
Abstract
Background. Low- and middle-income countries (LMICs) face persistent challenges in reducing pediatric mortality, particularly in emergency settings. Simulation-based training (SBT) offers a practical solution to improve pediatric emergency care by enhancing healthcare providers’ skills and clinical decision-making. Objective. This narrative review explores the effectiveness, challenges, and implementation strategies of SBT for pediatric emergency care in LMICs. Methods. A comprehensive literature search was conducted using PubMed, Scopus, and Google Scholar databases and 36 selected articles were included. Results. Findings highlight significant improvements in clinical skills, teamwork, and decision-making through SBT, with low-fidelity and in-situ simulations emerging as cost-effective alternatives for these settings. Case studies from Ghana, India, and Uganda showcase innovative, affordable models, including task-trainers and homemade mannequins, which address local barriers. Despite its potential, further research is needed to evaluate long-term outcomes and establish standardized assessment metrics. Conclusion. SBT represents a scalable and impactful strategy to strengthen pediatric emergency care and reduce child mortality in LMICs.
Introduction
In the last few decades, international efforts have been made to reduce infant and neonatal mortality. The mortality rate for children under 5 has significantly declined; it went from 93 deaths per 1000 live births in 1990 to 39 deaths per 1000 in 2018. But low- and middle-income countries (LMICs), especially those in Africa, continue to have high rates of infant death. The overall child mortality rate in these areas is still 76 fatalities for every 1000 live births, although there is wide regional variation in this rate.1,2
Improving pediatric emergency care has become a priority in low-resource settings since many newborn deaths might be avoided with easy, affordable, and successful interventions. Every year, almost 1 million babies pass away on their first day of life, followed by another million within the first week and nearly 2 million more during the up to 28-day neonatal period. Furthermore, there are about 3 million stillbirths worldwide each year. 3
For a long time, simulation has been a practical teaching method to reduce mortality associated with resuscitation. 1 The World Health Organization (WHO) has advised adding simulation-based training to these programs to enhance care in low-resource settings. The specific requirements of low-resource environments have led to the development of programs like Saving Children’s Lives, Helping Babies Breathe (HBB), the Emergency Triage, Assessment, and Treatment (ETAT and ETAT+) Essential Steps in Managing Obstetrical Emergencies (which includes neonatal care) in South Africa, and others. 1
This review will focus on simulation in pediatric emergency care as an effective way of enhancing it, especially in low-resource settings such as Africa and the Middle East. Finally, we are going to address the challenges of implementing it with some recommendations from international guidelines and success cases to further scale into LMICs.
Materials and Methods
This narrative review aimed to evaluate the literature in English related to pediatric emergency care in low-resource settings, specifically focusing on the role of simulation-based training. An electronic search was conducted using PubMed, Scopus, and Google Scholar databases. The search covered studies published from January 2013 up to October 2024. The key search terms used were combinations of “simulation” or “simulation training,” or “simulation-based training” and “low resource” and “countries,” “settings,” or “nations,” as well as “pediatrics,” “child,” and “emergency.”
The inclusion criteria for the studies focused on original research, systematic reviews, other narrative reviews, literature reviews, and case studies that specifically addressed simulation training for pediatric emergency care in low-resource settings. Studies that did not provide specific information about pediatric emergency care, which includes trauma care, simulation training, or the targeted low-resource environments were excluded. We further applied exclusion criteria for papers with inadequate sample size, unclear methodology, or not meeting quality control standards regarding design and statistical rigor.
100 abstracts were initially screened, and 36 full-text articles were selected for detailed evaluation. One independent reviewer conducted the selection process. In cases of disagreement, a second reviewer was consulted, and their decision was considered final. The final articles selected were reviewed for key themes related to the effectiveness, challenges, and outcomes of simulation-based training in pediatric emergency care in low-resource settings. Relevant data were systematically extracted and categorized into thematic subgroups.
