
Abstract
Background. Pediatric populations are highly vulnerable to various diseases and are at risk of irrational prescribing practices, which can impact treatment outcomes and contribute to increased healthcare costs. Knowledge of disease, prescribing patterns, and knowledge of drug administration help to promote rational drug use in pediatric care. Objective. To assess the prevalence of common diseases and prescribing patterns in the Pediatric outpatient department of Kankai Nagar Hospital. Methods. A 1-month cross-sectional study was conducted on 245 pediatric patients at Kankai Nagar Hospital. Random sampling was used, and data were collected from prescriptions and patient-caregiver interviews. Descriptive statistics were used to evaluate prescribing trends, and costs were calculated to assess economic implications. Results. Among the patients, 60% were male, with upper respiratory tract infections being the most common diagnosis (26.5%). The average number of drugs per encounter was 3.08, higher than the WHO standard, suggesting polypharmacy risks. NSAIDs (19.81%) and antibiotics (17.43%) were the most commonly prescribed drugs. The average cost per prescription was NPR 456.23, while antibiotics averaged NPR 159.56. Only 23.38% of caregivers had complete knowledge of correct dosages. Conclusion. The study reveals acceptable prescribing patterns but indicates prevalent polypharmacy, with reliance on NSAIDs and antibiotics and limited caregiver knowledge of drug use. Addressing these issues through caregiver education, policy changes, and clinical pharmacy integration could enhance rational drug use and improve pediatric healthcare outcomes.
Keywords
Introduction
Pediatrics, a specialized field of medicine, focuses on the development, health, and medical conditions of children from infancy through adolescence. Children undergo rapid physical and cognitive growth, and their bodily systems, including organs, enzymes, and immune responses, develop at varying rates, rendering them uniquely susceptible to diseases and infections. 1 This is particularly true for young children, who frequently suffer from infections in the respiratory and gastrointestinal tracts. Respiratory infections, especially lower respiratory infections like pneumonia, remain a major concern, contributing significantly to morbidity and even mortality among children under 5 years of age. 2
Prescribing medications in pediatric populations requires careful consideration due to these developmental differences. The act of prescribing involves a healthcare professional, typically a physician, who assesses the patient’s condition, selects an appropriate therapy, and provides the necessary guidance for its use. 3 Effective prescribing ensures that children receive the right medications in appropriate dosages and formulations tailored to their specific health needs. Proper prescribing practices are essential not only for achieving positive health outcomes but also for minimizing adverse drug reactions and medication errors. 4
The concept of Rational Use of Drugs (RUD) underscores the importance of providing patients with medications that meet their clinical needs at doses appropriate to their unique requirements, for a suitable duration, and at the lowest possible cost. Unfortunately, irrational prescribing practices are prevalent worldwide, leading to unnecessary costs, adverse drug reactions, and an increased risk of drug interactions, which may result in prolonged hospital stays and even mortality. 5 The World Health Organization (WHO), in collaboration with the International Network for the Rational Use of Drugs (INRUD), developed a series of prescribing indicators to evaluate and promote rational drug use. These indicators assess various aspects of prescribing practices, including polypharmacy, the tendency to prescribe branded drugs, overuse of antibiotics, and inappropriate prescribing outside of essential medications lists. 6 WHO has released the “WHO Model Formulary for Children,” containing 240 essential medicines for treating illness in children based on global evidence. It contains standardized information on the recommended use, dosage, adverse effects, and contraindications of these medicines for use in children, so it helps rational prescribing. 7 Similarly, the British National Formulary (BNF) for Children is also another evidence-based formulary that provides up-to-date information on the use of medicines for treating children. 8 These guidelines provide clear direction on when medication is indicated and help prevent unnecessary or inappropriate use. For example, upper respiratory tract infections (URTIs) in children are among the most common health issues. 9 However, guidelines recommend against routinely prescribing antibiotics for acute coughs associated with URTIs, as these are typically caused by self-limiting viral infections.8,9 Antibiotics should only be prescribed in complicated cases, and even then, only after a thorough face-to-face clinical examination to assess the need for such treatment. 8
