstetric factors such as no antenatal care follow-up, preterm delivery, induction of labor, and presence of obstetric complications; medical factors such as a maternal hemoglobin level of <11 g/dL; neonatal factors such as fetal malpresentation (breech presentation and shoulder presentation/transverse lie), low birth weight, and congenital malformation; and health facility-related factors such as not using a partograph during labor.
The study revealed that the odds of a rural residence were 2.35 times higher among cases than controls (AOR, 2.35; 95% CI, 1.44–3.83). The number of mothers who had no antenatal follow-up was 2.41 times higher among cases than controls (AOR, 2.41; 95% CI, 1.35–4.29). Preterm delivery was also a significant determinant of perinatal mortality. The odds of preterm delivery were 2.75 times higher among cases than controls (AOR, 2.75; 95% CI, 1.61–4.70). The odds of induced labor onset were 2.23 times higher among cases than controls (AOR, 2.23; 95% CI, 1.33–3.72).
The occurrence of obstetric complications was also a significant determinant of perinatal mortality. The odds of obstetric complications were 2.77 times higher among cases than controls (AOR, 2.77; 95% CI, 1.81–4.24). The odds of a mother’s hemoglobin level of <11 g/dL were 2.05 times higher among cases than controls (AOR, 2.05; 95% CI, 1.10–3.84). The odds of low birth weight were 3.59 times higher in cases than controls (AOR, 3.59; 95% CI, 2.20–5.84).
Malpresentation was another significant determinant of perinatal mortality. The odds of breech presentation were 3.52 times higher among cases than controls (AOR, 3.52; 95% CI, 1.92–6.45), and the odds of transverse lie/shoulder presentation was 11.37 times higher among cases than controls (AOR, 11.37; 95% CI, 1.94–66). The odds of a fetus with congenital malformation were 9.15 times higher among cases than controls (AOR, 9.15; 95% CI, 2.98–28.08). The odds of labor without follow-up using a partograph were 3.75 times higher among cases than controls (AOR, 3.75; 95% CI, 2.46–5.71) (Table 4).
Determinants of perinatal mortality among births at tertiary hospitals in East Wollega from 1 January 2017 to 30 December 2019.

Data are presented as n (%) unless otherwise indicated.
*P < 0.05, **P < 0.01, ***P < 0.001.
#Hypertensive disorders of pregnancy, obstetrics hemorrhage, labor abnormalities, cord prolapse.
AOR, adjusted odds ratio; CI, confidence interval; ANC, antenatal care.
Discussion
This study revealed different determinants of perinatal mortality in the study area. Knowing these determinants is crucial to recognizing the focus area for minimization of perinatal mortality. The present study showed that living in rural areas was significantly associated with an increased risk of perinatal mortality. This result is in line with studies conducted in Jimma and Tigray.6,13 This might have occurred because mothers who live in rural areas face delays in reaching health facilities due to poor transportation. This leads to obstetrical complications and increases the risk of perinatal loss. 14
In this study, mothers who had no antenatal care follow-up had higher odds of experiencing perinatal mortality than their counterparts, which is in line with studies conducted in Hawassa and Nigeria.8,15 This might be because antenatal care helps mothers to undergo screening for high-risk factors and to take appropriate measures if risks are detected. Additionally, it creates a good opportunity for health care providers to implement immediate management. Moreover, clinicians can provide counseling to mothers and families about what should be done to minimize risks.
Preterm deliveries were significantly associated with an increased risk of perinatal deaths. This finding is similar to studies conducted in Tigray and Addis Ababa.8,9 Similar findings were also reported in India and Kenya.10,11 This could be due to the presence of underlying maternal medical conditions or obstetric complications. Preterm birth is also associated with an increased risk of neonatal complications (e.g., sepsis, birth trauma), which can lead to neonatal death.9,11
Regarding the onset of labor, mothers who were induced with medications (oxytocin or misoprostol) were more likely to experience perinatal mortality. This finding differs from that of a study conducted at a Jimma University specialized hospital, which showed that labor onset has no association with perinatal mortality. 7 This discrepancy might be due to the differences in the study setting, study design, and intrapartum follow-up during induction or the presence of underlying maternal problems.