Ethical Approval and Informed Consent
Ethics approval and Informed Consent were not required for this narrative review
The Role of Simulation in Pediatric Emergency Training
The practice of simulation, by definition, is creating a virtual reality where a situation or an environment represents a real-life event to learn, practice, evaluate, test, or acquire a skill. There has been an exceptional expansion in using simulation-based training (SBT) in health care over the past 2 decades as simulation-based training expanded to be used as a tool to uplevel clinical skills and teamwork in addition to evaluating the competency of medical and trauma management in the pediatric population and across all other specialties. 4
Types of Simulation: High-Fidelity Versus Low-Fidelity Versus In-Situ
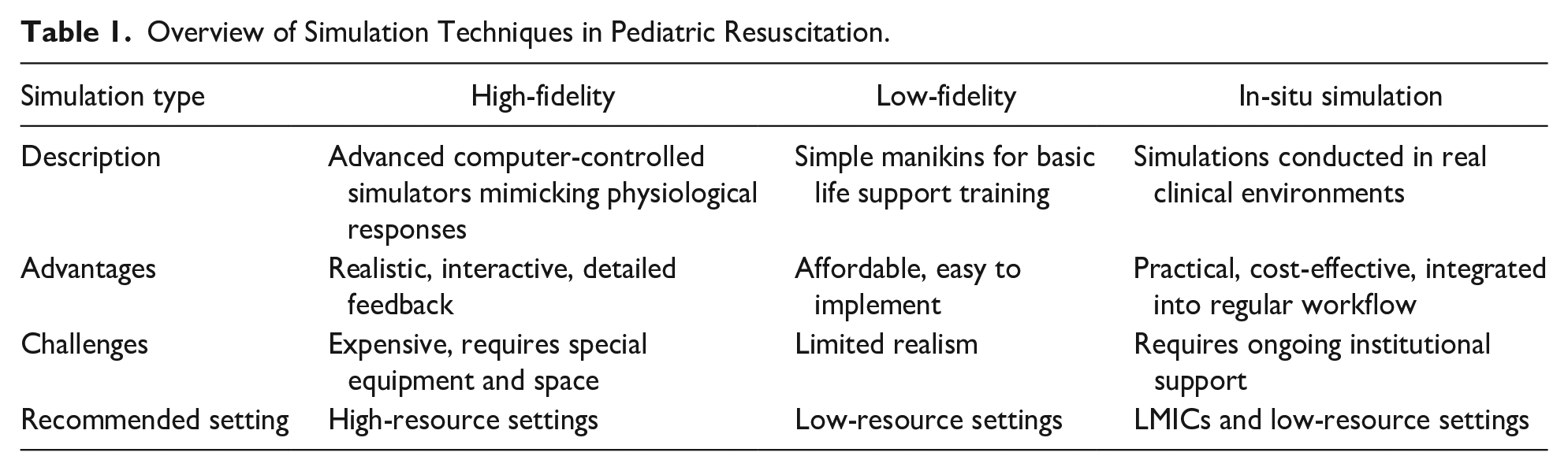
Low-fidelity simulations have been used for decades to represent clinical events or for basic life support training, using simple manikins and traditional mock codes. Vise versa, high-fidelity simulations are more recent, offering more realistic experiences through computer-controlled simulators. Advanced manikins can simulate breathing and heart sounds, chest movements, palpable pulses, and airway changes, for example, swelling and spasms. Additionally, they feature advanced monitors that show vital signs and ECG rhythms and can be programed to mimic real-life responses to interventions. 4 An overview of the key features, advantages, challenges, and recommended settings for different simulation techniques in pediatric resuscitation is provided in Table 1.
Overview of Simulation Techniques in Pediatric Resuscitation.
Benefits of Simulation in Pediatric Emergency Settings
Simulation training in pediatric critical care has proven benefits in increasing clinical proficiency and decreasing morbidity. In sub-Saharan African pediatric institutions, mortality rates have declined because of programs like the ETAT program of the WHO, particularly during the crucial first 48 hours after hospital admission. 2
Furthermore, the HBB training program has demonstrated notable advancements in the treatment of newborns, as seen by the increase in stimulation of non-breathing infants from 36% to 100% and the improvement in bag-mask ventilation (BMV) efficacy from 20% to 100% after the program. These results emphasize the significance of simulation in improving care in pediatric emergencies. 1
Challenges in Pediatric Emergency Training in Low-Resource Settings
Lack of Access to Advanced Medical Equipment
Creating a training curriculum that simulates sustainability and raising the standard of neonatal critical care has not been easy in nations with few resources. Criticisms have been raised regarding the adequacy of newborn resuscitation programs (NRP) in low-resource settings. Programs such as Kenya’s Emergency Triage, Assessment, and Treatment (ETAT) and Helping Babies Breathe (HBB) have faced challenges due to limited access to essential equipment. However, updates to HBB, including incorporating chest compression guidelines, align with local resources and Kenyan pediatric recommendations, aiming to address these concerns. 1
The lack of pediatric intensive care units (PICUs), inadequate pediatric equipment, and restricted access to pediatric critical care and emergency medicine (PCCEM) specialists make it challenging to set up training programs in Ecuador. Most LMICs lack PCCEM, which has led to a high rate of neonatal morbidity. 5
Shortage of Trained Personnel
Due to shortages or complicated schedules, removing instructors and participants from their places of employment can be difficult. It took 13 on-site training sessions over 6 weeks in a case study at Tenwek Hospital to train 98 providers. Longer-term programs like ETAT had high dropout rates due to emergency triage and night call schedules. Studies also stated that finding suitable participants for on-site training was difficult because they were frequently required for crucial clinical positions, and the hospital administrator did not send them. 1 Again, most low-resource settings cannot provide the vast number of educated staff required to give such oversight. In the study, 14 research coordinators offered continuing practice supervision. Such supervised frequent practice would not have been possible due to our educators’ clinical responsibilities. 1
Infrastructure Challenges in Low-Resource Settings
A large portion of sub-Saharan Africa receives their education through lectures and textbooks, the predominant method used in the region, particularly for training. One of the major issues identified in a study on essential steps in managing obstetric emergencies was the educators’ unease with conducting simulations. Studies conducted in Kenyan, ETAT, and HBB indicate that these settings require teamwork training. Although doctors and nurses typically operate independently, the facilitator of simulation-based training must include a variety of practitioners. 1
Types of Simulation Techniques Suitable for Low-Resource Settings