Studies on prescribing patterns are instrumental in evaluating the role and impact of drugs in healthcare, particularly in resource-limited settings. Monitoring prescribing patterns becomes even more critical in pediatric care, where antimicrobial agents are widely used to treat infectious diseases. 10 Excessive or inappropriate use of antibiotics, for instance, can contribute to the emergence of antibiotic resistance, a growing global health challenge. Research has consistently revealed that there is overprescribing of antimicrobials, 11 including in the pediatric population, where antimicrobial prescribing is higher than the WHO-prescribed standard. 12 This situation is more pronounced in developing countries like Nepal, where inappropriate prescription practices, limited diagnostic facilities, unauthorized sale of antimicrobials, inadequate patient education and non-compliance due to poverty and other factors like failure to take antimicrobials after symptoms subsides, and inappropriate self-medication predominates.6,13,14 Overprescribing of antimicrobials has contributed to the financial burden on the poor Nepali population, as well as antimicrobial resistance, and calls for antimicrobial stewardship, where the prescribing pattern research is a key source of information. Moreover, medications like paracetamol and ibuprofen, frequently used to manage fever in children, have shown potential associations with increased risks of conditions such as asthma and severe allergic reactions like anaphylactic shock when used without hypersensitivity reaction testing. 15 Similarly, aspirin has been associated with Reye’s syndrome in children suffering from chicken pox or influenza and Chloramphenicol with gray baby syndrome. 16
Nepal’s Drug Standard Regulations 2043 categorizes medicines into 3 groups: “Ka,” “Kha,” and “Ga.” Medicines in the “Ka” and “Kha” categories are intended to be sold and distributed only with a prescription from a registered physician, while “Ga” category medicines like paracetamol and ibuprofen are designated as over-the-counter (OTC) drugs that can be obtained without a prescription. 17 However, the implementation of these regulations remains inconsistent. For instance, even “Kha” category medicines, such as antibiotics, are often sold freely without having a prescription. 18 Unlike international practices, dispensed medicines in Nepal typically lack patient-specific labeling. 19 This forces patients or caregivers to rely on and recall verbal instructions provided by drug dispensers, increasing the risk of miscommunication and forgetfulness of instructions during medication administration. Although pharmacies are supposed to be operated by qualified professionals, such as licensed pharmacists, many are run by unauthorized professionals, resulting in substandard counseling and inadequate guidance for medicine use. 20 These challenges contribute significantly to medication errors and the irrational use of drugs, emphasizing the need for prescription pattern studies, strengthened prescription practices, comprehensive patient education, and regulatory enforcement to ensure safe and effective medicine use in Nepal.
Nepal faces significant challenges in its prescribing practices, including non-adherence to evidence-based medicine (EBM) and established guidelines, the use of medications without valid indications, irrational drug use, and therapeutic duplications. 14 These issues contribute substantially to drug therapy-related problems. Additionally, research on drug prescribing patterns within pediatric populations in Nepal remains limited, underscoring a gap in understanding medication practices and their impact on child health. The Nepal Demographic and Health Survey (NDHS) of 2016 reported that a significant proportion of children suffered from conditions like fever, diarrhea, and respiratory infections, underscoring the need for evidence-based, rational prescribing practices. 21 Addressing this knowledge gap is essential for improving healthcare delivery, ensuring access to appropriate medications, and optimizing treatment outcomes for children.
Limited studies have been done in Nepal to assess the prescribing pattern of antibiotics in pediatric hospitals, and they have revealed a high prescribing of antibiotics. However, no research has been conducted in Nepal till now to assess morbidity and prescribing patterns in pediatric outpatient departments. Moreover, previous studies on prescribing pattern of antibiotics did not assess cost analysis of prescription and caretaker knowledge of the method of drug use, which are important components of patient compliance and rational drug use. Therefore, this study aims to assess morbidity patterns and drug prescribing practices in the pediatric outpatient department of Kankai Nagar Hospital in Eastern Nepal. Additionally, the secondary objectives are to assess cost analysis of prescription and caretaker knowledge of the method of drug use. By examining prescribing patterns, this research seeks to provide insights into current practices, identify potential areas for improvement, and contribute to the development of effective, evidence-based healthcare strategies for pediatric patients in Nepal.
