
Abstract
Introduction. Neonatal mortality, the death of infants within 28 days, is a major challenge for healthcare in developing countries. Despite global declines, data on rural patterns remain scarce. Objective. To determine neonatal mortality trends and factors in rural Ethiopia. Methods. The Ethiopian Demographic Health Survey (EDHS) conducted cross-sectional studies in rural Ethiopia in 2011, 2016, and 2019. Consenting women who gave birth in these years were included. Data were analyzed with STATA 17 using multistage cluster sampling, logistic regression, and weighted estimates. Results. Data from 22 755 women showed neonatal mortality rates dropped from 7.5% to 6.03%. Gambela and Tigrai had the lowest rates, while Dire Dawa and Somali regions had higher rates. Key factors included mother’s age, wealth, birth order, sex, twins, breastfeeding, and baby’s size. Conclusion. Despite decreases, challenges persist. Regional health bureaus should enhance antenatal care and promote facility births.
Introduction
Neonates are newborns up to 28 days old.1,2 Neonates can be classified by gestational age, birth weight, and based on the combination of gestational age with birth weight. 3
Neonatal death is a serious problem that occurs within the first 28 days of life due to various factors, which can be from prenatal, intra-natal, or post-natal driven causes.4,5
Neonatal mortality is commonly expressed as the number of deaths during the first 4 weeks of life per 1000 live births within a given time frame. Based on the time of death, neonatal mortality can be subdivided into very early (<1 day), early (1-7 days), and late neonatal deaths. 6
The neonatal mortality rate is highest within the first 7 days of life, with 75% of deaths occurring during that time. Roughly 1 million neonates die within 24 hours of birth. Preterm-related complications, perinatal complications, and infections are the leading causes of neonatal mortality.5,6
The 3 major causes of neonatal deaths globally are infections (36%), pre-term delivery (28%), and birth asphyxia (23%). 7 Africa loses 1.12 million neonates yearly due to preventable causes, including prematurity, low birth weight, infections, lack of oxygen, and birth trauma. 8
In 2021, 2.3 million children died in the first month of life worldwide or approximately 6400 newborns per day. The annual death toll could reach up to 2.5 million, mostly in low- and middle-income countries (LMICs), where basic human rights are often ignored.9,10 Of the total global neonatal mortality, 80% occurred in Sub-Saharan Africa and Southern Asia, with two-thirds of deaths happening on the first day of life and 3-quarters within the first 7 days. The place of neonatal birth significantly impacts survival, with mortality rates being 20 times higher in Sub-Saharan Africa and Southern Asia, and even higher for newborns during conflicts. 9
The burden of neonatal mortality is not limited to the neonates themselves but has multilevel effects on a country’s profile, family spiritual life, family health, family social relations, and family economy. It can also cause divorce among partners due to blame, mistreatment, and dishonor.11,12 Neonatal mortality is a painful experience that can cause parental psychosocial problems, which may result in family members contemplating or committing suicide. 11
Professionals who work in neonatal intensive care units are more likely to be present during the end-of-life time for neonates, which can hurt their emotions and practice. Coping with the death of newborns is a highly stressful task that can lead to post-traumatic stress symptoms and burnout in professionals. 13
The Sustainable Development Goals (SDG) aim to end preventable deaths of newborns and children under the age of 5 by 2030. All countries should strive to reduce newborn mortality to at least 12 deaths per 1000 live births and under-five mortality to at least 25 deaths per 1000 live births. However, in rural Ethiopia, the neonatal mortality rate is still very high, standing at 62 deaths per 1000 live births. This is significantly higher than the SDG targets. 14
Based on current trends in neonatal mortality, it is projected that 1.8 million neonates would die in 2030. However, if each country achieved the SDG targets, there would be about 1.2 million neonatal deaths. Achieving this goal requires increased efforts to enable continued improvements in child survival. 15