Simulation-based training in low-resource settings faces several challenges, including a lack of infrastructure, time, and a simulation culture. However, management support, a trained team, and smart sourcing can facilitate successful adoption. Efforts to integrate simulation into existing curricula and raise awareness of its benefits are crucial for enhancing pediatric emergency care. Institutional leadership drives these changes and supports simulation-based initiatives. 6
Task Trainers and Their Applications in Low-Resource Settings
In low-resource settings, task trainers have proven highly effective in enhancing medical training, especially for specific technical skills like surgery and obstetrics. A review of healthcare simulation in developing countries revealed that hand-made task trainers were used in most studies, demonstrating significant improvements in participants’ technical abilities and satisfaction. These low-cost models, some costing as little as 15 dollars, allow for the widespread adoption of simulation-based training, even in areas with minimal resources, making them crucial tools for healthcare education in such settings. 7
For example, the Helping Babies Breathe (HBB) program in Kenya demonstrated the transformative impact of task trainers. Prior to training, only 36% of non-breathing infants received adequate stimulation during resuscitation, and the effectiveness of bag-mask ventilation (BMV) was just 20%. Following the introduction of low-cost neonatal mannequins as task trainers, these figures rose to 100% for both adequate stimulation and BMV effectiveness. 1 This underscores the critical role of task trainers in improving neonatal outcomes in resource-limited contexts.
Similarly, the PediSTARS Initiative in India utilized locally modified, low-cost mannequins for skill training in neonatal resuscitation and airway management. These cost-effective models provided high-realism training opportunities, leading to significant improvements in provider confidence and procedural skills. 8
Homemade Mannequins for Basic Skill Training
Cost is a significant barrier to implementing SBT in low-resource settings. PediSTARS innovatively addressed this challenge by utilizing and modifying low-cost mannequins to create effective training tools. These modifications achieved high-realism simulations, demonstrating that valuable simulation experiences can be provided even in resource-limited settings. This strategy is particularly relevant for basic skill training, where low-cost or homemade mannequins offer practical, hands-on learning without expensive technology or infrastructure. 8
Integration of Low-Cost Simulation Techniques Into Training Programs
Integrating low-cost simulation techniques into regular training requires overcoming barriers like time constraints and resource shortages. The study highlighted that a flexible approach to debriefing, including “flash debriefs” in time-constrained environments, allowed for more efficient use of simulation training. Leadership support and team building were identified as crucial enablers for successfully embedding simulation-based learning into routine training, which could improve health outcomes in low-resource settings. 9
Simulation for Pediatric Resuscitation Training
Simulation-based training has emerged as a vital component in equipping healthcare professionals for pediatric resuscitation, where timely interventions are essential. A growing body of research highlights the positive impact of simulation on clinical performance and decision-making in critical situations. 10
The use of simulation techniques in pediatric resuscitation scenarios is pivotal for optimizing response times and enhancing the standard of care in emergencies involving children.
Importance of Simulation in Pediatric Resuscitation Care
The COVID-19 pandemic necessitated rapid adaptations in pediatric emergency care to ensure patient safety and healthcare worker protection. Regular multidisciplinary simulation sessions were employed to refine processes, enhance communication, and develop protocols for critical situations. These simulations effectively disseminated new practices and optimized workflows, underscoring the vital role of simulation in improving care for critically ill children while minimizing risks during unforeseen emergencies. 11
Key Techniques Used in Pediatric Resuscitation Simulation Training
Pediatric residency programs increasingly utilize simulation to enhance trainees’ procedural and resuscitation skills, addressing the gap in their training. A review of the literature highlights the effectiveness of simulated procedural and resuscitation scenarios, though results vary across studies. Techniques such as video-assisted debriefings, mock resuscitation scenarios, and structured evaluations are crucial. 12 Despite promising findings, further research is needed to validate assessment tools and explore how simulation skills translate to real-world patient outcomes in pediatric care.