Method
Study Design, Study Setting, Sample Size, and Selection Criteria
A cross-sectional study was conducted in the Pediatric Outpatient Department at Kankai Nagar Hospital, located in Koshi Province, Kankai Municipality (Surunga-3), Eastern Nepal. The study population was pediatric patients visiting the pediatric outpatient department of Kankai Nagar Hospital for checkups and treatment. The study was carried out over a 1-month period, from May 21 to June 21, 2024. Kankai Nagar Hospital is a secondary-level healthcare facility that provides a range of services across various departments, catering to patients from surrounding areas. To calculate the sample size for the study, we used a prevalence-based estimate calculator, 22 aiming for a 95% confidence interval and a 5% margin of error. The estimated sample size was 245, considering a 20% prevalence of generic prescribing in previous studies. 23 Simple random sampling was employed using a computer-generated random number method to select eligible pediatric patients who met the study criteria. Children up to the age of 12 visiting the outpatient department were included, provided that their guardians or caregivers consented to participate. Children with severe or critical illnesses admitted to the pediatric ward and those whose caregivers did not consent were excluded from the study.
Procedure
Graduating pharmacists visited the Pediatric Outpatient Department at Kankai Nagar Hospital daily to gather information on pediatric patients registered for consultation with the attending physician that day. Each eligible pediatric patient was assigned a number, and a computer-generated random number was used to select the required number of participants for enrollment in the study. To minimize recall biases of knowledge on the method of drug use, data were immediately collected from enrolled patients and their caretakers after the pharmacy filled their prescriptions. A structured data collection form was used, which included a consent form, sections for socio-demographic information, and details of the prescribed medications.
A self-constructed patient profile form was utilized to record data on morbidity and drug prescribing patterns. This structured patient profile data collection form was designed by taking references from previous studies on similar topics.24,25 Relevant information was gathered from physical patient records, such as case sheets, outpatient department (OPD) prescriptions, and interviews. Any missing socio-demographic information and knowledge of drug administration techniques was collected through a questionnaire by interviewing the patients’ caregivers. Major diagnoses and prescribed drugs were categorized, and the cost of each prescription was calculated and recorded in the printed data collection form.
Data Analysis
The collected data were entered into Microsoft Excel for analysis. Descriptive statistics were used, with results presented as frequencies and percentages for categorical data, and mean values for continuous variables.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Institutional Review Committee of Purbanchal University School of Health Sciences (PUSHS-IRC) with reference number 056-080/081. Additionally, approval for data collection from Kankai Nagar Hospital was obtained from the hospital administration (Ref. no: 171). Participation in this study was voluntary, and written informed consent was obtained from the children’s caregivers or legally authorized representatives before data collection.