The study conducted in China showed that neonatal mortality had steadily decreased from 5.9 deaths per 1000 live births in 2014 to 3.9 deaths per 1000 live births in 2018, which was lower than the target of SDG at the national level. 16 The systematic review conducted in Brazil showed that the average neonatal mortality rate was 9.46 deaths per 1000 live births in 2017, with a reduction of 2.15% between 2007 and 2017. 17 In the systematic review of Southeast Asian countries, Indonesia had the highest neonatal mortality rate, with 61 deaths per 1000 live births in 2017. This trend decreased gradually from 103 per 1000 live births in 2000. 18 In Nepal, although neonatal mortality is decreasing, if it continues at the current rate, it will take another 50 years for the country to attain the 2030 SDG target. The neonatal mortality rate declined by an average of only 4.0% between 2001 and 2016. 19
In Ghana, there has been a steady decline in neonatal mortality from 30 per 1000 live births in 1998 to 25 per 1000 live births in 2017 for all births. 20 In Burundi, the NMR declined from 38.7 per 1000 live births in 2010 to 25.0 deaths per 1000 live births in 2016, respectively. The richer wealth quintile has slightly higher NMR than other parts of the country. 21 The review results conducted in Kenya showed that the neonatal mortality rate has fallen gradually from 35.4 deaths per 1000 live births in 1975 to 19.6 deaths per 1000 live births in 2018. 8
In Ethiopia, the neonatal mortality rate declined logarithmically by 1.9% per annum from 1995 to 2010. 7 However, neonatal death rates climbed from 29 per 1000 live births in the Ethiopian Demographic Health Survey (EDHS2016) to 30 per 1000 live births in the Ethiopian Mini Demographic Health Survey (EMDHS 2019) report.7,21 -23 Despite its increment, there are significant variations across specific regions of the country. For instance, in the Somalia region, around 130 newborns do not survive beyond the first week of life, the estimated NMR is 54 per 1000 live births in Oromia and 46 per 1000 live births in the Amhara region. Ethiopia’s progress was slow, and it fell well short of the UN’s ambitious aim of avoiding unnecessary infant deaths and lowering neonatal mortality to 12 per 1000 live births in every nation by 2030. 22
Male neonate had a higher likelihood of dying in the first 4 weeks of life when compared to their female neonate. This finding was consistently found in the study conducted using DHS data in Zambia, 24 Afghanistan, 25 Nigeria, 26 Burundi, 21 and Bangladesh. 27
Studies have shown that extending the interval between pregnancies to more than 24 months positively impacts neonatal survival. A study using DHS data in Nepal found that birth intervals shorter than 24 months significantly predict neonatal mortality. 20 In Zambia, ZDHS data showed that longer birth intervals are linked to lower neonatal mortality. Similarly, EDHS 2016 data from Ethiopia found that children born after intervals greater than 24 months had a higher chance of surviving the neonatal period.20,25
Multiple pregnancies are classified as high-risk births due to higher fetal and neonatal complications compared to singletons. This finding is supported by a DHS study in Ghana, 20 Afghanistan, 25 and Ethiopia. 7 A study in Afghanistan found that maternal ages below 18 and above 35 are linked to higher neonatal mortality compared to ages 20-30. 25
A retrospective cohort study in Brazil 17 found that neonates born to first-time mothers had higher chances of dying compared to those born to multiparous mothers. Contradicting this, a DHS study in Ghana found that high parity was linked to higher neonatal mortality. 20
A study using DHS data from Ghana found that mothers who did not attend ANC had a 5 times higher risk of neonatal mortality compared to those who did. This finding was consistent in studies from Afghanistan, Nigeria, and Ethiopia.7,25,26
A study in Zambia found that children born to mothers using contraceptives were 66% more likely to survive compared to those born to mothers not using contraceptives. 28 In a longitudinal study in Northwestern Ethiopia, mothers using contraceptives were 2 times less likely to lose a child compared to those not using contraceptives, consistent with the previous study. 20
Neonatal mortality remains a significant issue, especially in rural Ethiopia, where access to specialized facilities is limited. This study aims to analyze EDHS data from 2011 to 2019 to understand trends and factors contributing to neonatal mortality in these areas.
Materials and Methods
Study Area, Design, and Period
A community-based cross-sectional study was conducted on the rural population across all administrative regions of Ethiopia by the EDHS program in 2011, 2016, and 2019.
Participant’s Selection and Exclusion
The inclusion and exclusion criteria are crucial in defining the study population and ensuring the analysis focuses on relevant data. In the context of neonatal mortality analysis using EDHS data, these criteria ensure that the dataset is comprehensive, representative, and pertinent to the research objectives.
Source Population
All women of reproductive age living in rural Ethiopia during the EDHS surveys of 2011, 2016, and 2019 were considered as the source population.