Impact of Simulation on Resuscitation Outcomes in Low-Resource Settings
At Tenwek Hospital in Kenya, implementing the HBB program significantly improved neonatal resuscitation outcomes. Before HBB, resuscitation skills were limited, with only 36% of nonbreathing infants receiving adequate stimulation. Post-HBB training, this rate increased to 100%, and BMV effectiveness rose from 20% to 100% in observed cases. The training resulted in a substantial increase in Objective Structured Clinical Examination (OSCE) scores, doubling from a mean of 8.5 to 15.7 (P < .001), showcasing the program’s effectiveness in enhancing the skills necessary for improved neonatal survival in low-resource settings. 1
Simulation for Managing Pediatric Trauma in Low-Resource Settings
Pediatric trauma is a leading cause of death and disability, particularly in LMICs, where 95% of childhood injury deaths occur. Tailored pediatric trauma training in these regions presents an opportunity to improve outcomes. A review of course offerings in LMICs found that training frequently includes simulations, didactic modules, and clinical mentorship, though trauma-specific education remains limited. 13 Expanding accessible training, such as simulation-based programs, could significantly improve pediatric trauma care in these settings
Pediatric Trauma Challenges in Low-Resource Settings
Pediatric traumatic brain injuries (TBIs) represent a major global health concern, contributing significantly to childhood mortality and disability, especially in LMICs. Road traffic accidents (RTAs) are the primary cause of TBIs in these regions, compounded by insufficient pre-hospital and hospital care, as well as inadequate rehabilitation resources. The outcome for TBI patients in LMICs is notably worse, with mortality rates double those in high-income countries (HICs). This is particularly true for severe TBIs, where the lack of advanced neurosurgical and neurocritical care facilities further complicates management.14,15
Simulation Techniques for Trauma Care
In trauma care, simulation techniques have become essential for enhancing teamwork and communication among clinicians. A study involving focus groups with multidisciplinary trauma care professionals highlighted the benefits of in situ trauma simulations with debriefing sessions. These simulations provided a valuable opportunity for team members to practice critical skills such as leadership, communication, and cooperation. Participants noted that these simulations helped improve team dynamics, with leadership being a key factor in successful trauma management. 16 The study underscored the importance of continued simulation-based training to address nontechnical skills often overlooked in traditional medical training.
Impact of Simulation on Pediatric Trauma Outcomes
Simulation-based training for pediatric trauma care has positively impacted several critical aspects of trauma resuscitation. A review of 47 studies highlighted that simulation training is strongly associated with improvements in nontechnical skills, such as teamwork and communication, and measurable resuscitation outcomes, such as the number of tasks completed and time to task completion. However, while simulation significantly enhances provider knowledge and the speed of trauma interventions, little evidence directly links it to better patient outcomes. 17 The variability in training methodologies and reporting standards suggests the need for more consistent approaches to studying the full potential of simulation in pediatric trauma care.
Cost-Effectiveness of Simulation in Low-Resource Settings
Simulation-based training in pediatric emergency care has proven to be more cost-effective in the long term compared to traditional training methods. 18 While simulation requires an initial investment in equipment and resources, the benefits it provides in terms of skill retention, improved care quality, and reduced reliance on costly, real-world interventions make it a financially viable solution for low-resource settings.
Comparative Cost-Benefit Analysis of Simulation Versus Traditional Training
Traditional training methods, which often rely on lectures and textbook learning, are limited in their ability to provide hands-on experience. Simulation-based training, in contrast, offers direct application of learned skills in a controlled environment, making it more effective in improving practical competencies. Although initial costs for simulation may be high—particularly for equipment like manikins and high-fidelity monitors—these tools can be used repeatedly, reducing the need for expensive consumables or constant upgrades. 7 For instance, a study in Ecuador found that despite the upfront costs, simulation training led to improved team coordination and reduced errors during real-life resuscitation, highlighting its long-term cost benefits. 5
Long-Term Cost Savings in Pediatric Emergency Care
The long-term savings associated with simulation stem from its ability to improve clinical outcomes and reduce medical errors. As healthcare providers gain proficiency through repeated simulation drills, they become more adept at handling critical emergencies, leading to fewer complications and lower healthcare costs in the long run.7,19 In Nepal, for instance, a simulation-based pediatric emergency program significantly improved care quality without the need for frequent costly retraining, as the manikins and task trainers used were durable and required minimal maintenance 19 . Moreover, simulation training has been linked to reduced mortality rates in pediatric care, which translates into financial savings for health systems. 5
Economic Challenges and Solutions in Low-Resource Settings
Despite its potential for cost savings, economic barriers remain a challenge in implementing simulation-based training in low-resource settings. High initial costs for equipment, the need for trained facilitators, and limited financial support can hinder widespread adoption 7 . However, innovative solutions such as homemade mannequins and low-cost task trainers have been developed to mitigate these expenses 1 . Additionally, partnerships with international organizations and donor support have proven successful in establishing simulation centers in low-income regions.5,19
Challenges and Barriers to Simulation in Low-Resource Settings
Simulation-based training, though beneficial, faces several obstacles in low-resource settings. These challenges range from high upfront costs to a lack of infrastructure and resistance from healthcare staff who are unaccustomed to new teaching methodologies. Addressing these barriers is crucial to scaling simulation programs and enhancing pediatric emergency care.