Results
Socio-Demographic Characteristics of Patients
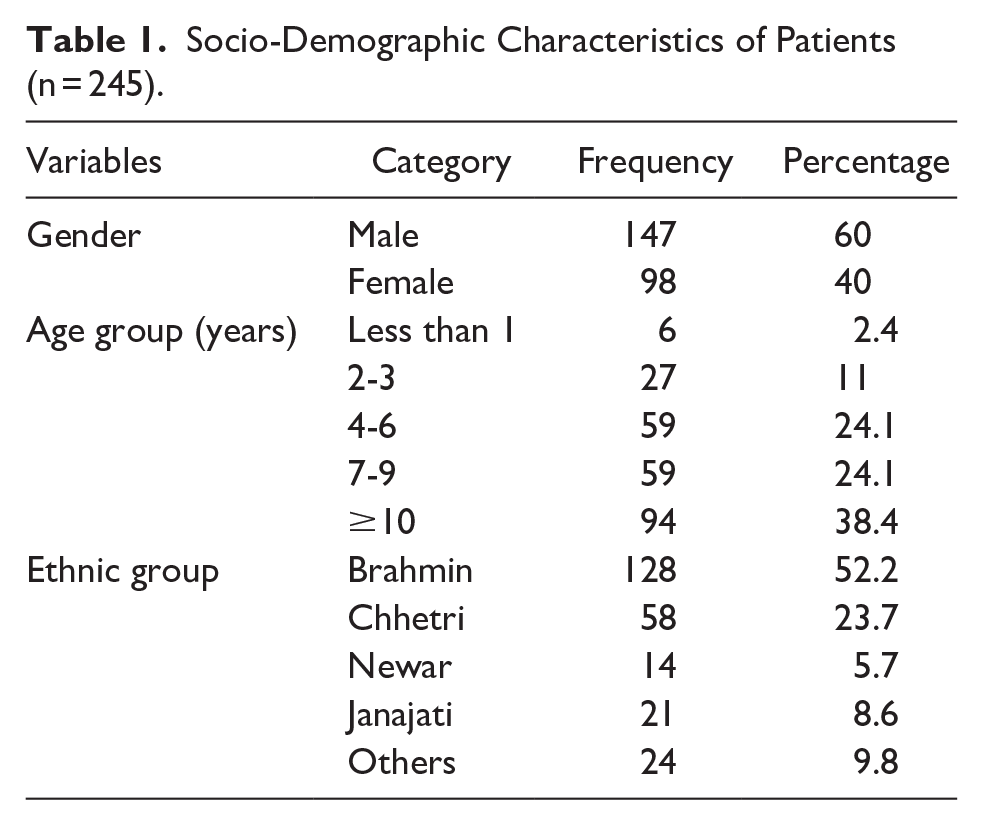
Out of 245 patients, 60% (147) were male and 40% (98) female. The age group with the highest proportion was 10 years and older (38.4%), followed by 4 to 6 years and 7 to 9 years (24.1% each), and 2 to 3 years (11%). The majority belonged to the Brahmin ethnic group (52.24%), followed by Chhetri (23.67%) and Janajati (8.57%), as shown in Table 1.
Socio-Demographic Characteristics of Patients (n = 245).
Major Diagnosed Disease in Pediatric Patients
The highest diagnosed disease was upper respiratory tract infection (26.5%), followed by conjunctivitis (12.2%), while the least common were acute gastroenteritis (1.6%) as shown in Table 2.
Major Diagnosed Disease in Pediatric Patients.

Others*: Otitis media, impetigo, anxiety, scabies, polyurea, dental caries, head itching, floppy syndrome, back pain, intra-abdominal lymphadenopathy, diarrhea, cellulitis, epididymitis, hypocalcemia, cut injury.
Therapeutic Category of Drug Prescribed and Classification
The most prescribed therapeutic category was autacoids and related drugs, which consists of NSAID and Antihistamines (33.81%), followed by antimicrobial agents (20.60%), while the least prescribed were respiratory drugs (4.49%), as shown in Table 3. The average number of drugs prescribed per patient encounter was 3.08.
Therapeutic Category of Drug Prescribed.

Miscellaneous*: Carboxymethylcellulose, steroids, povidone iodine, permethrin, electrolytes, serratopeptidase, trypsin- chymotrypsin (chlorhexidine + metronidazole + benzalkonium chloride + triamcinolone).
In the classification of therapeutic drugs, NSAIDs were the most commonly prescribed under autacoids (58.59%), antibiotics dominated the antimicrobial agents category (88.46%), and among gastrointestinal drugs, H2-blockers were the highest (30.95%) as shown in Table 4.
Classification of Therapeutic Category of Drugs.

Total Cost Analysis of Prescription and Antibiotics
In the cost analysis of prescriptions, most prescriptions (64.08%) fell below NPR 500, followed by 29.38% in the NPR 500 to 1000 range, while only 0.40% exceeded NPR 2000 as shown in Table 5.
Total Cost Analysis of Prescription.