Study Population
All pregnant women residing in rural areas of Ethiopia during 2011, 2016, and 2019, as recorded in the Ethiopian Demographic and Health Surveys (EDHS), were included as the study population.
Sample Size Determination and Sampling Techniques
All pregnant women who gave birth in rural Ethiopia during 2011, 2016, and 2019 were included in the Ethiopian Demographic and Health Surveys (EDHS). Households were selected via multistage cluster sampling to include pregnant women who gave birth and volunteered to participate in the study.
Study Variables
Neonatal mortality is defined as the death of a newborn within the first 28 days of life, as reported by the Ethiopian Demographic and Health Survey (EDHS). It is considered a dependent variable in this study. The independent variables that were considered in the study were age, region, altitude, religion, education, marital status, household access to media, source of drinking water, type of toilet facility, type of cooking fuel, wealth index of the household, number of living children, birth order number, number of antenatal visits, whether the child is a twin, sex of the child when it is put to the breast, place of delivery, delivery by cesarean section, and size of the child at birth.
Data Quality Assurance
The data was extracted from the EDHS website after getting formal permission to access the data for research purposes only. Then the required data is meticulously exploited for the analysis and it was analyzed carefully using software and the data were also checked for missing values.
Data Processing and Analysis
The neonatal mortality data from the DHS are analyzed using frequencies, percentages, cross-tabulations, and multiple logistic regression statistical methods, taking into account the complex survey design. Weighted estimates are produced to generate population-level statistics.
Multiple logistic regression analysis was utilized, with neonatal mortality coded as 0 and 1. A code of 0 indicates that the outcome of interest died, while a code of 1 indicates the absence of the outcome of interest, meaning the subject is alive.
After a result from the logistic regression model with a logit link function, computing a marginal effect or risk difference often has numerous advantages as it estimates a percentage point change, not a percent change. As we add more variables to the model, the marginal effects are not sensitive, and they remain unchanged. To compute the marginal effects, the change in probability when the discrete value of 1 of the independent variable changed is calculated.
Among the various logistic regression model fit assessment criteria, the commonly used measures, such as the Hosmer-Lemeshow test, the link test, the receiver operating characteristic (ROC) curve, pseudo R-squared, Residual Analysis, and outlier detection were used. All analyses were performed with Stata v. 17.
Data Collection Techniques
Data were extracted from the Ethiopia Demographic and Health Surveys (EDHS) conducted in 2011, 2016, and 2019 based on the outcome of interest, neonatal mortality. A request to EDHS was made on Jan 15, 2024, to access the data for research purposes and we obtained the data on date Jan 16, 2024, with an affirmation letter from the EDHS team. The DHS employed a multistage cluster sampling design to select households for participation. The authors got permission to access the EDHS data from the ICF-DHS program. 29
Results
Background Characteristics
Out of the 22 755 participants, the majority of data (9663 or 42.5%) were obtained from the 2011 EDHS, followed by 8667 (38.1%) from the 2016 EDHS. In terms of altitude, many participating neonates (9699 or 42.6%) were from altitudes between 1501 and 2300 m, while 7515 (33%) were from altitudes between 501 and 1500 m. That means more than 75% of the EDHS data on neonatal mortality used for this study were obtained from a cluster at an altitude of 501 to 2300 m. Geographically, the DHS data used for this study were extracted from the rural distribution of all regions. Oromiya (16.4%), SNNPR (Southern Nations Nationalities Peoples’ Region; 14.5%), Amhara (11.2%), Afar (11.0%), and Somali (10.93%) regions tend to have a higher number of neonate participants in the study compared to the other rural regions. A smaller number of neonatal deaths in rural areas of Dire Dawa city administration and Harari region were included (4.1%, and 4.8%, respectively; Table 1).
Demographic Characteristics and Determinants of Neonatal Mortality Trends in Rural Ethiopia, EDHS 2011, 2016, and 2019; N = 22 755.

Among the 15 623 mothers, 68.7% have 3 or more living children, while 7132 (31.3%) have fewer than 3 living children. The age distribution of the mothers was examined, revealing a predominantly adult demographic profile. The majority of individuals fell within the 25 to 34 age range, constituting 11 599 (51%) of the total population. The income distribution analysis demonstrated significant heterogeneity among the participating mothers. The majority of respondent mothers, 14 050 (61.7%), indicated a poor wealth index, while 4683 (20.6%) and 4022 (17.7%) of mothers reported a rich and middle wealth index, respectively. Disparities in the number of antenatal care service visits during pregnancy were also observed among mothers.