High Upfront Costs of Simulation Programs
The most significant barrier to adopting simulation training in low-resource settings is the high upfront cost of equipment and software. Manikins, particularly high-fidelity ones that can simulate complex physiological responses, are expensive, and low-resource settings may lack the financial resources to acquire such tools. 7 In South America, the cost of establishing a pediatric critical care simulation center was mitigated with donations and partnerships from foreign institutions, but this model won’t always be feasible for all settings. 5 Additionally, the need for simulation-specific training for instructors adds to the overall cost 19 . Nevertheless, alternatives such as task trainers and low-tech manikins have proven useful in addressing these cost challenges. 7
Lack of Infrastructure to Support Simulation Training
Another major challenge is the lack of infrastructure to support simulation-based training. Many hospitals in low-resource settings are not equipped with dedicated spaces for simulation labs, and even basic utilities like reliable electricity and internet access can be inconsistent.7,19 In Kenya, for instance, simulation programs were constrained by the lack of physical space and technical support needed to operate simulation tools, which limited the scope of training that could be offered 1 . Additionally, the absence of robust hospital networks to share resources and information hampers the development of sustainable simulation programs. 7 To overcome these infrastructure challenges, some programs have repurposed existing spaces or used portable equipment for simulation training. 19
Overcoming Resistance to Adopting New Training Methods
Resistance to new training methodologies is another significant barrier. Many healthcare providers in low-resource settings are accustomed to traditional learning models, such as classroom-based lectures, and may be hesitant to embrace simulation training. 5 This resistance is often due to a lack of familiarity with simulation and its potential benefits. In Ecuador, efforts to introduce simulation into pediatric emergency care were initially met with skepticism from staff, who felt that traditional training methods were sufficient. 5 However, after seeing improvements in patient outcomes and staff confidence, resistance began to decrease.
To overcome this challenge, programs must include clear communication about the benefits of simulation and provide opportunities for staff to experience the advantages firsthand. 1 Introducing simulation gradually, starting with simple task trainers before progressing to more complex scenarios, can help ease the transition for staff who are unfamiliar with the technology. 7 Additionally, ensuring that simulation training is culturally contextualized and tailored to the specific needs of the healthcare staff can further reduce resistance. 1
Figure 1 provides a visual summary of the key barriers to implementing simulation-based training programs in LMICs.
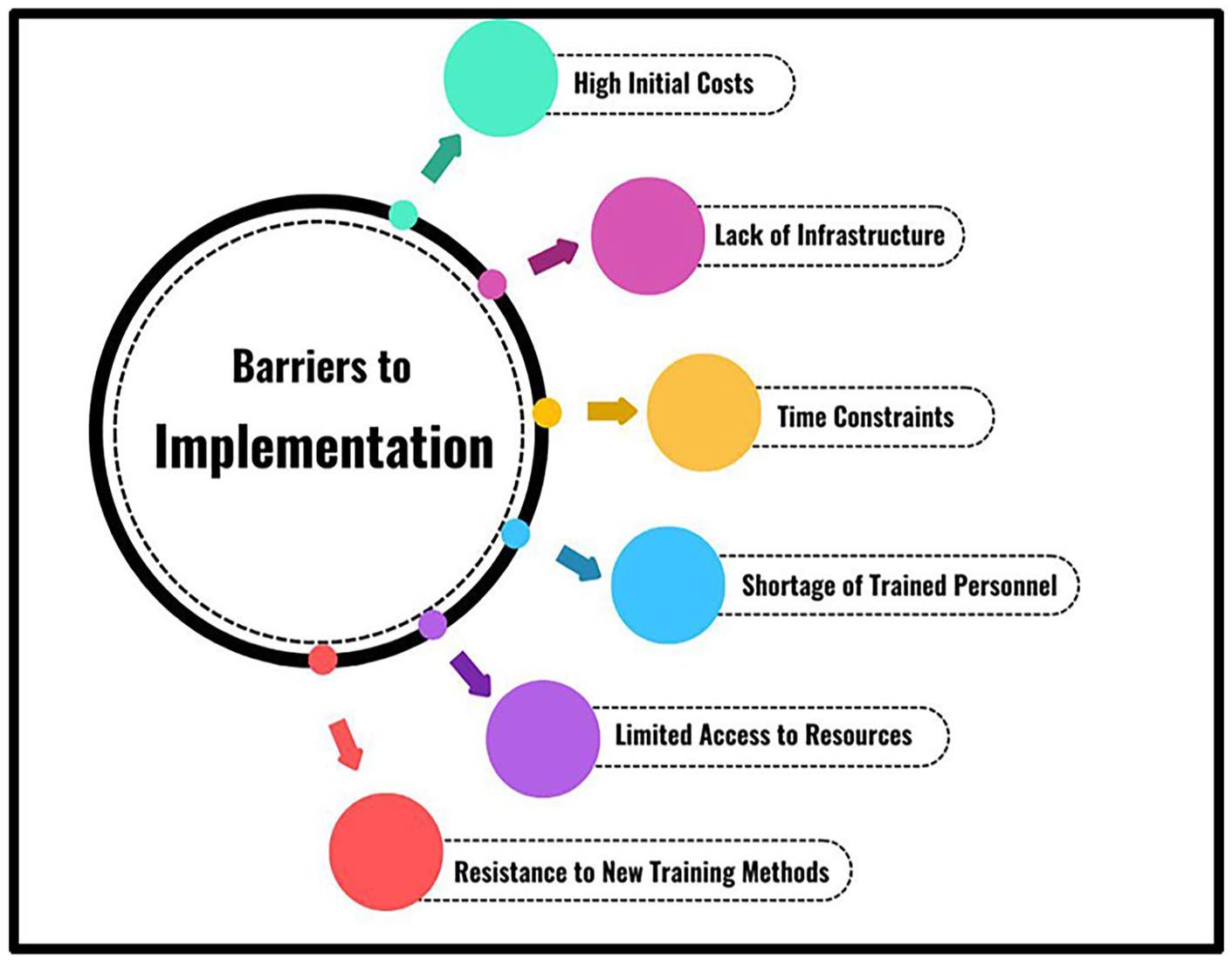
Summary of barriers to implement simulation-based training programs in LMICs.