With respect to obstetric complications, perinatal mortality was more common in mothers who did than did not develop obstetric complications. The risk of perinatal death was higher among mothers with preeclampsia, antepartum hemorrhage, and cord prolapse. This result is consistent with those of studies conducted in Arbaminch, 10 Kenya, 16 and Zambia. 17 This could be due to the direct effect of these complications on the fetus or the lack of early detection and intervention of these complications. Obstetric complications such as antepartum hemorrhage and hypertension might predispose to induction before term, which leads to iatrogenic preterm birth. However, a study conducted in Addis Ababa contradicted this study result. 9 It indicated that obstetric complications are not significantly associated with perinatal mortality. This might have occurred because most of the mothers (96%) in the study underwent antenatal care follow-up. Such care allows most of the causes of complications to be identified during follow-up and helps health professionals to take appropriate measures before obstetric complications occur.
In the present study, fetal malpresentation (breech presentation and shoulder presentation) were associated with an increased risk of perinatal mortality. This finding is in line with previous studies conducted in Hawassa and Jimma.7,8 This finding may be related to the fact that obstetric complications such as cord prolapse and abnormal labor are secondary to malpresentation.
Additionally, birth weight was a significant determinant of perinatal death. Low-birth-weight newborns had a risk of perinatal mortality. This finding is comparable with those of studies performed in Addis Ababa, Uganda, and India.9,18,19 This might be because low-birth-weight newborns are more easily exposed to neonatal complications such as hypothermia, hypoglycemia, and sepsis. Another possible explanation is that low-birth-weight newborns are usually preterm deliveries subjected to the above-mentioned complications.
In this study, congenital malformation was a significant determinant of perinatal mortality. The perinatal mortality rate was much higher among neonates with than without congenital malformation. This is similar to the findings of studies performed in Addis Abba, 9 Kenya, 16 and Australia. 20 This finding might be due to a lack of screening and early detection of congenital malformations that are not compatible with life during the antenatal period. For complications that are compatible with life, this finding might be due to poor neonatal care.
The present study also showed that partograph utilization was a significant determinant of perinatal mortality. Mothers whose labor was not followed by partograph monitoring had higher odds of experiencing perinatal mortality. This finding is in line with studies conducted in Tigray and Addis Ababa.9,11 This is because the use of a partograph can enable health professionals to identify any abnormalities during labor. Therefore, it can prevent perinatal loss that can be managed if an early diagnosis is made.
Finally, the present study showed that perinatal asphyxia and prematurity were among the most common reasons for early neonatal death. This is similar to the findings of studies in Nigeria and India.19,21 This might be due to the presence of obstetric complications, poor intrapartum care, and poor neonatal care.
A limitation of this study is that it was based on secondary data. This made it difficult to obtain all necessary variables, such as educational status, occupation, income, and birth interval. Another limitation is that this study was retrospective in nature.
Conclusion
Given the determinant factors of perinatal mortality in the study area, health facilities are recommended to implement appropriate antenatal care, intrapartum care, and neonatal care to prevent perinatal mortality. They are also advised to use partographs and ensure better access to antenatal care facilities.
Research Data
Research Data for Determinants of perinatal mortality at tertiary hospitals in East Wollega, Western Ethiopia: a case–control study
Research Data for Determinants of perinatal mortality at tertiary hospitals in East Wollega, Western Ethiopia: a case–control study by Rut Oljira, Elias Merdassa, Gemechu Kejela, Firehiwot Fentahun and Temesgen Tilahun in Journal of International Medical Research
Footnotes
Acknowledgements
The authors would like to thank the Wollega University Institute of Health Sciences for funding this study. The authors also sincerely thank all supervisors and data collectors for their cooperation and support during the study period.
Author contributions
All authors participated in the conceptualization, formal analysis, investigation, methodology, supervision, visualization, writing-original draft, writing-review and editing, and approval of the final draft. All authors read and approved the manuscript.
Availability of data and materials
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wollega University Institute of Health Sciences.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.