While 50.1% of the women did not attain the optimal number of ANC service visits—at least 4 ANC visits—it has been reported that the attendance status of more than one-third of the mothers, 34.5%, was not reported. Only 15.4% of the mothers were reported to have attained the optimal level of at least 4 ANC visits. The marital status of mothers indicates that the majorities of them (94.2%) are married and live with their husbands. Examining educational attainment levels reveals that a substantial portion of the participating mothers (72.0%) had no formal education. The distribution of religious affiliations of mothers in the study was analyzed, and Muslims were found to be the largest group, followed by Orthodox religion (Table 2).
Maternal Background Characteristics and Determinants of Neonatal Mortality Trends in Rural Ethiopia, EDHS 2011, 2016, and 2019; N = 22 755.

Household and Health Service Related Characteristics
In this study of households’ access to facility characteristics, we found that 15 715 (69.1%) of mothers use unprotected sources of drinking water, 12 989 (57.1%) do not access toilet facilities, while the remaining 7040 (30.9%), and 9766 (42.9%) of rural mothers access protected drinking water and toilet facilities, respectively. The summary table also reveals that more than half of the surveyed population (69.6%) did not have access to television and radio. More than 90% of these mothers use wood as fuel for cooking and other activities. Access to facilities such as protected sources of drinking water, utilization of toilet facilities, access to the media, and use of electricity for cooking and food preparation as fuel are likely to support mothers and childcare, implying a decrease in infant mortality (Table 3).
Facility Accessibility Characteristics and Determinants of Neonatal Mortality Trends in Rural Ethiopia, EDHS 2011, 2016, and 2019; N = 22 755.

Neonatal and Delivery Related Characteristics
As depicted in the table below, 51.4% of the children in the sample are male, while 48.6% are female. The distribution of neonatal mortality status in rural areas, based on the 2011, 2016, and 2019 EDHS data, revealed that 6.9% of the neonates in the sample died, while 93.1% survived. This provides insight into the mortality rate among neonates in the studied population. The status of the infant regarding the time she or he started breastfeeding was analyzed and found that 59.5% of the children were put in the breast immediately after birth, while 40.5% were not. The distribution of child sizes at birth was also another variable of interest, which shows that 23.9% were classified as large, 31.9% as average, and 24.8% as smaller. Additionally, 19.4% have an unknown size (Table 4).
Neonatal and Maternal Related Characteristics for Trends and Determinants of Neonatal Mortality in Rural Ethiopia, EDHS 2011, 2016, and 2019; N = 22 755.

The majority of neonates in the study were reported to be single births (97.1%), and only 2.9% were multiple births (twins). The place of neonate delivery was also a study variable, revealing that 81.3% of the deliveries occurred at home, while the remaining 18.7% took place in a health facility. Substantial types of deliveries encompassed in the study were vaginal deliveries, 98.7%. Only 1.3% of the deliveries were by cesarean section (Table 4).
Trends of Neonatal Live Status in Rural Areas
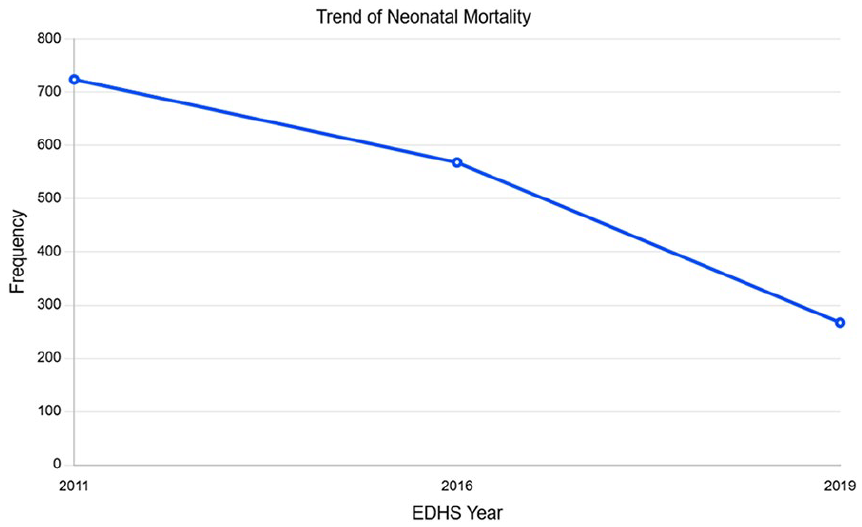
There is a notable disparity in neonatal mortality status across the EDHS years. The 2011 DHS encountered the highest number of neonatal deaths, 724 (7.5%), followed by the 2016 DHS with 568 (6.6%). In the 2019 DHS data, the fewest number of neonatal deaths was recorded. This implies that the risk of neonatal mortality in rural Ethiopia is decreasing. This decrease in neonatal mortality rates across the DHS years in rural Ethiopia is displayed in the figure below (Figure 1).