Successful Implementation of Simulation-Based Training Programs in LMICs
Programs for training based on simulations have become a viable means of improving healthcare results, especially in environments with limited resources. Delivering high-quality healthcare is extremely difficult in low- and middle-income countries (LMICs), particularly when it comes to emergency pediatric treatment. 20 On the other hand, simulation-based training has been a successful tactic for enhancing healthcare practitioners’ clinical abilities.
In this part, we will look at case studies from Ghana, India, and Uganda. These countries have effectively implemented simulation training programs emphasizing trauma treatment, emergency care, and pediatric resuscitation. These examples of successful implementation of simulation-based training programs in LMICs are summarized in Figure 2.

Successful implementation cases globally.
Ghana: Integration of Low-Cost Simulation Models for Pediatric Resuscitation
Ghana’s pediatric emergency care systems have included low-cost simulation models with impressive results. Ghana has embraced low-cost, locally produced models that mimic real-life pediatric resuscitation scenarios in resource-constrained settings, where access to high-fidelity simulation technologies may be limited. Several healthcare facilities have effectively used these models, allowing medical professionals to practice vital resuscitation procedures without requiring pricey equipment. 21
Healthcare professionals who were taught with these inexpensive simulation models showed a notable increase in their capacity to carry out pediatric resuscitations, which improved patient outcomes. Furthermore, using locally made models guaranteed that the simulation tools were appropriate for the unique problems encountered by the Ghanaian healthcare system in addition to lowering costs. Ghana has developed a sustainable training strategy that considers financial and clinical limitations. This has been accomplished by promoting collaboration among educators, healthcare workers, and local innovators. 21
India: Community-Based Pediatric Emergency Training With Low-Fidelity Simulations
Implementing community-based pediatric emergency training programs in India has played a pivotal role in providing life-saving medical treatment to underprivileged and rural regions. Because many Indian districts lack access to sophisticated simulation technology, unlike high-resource settings, low-fidelity simulation models are being used to teach healthcare staff in emergency pediatric care. These low-fidelity simulators have been included in community healthcare practitioners’ training programs to imitate critical clinical settings, including airway management and basic resuscitation methods. 22
The effectiveness of these community-based training initiatives emphasizes the value of contextually appropriate simulation models that can bridge the gap between the availability of resources and the need for superior emergency treatment. This strategy has helped healthcare professionals in rural regions become more competent while boosting their self-assurance and readiness to handle pediatric crises. 22
Uganda: Peer-Led Simulation Training in Pediatric Trauma Care
Peer-led simulation training programs effectively improve healthcare personnel’s abilities to manage pediatric trauma situations in Uganda. Uganda implemented a peer-led strategy to address the scarcity of skilled trainers in pediatric trauma treatment. Healthcare professionals with specialized training in simulation-based approaches were assigned to educate their peers. The peer-to-peer concept has been incredibly successful in guaranteeing that instruction is always accessible, even when there are no outside trainers present.23,24
Pediatric trauma treatment in Uganda has greatly improved since peer-led simulation training was introduced, especially in remote and low-resource settings. Improved competency in handling severe injuries, such as burns, fractures, and head injuries, which are frequent among pediatric patients, has been shown by healthcare workers educated under this approach. Furthermore, the peer-led method establishes a culture of cooperation and ongoing education, where healthcare professionals are motivated to exchange information and expertise. 24
Role of Task-Shifting and Simulation in Empowering Non-physician Healthcare Workers
Task-shifting, or the transfer of some medical responsibilities from doctors to healthcare professionals who are not doctors, such as nurses and community health workers (CHWs), has shown to be an effective tactic in solving the scarcity of healthcare workers, especially in situations with limited resources. Simulation-based training greatly enhances these employees, enabling them to assume pivotal positions in pediatric emergency treatment. 25
Training Nurses and Community Health Workers Using Simulation
Simulation training gives healthcare personnel who are not physicians the practical skills needed to manage pediatric crises. Nurses and CHWs can practice life-saving techniques through realistic clinical scenarios, including resuscitation, airway management, and trauma care. Their clinical judgment is improved by this practical approach, which makes it possible for them to react appropriately in actual circumstances. 26
Impact of Task-Shifting on Pediatric Emergency Care
Task-shifting has enhanced pediatric emergency treatment by increasing the number of healthcare professionals in underprivileged regions when paired with simulation training. Previously restricted in their role, CHWs and nurses are now educated to provide prompt, high-quality treatment, relieving pressure on overworked doctors and enhancing patient outcomes. 27