In the cost analysis of antibiotics, the majority of prescriptions (75.42%) were in the NPR 100 to 500 range, followed by 19.49% in the NPR 501 to 1000 range, with only 1.69% costing above NPR 1000 as shown in Table 6. The average cost of antibiotic per prescription was NPR 159.56.
Total Cost Analysis of Antibiotics.

Patient or Caretaker Knowledge of Method of Drug Use
In the analysis of patient or caretaker knowledge of prescribed drug use, 23.38% had complete knowledge of the correct dosage regimen information, and 69.08% knew when to take the medication. Conversely, 76.61% were unaware of the correct dosage, and 30.91% lacked knowledge of the appropriate timing as shown in Table 7.
Patient or Caretaker Knowledge of Method of Drug Use.

Discussion
The primary goal of this study was to evaluate drug prescribing patterns in the Pediatric Outpatient Department of Kankai Nagar Hospital, Eastern Nepal, to promote rational drug use and improve healthcare efficiency and cost-effectiveness. Through this analysis, we identified various deficiencies in current prescribing practices, highlighting areas for improvement that can contribute to a more rational and economical healthcare system.
In our study, 60% of the pediatric patients were male, aligning closely with findings by Shakya and Shrestha, 26 where 69% of pediatric patients were male. This gender distribution suggests a similar trend in healthcare-seeking behavior across different regions.
The average number of drugs prescribed per patient encounter in our study was 3.08, an indication of polypharmacy in pediatrics population, though it is lower than that reported in Western Nepal (6.12) 27 and South India (4.56), 28 yet higher than values from other regions of Nepal, such as Central Nepal (2.81). 29 The World Health Organization (WHO) recommends an average of less than 2 drugs per encounter to minimize the risk of adverse drug interactions, cost, and antimicrobial resistance. 30 Reducing the average number of drugs per encounter in our setting could help address these issues by improving patient adherence and decreasing the likelihood of negative health outcomes due to polypharmacy.
Upper respiratory tract infections (URTI) were the most common diagnosis in our study (26.5%), consistent with findings by Gedam et al, 31 who reported URTI as the leading diagnosis in pediatric patients (50.07%), and Malpani et al, 32 who also identified URTI as the most prevalent illness (25.58%). These findings emphasize that respiratory infections remain a significant health concern among children in various settings, influenced by environmental and infectious factors such as exposure to pollutants and viral and bacterial infections. This pattern indicates a need for targeted interventions to reduce respiratory infections in children, possibly through public health campaigns addressing environmental risks and vaccination initiatives.
In terms of drug prescriptions, NSAIDs were the most commonly prescribed category (19.81%), followed by antibiotics (17.43%) and H2-blockers (3.43%). Our findings are in line with studies conducted by Antony et al, 33 and Gedam et al, 31 which also reported NSAIDs and antibiotics as the most frequently prescribed drugs in pediatric settings. The high prescription rate of NSAIDs and antibiotics suggests a reliance on these drugs for symptomatic relief and infection control, respectively. Considering the international scenario, for example, studies in Italy show that there has been an overall decrease in antibiotic prescriptions over the years in the pediatric population. 34 However, our studies show higher reliance on antibiotics, and this reliance raises concerns about potential overuse, particularly of antibiotics, which could lead to antimicrobial resistance. Rationalizing antibiotic use and ensuring adherence to guidelines for infection control is essential to mitigate these risks.
The average cost of drugs per prescription in our study was NPR 456.23 (USD 3.40), while the average cost for antibiotics was NPR 159.56 (USD 1.18). These costs are comparable to findings from Pokhara, Western Nepal, where the average prescription cost was USD 2.75. 35 However, these values are substantially lower than costs reported in higher-income countries, such as China, where the average cost of drugs per visit was USD 13.84. 36 The cost discrepancy can be attributed to income levels and healthcare system differences between low- and high-income countries. Despite lower prescription costs than developed countries, there remains a need to ensure cost-effective prescribing practices to alleviate the financial burden on low-income families since research has demonstrated that improper antibiotic prescriptions are frequently observed in pediatric patients, leading to a heightened risk of adverse drug reactions and increased healthcare costs associated with these treatments. 37
Only 23.38% of parents or caregivers had complete knowledge of the correct dosage for the prescribed medications, and 69.08% understood when to administer the drugs. This knowledge level is significantly lower than that reported by Pise et al, 38 where 59% of caregivers had adequate knowledge of drug use. The gap in caregiver knowledge in our study could be due to the rural, low-literacy population frequently attending the hospital. Implementing educational interventions and patient counseling could help improve caregiver understanding of medication use, ultimately enhancing adherence and treatment outcomes for pediatric patients.