Trends of neonatal mortality and determinants of neonatal mortality in rural Ethiopia, EDHS 2011, 2016, and 2019; N = 22 755.
While observing data on total mortality in different regions of Ethiopia across the years 2011, 2016, and 2019, as recorded in the Ethiopian DHS (Demographic and Health Survey), the total mortality rate in Tigray decreased from 6.7% in 2011 to 3.6% in 2019. The total mortality rate in Afar also decreased, from 8% in 2011 to 4.4% in 2019. Similar trends were observed in other regions, with a decrease in total mortality rates from 2011 to 2019, indicating potential improvements in child health and healthcare services.
Total mortality rates vary between regions and across survey years. In 2019, as an illustration, the regions with the lowest mortality rates include Gambela (3.8%) and Tigray (3.6%), while the highest mortality rates are observed in Dire Dawa (4.4%) and Somali (4%).
While the general trend indicates a decline, there are regional variations in the pace and magnitude of this decline. Some regions show more significant reductions in neonatal mortality rates compared to others. For example, regions like Amhara, Benishangul Gumuz, SNNPR, and Dire Dawa exhibit consistent decreases in mortality rates over the years, indicating successful interventions or improvements in healthcare infrastructure and services. On the other hand, regions like Afar, Somali, Gambella, and slightly Oromiya may show less pronounced declines or even fluctuations in neonatal mortality rates, suggesting potential challenges or disparities in healthcare access or quality. This comparison provides insights into how each region fares compared to the national average.
Factors Associated Neonatal Mortality in Rural Ethiopia
Displayed in this table are the logistic regression results pertaining to neonatal mortality, with the categorization of 1 for death and 0 for survival, and its relationship to various independent variables. Notably, the results reveal a significant negative correlation between the Ethiopian DHS years and the probability of neonatal mortality.
A comparison of data, from Ethiopian Demographic and Health Surveys (EDHS) in 2011, 2016, and 2019, shows that neonatal mortality is decreasing over time. Neonates surveyed in 2016 were 13% less likely to die compared to those in 2011, while newborns in 2019 were 34% less likely to die than those in 2011. The age of the mother is also a significant factor. Neonates born to mothers aged 25 to 34 years were 14% less likely to die than those born to mothers aged less than 25 years. No significant association was found for mothers aged 35 to 49 years. The study found that neonatal mortality is negatively correlated with the rich wealth index. The odds ratio was 0.84 (P = .00), meaning that a child born to a wealthy mother has a 16% lower chance of dying compared to a child born to a poor mother. Families with 3 or more living children have 88% lower odds of neonatal mortality than families with less than 3 living children, according to the study. The adjusted odds ratio was 0.12.
The study examined the impact of birth order on the likelihood of neonatal death, dividing it into 3 categories: first order, second to fourth order, and more than fourth order. The results revealed that both second to fourth-order and above-fourth-order were statistically significant predictors of neonatal death, with infants after the first birth order exhibiting a significantly higher likelihood of death compared to the first birth order. Specifically, neonates in the 2 to 4 birth order have approximately 180% times higher odds of death when compared to the first birth order, holding constant the effect of other variables in the model. A study found that neonates born at higher birth orders have significantly higher odds of death. Infants from multiple deliveries are more likely to die compared to singleton deliveries. The gender of a newborn was found to have a significant effect on their likelihood of survival. Female infants were 20% less likely to die compared to male infants (OR = 0.80, P = .00). The time of breastfeeding after birth was also analyzed, and it was found that immediate breastfeeding was significantly associated with a 99% decrease in the odds of death compared to delayed breastfeeding at birth (OR = 0.01, P = .00), while other factors were held constant. These findings indicate a strong relationship between neonatal mortality and delayed breastfeeding after birth in rural areas among the population surveyed. Furthermore, the odds of neonatal death were 35% lower for mothers who utilized optimal antenatal care service visits compared to those who did not attend these visits (OR = 0.65, P = .00).