Case Studies Showing Success in Non-Physician Training
Task-shifting programs based on simulation have proven effective in places like rural Uganda and India. Improved survival rates and overall healthcare delivery have resulted from the skills of non-physician healthcare personnel who are educated through simulation in handling pediatric crises. 28
Measuring the Impact of Simulation on Pediatric Emergency Outcomes
Simulation-based training has emerged as a crucial component in preparing healthcare professionals for pediatric emergencies where timely and effective interventions are vital. A systematic review of 79 studies indicated that such training significantly enhanced clinical performance in time-critical tasks and adherence to established guidelines. 20 Notably, improvements in team dynamics and technical skills were observed for up to 6 months post-training, suggesting that simulation not only fosters immediate skill acquisition but may also have lasting effects on emergency response capabilities in pediatric care settings. 20
Key Metrics for Evaluating Simulation Training Outcomes
Clinical performance, response times, and patient outcomes measure simulation effectiveness in pediatric emergencies. Clinical performance is assessed through proficiency in critical airway management and resuscitation tasks. Improved response times, crucial during emergencies, are directly linked to improved survival rates. Patient outcomes, such as reduced mortality and morbidity, are the ultimate indicators of successful simulation training.20,29
Methods for Measuring Clinical Improvements
Clinical improvements from simulation-based training were evaluated using qualitative and quantitative methods. Standardized pre- and post-training evaluations, often with checklists, assess technical skills, decision-making, and teamwork enhancements. Video recordings and debriefing sessions offer insight into performance, stress levels, and team communication effectiveness. Longitudinal studies track skill retention over time, providing valuable data on the long-term benefits of simulation training.29,30
Evidence of Improved Pediatric Emergency Care Outcomes
Evidence supports the effectiveness of simulation-based training for enhancing pediatric emergency care outcomes. For instance, a study of high-fidelity simulation in neonatal resuscitation showed significant improvements in knowledge and skills, leading to better clinical outcomes. 29 Another study in Nepal indicated marked gains in procedural skills and confidence among healthcare providers after simulation training, particularly in pediatric resuscitation and sepsis management. 30
Table 2 provides a detailed comparison of simulation-based training in HICs versus LMICs, highlighting key differences in infrastructure, resources, pedagogical approaches, and barriers to implementation.
Comparison Between Simulation Training in High-Income Countries (HIC) Versus Low-Middle Income Countries (LMIC).

Recommendations for Scaling Simulation Training in Pediatric Emergency Departments in LMICs
To effectively scale simulation training in pediatric emergency departments in LMICs, it is essential to integrate pediatric-specific content into the existing curricula. Developing low-cost simulation resources and collaborating with local institutions can enhance accessibility. 31 Engaging community health workers will broaden outreach, and ongoing evaluation will ensure programs meet local needs and improve pediatric emergency care outcomes. 31
Practical Strategies for Scaling Simulation Programs
Scaling simulation training in pediatric emergency departments (EDs) in LMICs is essential for improving health care outcomes. Effective strategies include organizing multidisciplinary workshops that involve healthcare providers such as nurses, physicians, and paramedics. These workshops can utilize low-fidelity simulation models to maintain cost-effectiveness while providing meaningful learning experiences. For example, workshops in Nepal demonstrated significant improvements in participants’ confidence and skills through hands-on practice in real-life scenarios. 30
Collaborative Partnerships
Collaborating between local healthcare institutions and international organizations is vital for scaling simulation training. These collaborations enhance resource-sharing, expertise, and training. Implementing train-the-trainer models allows local providers to receive advanced simulation training, enabling them to educate their peers. This approach builds a local capacity and fosters sustainability. Integrating simulation training into existing medical education curricula ensures that all healthcare providers acquire essential skills. 31
Sustainable, Low-Cost Simulation Initiatives
Sustainable, low-cost simulation initiatives require innovative strategies to leverage existing resources and community involvement. Integrating simulation training into routine clinical practice enhanced team performance without significant costs. Using in-house facilities and experienced staff allows hospitals to create effective and economical programs. 20 Engaging local medical schools and community organizations in co-host training sessions can further reduce costs and foster collaboration. 30
Recommendations for Future Research
Future research should evaluate the effectiveness of simulation training in pediatric emergency care outcomes. Longitudinal studies must assess long-term effects on clinical performance and patient outcomes. Developing standardized evaluation metrics will enable the comprehensive assessment of programs, ensuring relevance and engagement. 30 These steps will contribute to continuous improvement of simulation training in LMICs.