Our study highlights several areas for improvement in pediatric prescribing practices. Addressing issues such as polypharmacy, high reliance on NSAIDs and antibiotics, and caregiver education gaps can contribute to a more rational, cost-effective healthcare system.
Strengths and Limitations
One of the study’s strengths is its use of a structured and comprehensive approach to analyze drug prescribing patterns and morbidity in pediatric patients at Kankai Nagar Hospital in Eastern Nepal, offering valuable insights into pediatric healthcare practices in a resource-limited setting. Additionally, the study’s focus on both prescribing trends and caregiver knowledge provides a holistic view that can inform targeted interventions to improve rational drug use in pediatric populations. However, this study has certain limitations, including its single-center design, which may limit the generalizability of findings to other healthcare settings. Furthermore, the 1-month study period may not adequately account for seasonal variations in disease prevalence and drug prescriptions. Finally, the reliance on hospital records and caregiver interviews may introduce information and recall bias, as these sources may not fully capture all relevant patient information.
Conclusion
This study highlights the prescribing patterns and morbidity in pediatric patients at Kankai Nagar Hospital, Eastern Nepal, emphasizing the need for improved rational drug use in this population. The analysis reveals significant areas of improvement, such as reducing polypharmacy, rationalizing antibiotic use, and enhancing caregiver knowledge regarding medication administration. The high prevalence of upper respiratory tract infections and the frequent prescription of NSAIDs and antibiotics underscore the importance of targeted health interventions and adherence to prescribing guidelines. Addressing these issues can contribute to a more efficient, cost-effective healthcare system, ultimately benefiting pediatric patients and promoting better health outcomes. Continued efforts toward educating healthcare providers and caregivers, along with implementing evidence-based prescribing practices, are essential steps toward achieving rational drug use in pediatric healthcare.
Recommendation for Policy, Practice, and Educators
Policy
To promote rational drug use in pediatric care, health authorities should enforce policies that prioritize rational prescribing practices and patient education, particularly for antibiotics and NSAIDs. Regulatory bodies should mandate periodic audits of prescribing patterns in pediatric departments to identify and address irrational prescribing behaviors, thus improving patient outcomes and reducing healthcare costs.
Practice
Hospitals should integrate clinical pharmacists into pediatric outpatient departments, and patient-specific labeling in dispensed medicines should be practiced to enhance medication safety and optimize drug therapy. Clinical pharmacists can play a vital role in counseling caregivers on medication use, especially regarding dosage and timing, thereby improving caregiver knowledge and adherence. Additionally, healthcare providers, especially pediatrics physician, should be trained regularly on Standard treatment guidelines and the use of pediatrics formulary and other WHO guidelines and should focus on reducing polypharmacy by prescribing the minimum necessary drugs, aligning with WHO standards for drug use.
Educators
Pharmacy and medical education programs should incorporate modules focused on rational drug use, particularly in pediatric pharmacotherapy. Practical training and internships in pediatric settings should emphasize patient counseling, drug interaction awareness, and evidence-based prescribing practices to ensure future healthcare providers are equipped with the skills necessary for promoting safe and effective medication use in pediatric populations.
Footnotes
Acknowledgements
The authors sincerely thank Kankai Nagar Hospital for their unwavering support and cooperation during the data collection. We would also like to acknowledge the invaluable assistance the Purbanchal University School of Health Sciences provided throughout this study.
CRediT Authorship Contribution Statement
Data Availability Statement
The datasets used and analyzed during the study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent of Publication
All the authors in this study have consented to the publication of this study.