The model includes the size of the baby at birth, and it shows that babies born with a medium size have a significant negative association (OR = 0.75, P = .00), while babies born with a smaller size do not have a significant association. This means that babies born with a medium size are 25% more likely to die than babies born with a large size.
The model’s McFadden’s R square value is .2098, indicating that the independent variables included in the model account for approximately 21% of the variance in neonatal mortality. In addition, the model has a relatively good fit to the observed data, as the log-likelihood is −5670.54. The link test with a P-value of .1369 suggests that there is no strong evidence of a lack of fit, and the overall model fits statistically significantly (Table 5).
Multiple Logistic Regression Results Predicting Neonatal Mortality in Rural Ethiopia, EDHS 2011, 2016, and 2019; N = 22 755.

Abbreviations: B, unstandardized coefficient; SE, standard error; Wald, Wald statistic; OR, odds ratio.
P < .05.
Discussion
This study was conducted to examine trends and determinants of neonatal mortality in rural areas of Ethiopia by using the Ethiopian demographic health survey in 2011, 2016, and 2019.
In rural Ethiopia, trends of neonatal mortality from 2011 to 2016 decreased from 7.5% to 6.6%, unlike the very slow decline from 2016 to 2019, which was only 6%. This might be because Ethiopia has implemented ANC, postnatal care, immunization during and after pregnancy, the birth corner, basic life support, and birth attendance skills during the period before 2016. 30 This doesn’t mean that Ethiopia is not working with the listed strategies from 2016 to 2019 and till now, but the level of focus is different. This means the implementation of the strategies in rural areas of Ethiopia might be decreased due to give-back services, which may increase neonatal mortality.
However, regions such as Afar, Somali, Gambella, and, to a lesser extent, Oromia may exhibit less pronounced reductions or even fluctuations in neonatal mortality rates. This variation could indicate potential challenges or disparities in healthcare accessibility and quality within these areas. Factors contributing to these regional discrepancies could be limited healthcare infrastructure, socio-economic barriers, cultural practices, and the remoteness of certain locations.
From the multiple logistic regression, neonates included in the 2016 EDHS are 14.8% (CI: 0.283-0.037) less likely to die compared to those included in the 2011 EDHS. Here, the analysis shows that time has its effect on neonatal mortality, which could be defined by different factors such as the modernization and emergence of neonatal devices, scientific evidence, and the use of neonatal-trained human resources that interns used to give more qualified neonatal care that decreased the death rate. However, the probability of death among neonates included in the 2019 EDHS was 34.6% (CI: .602, .248) lower than neonates included in the 2016 EDHS. This finding shows that the probability of death over the recent period is lower, but there is a significant difference in each comparison EDHS period. Institutional level readiness differences during each period, the availability of neonatal intensive care units in most hospitals, and cultural issues that claimed that neonatal deaths were considered a secret and nothing or some bad punishment from the creator of the people that collectively affect the care of neonates that ends with death. 31 This justification works since the attitude, infrastructure, and multiple issues have been fixed from ancient to recent times. However, there is still a breakup to sustain the decrease in neonatal mortality from 2011 to 2016 and 2019 EDHS.
This study identifies that being born from a wealth index (rich) family decreases the probability of neonatal death by 20.8% (CI:0.394,0.073) compared to their counterparts. This finding is similar to studies conducted in South Asia, 32 Ghana, 33 and in Ethiopia. 34 The possible justification could be that factors contributing to the high neonatal mortality rate in poor families might be the lack of access to quality healthcare, maternal malnutrition, which may cause complications, inadequate sanitation, and living conditions, which may increase maternal infection, and limited education and awareness about the dangers of pregnancy.
Neonates from a family with a living child of 3 or more have 88% (CI: 10, 0.15) less chance of death than those found with less than 3. The possible justification could be due to limited resources; families with fewer members may have limited financial resources and access to healthcare services; mothers with lower family sizes may be younger; and young mothers often face increased risks during pregnancy and childbirth, which could boost neonatal mortality. However, this finding from this study is contrary to the conclusion reported by the study conducted in Ethiopia using the 2019 EDHS. 35
Neonates with birth order 2 to 4 and >4 order has a 2.80 (CI: 2.34, 3.34) and 6.39 (CI: 4.97, 8.21) times risk of death compared with birth order 2 and less. This finding is almost similar to the study conducted in Ethiopia.35,36 The possible justification for this finding could be due to increased maternal age, which can be accompanied by different neonatal complications secondary to maternal health, including prematurity.