Chapter 1: Simulation for Improving Pediatric Disaster Preparedness in Low-Resource Settings
Simulation-based training is increasingly recognized as a vital tool for preparing healthcare workers to effectively manage pediatric disasters, including mass casualty incidents. In low-resource settings, where access to advanced medical facilities and training can be limited, simulations provide a practical and adaptable solution for enhancing emergency preparedness. 20
Role of Simulation in Pediatric Disaster Preparedness
Simulation is vital for pediatric disaster preparedness, as it creates realistic scenarios for healthcare providers. It allows participants to practice critical skills safely, enhancing decision-making and teamwork under pressure. Research shows that simulation training boosts the confidence and competence of healthcare workers, enabling more effective responses during real disasters.32,33
Case Examples of Disaster Response Training in Low-Resource Settings
Case studies have shown that simulation-based training is effective in low-resource environments, significantly improving emergency response capabilities. For example, in-situ simulations in primary care offices enhance staff preparedness for pediatric emergencies. 32 Training initiatives in Uganda and Mexico have also successfully used local resources to educate first responders, resulting in better emergency outcomes. 34
Impact on Improving Pediatric Disaster Management
Simulations can significantly affect pediatric disaster management. Studies have shown that healthcare professionals trained in simulations are better equipped to handle emergencies and reduce morbidity and mortality rates among pediatric patients.35,36 Additionally, these exercises promote a culture of continuous learning, encouraging teams to refine their skills and protocols regularly for more effective disaster response.
Chapter 2: Simulation for Neonatal Emergency Care in Low-Resource Settings
In low-resource settings, simulation-based training is essential to enhance neonatal emergency care. By fostering hands-on experience and teamwork, these simulations significantly improve clinical skills and confidence, ultimately leading to better outcomes for vulnerable newborns. 20
Importance of Simulation for Neonatal Resuscitation Training
Simulation is crucial for neonatal resuscitation training, enabling healthcare providers to safely practice essential skills. Realistic scenarios enhance the ability to perform tasks during emergencies. Research indicates that simulation-based education significantly improves knowledge retention and practical skills for effective neonatal care.35,36
Simulation Techniques for Neonatal Emergency Management
Various simulation techniques have been used to enhance neonatal emergency management. These include high-fidelity simulations using advanced manikins that mimic real-life physiological responses and low-fidelity methods such as role-playing scenarios. Each technique provides unique benefits: high-fidelity simulations allow for immersive experiences, whereas low-fidelity methods are often more accessible in resource-limited settings. 36
Impact of Simulation on Neonatal Care Outcomes
The simulation significantly improved neonatal care outcomes. Studies indicate that simulation-based training facilities report lower neonatal complication rates and improved overall survival rates. 35 Integrating these programs into routine training enhances clinical competencies among healthcare providers, directly benefiting newborns in low-resource environments. 35
Conclusions
SBT has proven to be an effective method for enhancing clinical competencies, team dynamics, and decision-making skills in pediatric emergencies, where rapid and accurate responses are crucial. By utilizing both high- and low-fidelity simulations, as well as in-situ models, healthcare providers can gain hands-on experience that improves readiness for real-life scenarios. The successes of programs in Ghana, India, and Uganda demonstrate how SBT can be tailored to meet local needs, employing innovative, low-cost approaches that are accessible and sustainable.
However, SBT in low-resource settings faces significant barriers. High initial costs, limited infrastructure, and resistance to new teaching methodologies challenge the scalability of SBT. Nonetheless, the adoption of low-cost task trainers, homemade mannequins, and peer-led programs have shown promise in overcoming these obstacles, enabling more widespread implementation even in financially constrained environments. Building partnerships, securing funding, and fostering a simulation culture will be essential for the sustainable growth of SBT in LMICs.
Finally, standardized metrics for assessing SBT effectiveness will be vital to track progress and refine training programs. SBT presents a scalable, adaptable solution that can significantly improve pediatric emergency care and reduce child mortality in LMICs. With strategic investments and continued innovation, SBT has the potential to transform emergency care practices, providing essential support for fragile healthcare systems.
Footnotes
Acknowledgements
The authors thanks each and every emergency pediatrician that is involved in the caring and protection of children especially in places where is happening conflict.
Authors’ Contributions
Del Castillo Miranda, Jose Carlos is the principal author and has contributed to the crafting and arranging of all the sections, references, abstract, introduction, methods, results, and conclusions corresponding to the original draft and also added the comments from the second reviewer. Oweidat, Majd authored the Results section and contributed to the review and revision of the final version of the manuscript, as well as arranging the tables in the manuscript. Ali Abady, Eslam Moumen has done Table 2 and written segments in the Results section of the manuscript. Shehadeh, Mohammad Hakam has done both Figures 1 and 2 and collaborated with Chapters 1 and 2 of the results section. Aziz, Mayam Mohamed has done the Results section and part of the introduction of the original draft. Onyejesi, Chibuike Daniel has done a segment of Results section in the manuscript and corrected the original draft applying comments from the first reviewer. Alsabri, Mohammed is the senior and corresponding author of this manuscript, he had the original idea and conducted the team for elaborating this manuscript. Also has provided insights and access to high-quality information as an expert field emergency pediatrician.
Data Availability Statement
This narrative review did not generate new data. Data used in this review are available in the referenced articles.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This narrative review did not involve human subjects; therefore, an ethics review committee and informed consent were not applicable.
Informed Consent/Patient Consent
No patient or participant consent was required as this article is a narrative review and did not involve human subjects.
Trial Registration Number/Date
Not applicable