The odds of neonatal death in twin or multiple pregnancies are 3.8 times (CI: 3.13, 4.69) higher than in singleton pregnancies. The finding of this study is in line with previously conducted studies in Ethiopia. 33 This can be attributed to the high risk of preterm birth, small gestational age, low birth weight, and intrapartum anoxia associated with twin pregnancies, which individually or collectively contribute to neonatal mortality. 35
Based on the findings of this study, female neonates are 20% (CI: 0.72, 0.89) less likely to die compared with male neonates. This conclusion is in agreement with various other studies.7,29 The possible justification for this finding might not be biologically sound, despite different methodological and birth prevalence differences between the 2 sexes.
The preventive effects of early breastfeeding initiation among neonates is 99% ( CI: 0.01, 0.02) compared with neonates with delayed breastfeeding initiation. This finding agreed with different previous studies.29,32,33 This might be due to multiple uses of the first vaccine (breast milk) which protects the newborn from acquiring infection, decreases complications, and reduces newborn mortality.
In this study, optimal antenatal care has a positive association with neonatal mortality, which decreases the risk by 34% (CI: 0.53, 0.82), whereas unknown or no antenatal care increases the probability of neonatal death by 1.32 times (CI: 1.17, 1.50) compared with neonates born to mothers having regular ant-natal follow-up care. This finding is comparable with the previous studies.30,34,35 This finding is supported by scientific evidence in which antenatal care is intended to ensure that a woman has a safe pregnancy and allows screening of preeclampsia, fetal abnormalities, and other prevention strategies to be incorporated. As a result, early identification and management will be applied, which can decrease neonatal mortality. 37
The probability of neonatal death from a probability family of average child size is 25% (CI: .65, .87) less than neonates from a large family size. This finding is also in line with previously conducted studies.5,30,36 This might be due to the larger the family, the less economical it may be to serve the family, especially the pregnant mother with her fetus, resulting in different perinatal complications and a poor neonatal outcome, especially in rural areas.
Study Limitation
The results from the cross-sectional study reflect only one moment in time, making it impossible to analyze cause-and-effect relationships.
Conclusions
Regions such as Amhara, Benishangul Gumuz, SNNPR, and Dire Dawa have displayed consistent decreases in mortality rates, reflecting successful interventions or enhancements in healthcare systems and services.
Conversely, regions like Afar, Somali, Gambella, and to a lesser extent Oromia may exhibit less prominent declines or even fluctuations in neonatal mortality rates, suggesting potential challenges or disparities in healthcare accessibility or quality.
Additionally, factors such as maternal age, birth order, mothers’ wealth index, infant sex, birth size, presence of twins/multiple births, the number of antenatal care visits, and immediate breastfeeding after birth were found to be significantly associated with neonatal deaths.
Footnotes
Acknowledgements
We would like to thank the EDHS team for providing us with the data to analyze and draw conclusions.
Abbreviations
ANC, Antenatal Care; DHS, Demographic Health Survey; EDHS, Ethiopia Demographic Health Survey; EMDHS, Ethiopia Mini Demographic Health Survey; LMICs, Low and Middle-Income Countries; MDG, Millennium Development Goal; NMR, Neonatal Mortality Rate; SDG, Sustainable Development Goals
Author Contributions
All authors contributed to the preparation of the manuscript. S.A. prepared the draft manuscript D.S. collected and conducted analysis then, D.B. and T.G. revised the analysis. M.B., M.G., G.T., N.B., Y.S., F.A., and D.T. revised the final draft of the paper. All authors read and approved the final manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Not applicable. EDHS data used to conduct the study.
Ethical Consideration
Ethics approval was not required for this study. Because the IRB-approval procedures for DHS public-use datasets do not in any way allow respondents, households, or sample communities to be identified. There are no names of individuals or household addresses in the data files. The geographic identifiers only go down to the regional level, where regions are typically very large geographical areas encompassing several states/provinces.
Consent for Publication
Not applicable.