
Abstract
Objective:
The objective of this study was to assess effect of maternal near miss on neonatal mortality.
Methods:
Prospective cohort study was conducted on 384 pregnant women who came for delivery to purposely selected hospitals. The cohort was made up of 128 exposed (near miss) mothers and 256 non-exposed (non-near-miss) mothers. Women who came for delivery were only included. Those who came for services other than delivery such as abortion care, women who developed life-threatening condition not related to delivery, and those who come from no phone network area were excluded. A purposive sampling technique was used by including all mothers with near miss consecutively until the required sample size was obtained. Two non-near-miss mothers were selected using lottery for every near-miss mother. Survival analysis was done for both groups using Cox regression to look for effect of maternal near miss on neonatal mortality. Verbal informed consent from study participants was obtained.
Results:
A total of 354 (118 with near miss and 236 without near miss) women completed the follow-up time, yielding response rate of 92.2%. Of all, 55 (15.5%) of them have previous history of abortion, 44 (12.4%) were admitted to the intensive care unit during delivery, and 22 (6.2%) have history of past delivery of still birth. Severe preeclampsia with intensive care unit admission and severe anemia with transfusion of greater than 2 units of blood were common complications leading to maternal near miss. There were 17 (48 per 1000 live birth) neonatal death at the end of the study, of which 15 occurred among mothers with near miss. Monthly income (adjusted hazard ratio = 998, 95% confidence interval = 0.996–0.999), fetal presentation (adjusted hazard ratio = 6.48, 95% confidence interval = 1.84–22.73), APGAR score (adjusted hazard ratio = 0.746, 95% confidence interval = 0.620–0.898), and being near miss mother (adjusted hazard ratio = 8.40, 95% confidence interval = 1.638–43.118) were significantly affecting neonatal mortality.
Conclusion:
Maternal near miss and other fetal and general maternal characteristics have effect on occurrence of neonatal mortality. Therefore, due attention should be given to these factors for improvement of neonatal survival.
Introduction
The world has made progress in reducing maternal and child mortality in the past several decades.1,2 There has been substantial reduction in the maternal and children mortality since 1990. But the progress is slower in reducing neonatal mortality rates than in reducing mortality rates in children aged 1–59 months. Although the reduction in maternal mortality rate has been substantial, it falls short of the three-quarters target set in the Millennium Development Goals (MDGs) in 1990.1,2 According to report from the World Health Organization (WHO), the current global maternal mortality ratio and neonatal mortality rate is 216 death per 100,000 and 19 death per 1000 live births, respectively. 3
In 2016, neonatal mortality accounted for 46% of under-five mortalities.1,3 The burden is unevenly distributed across regions and countries. At the country level, half of all neonatal deaths are concentrated in five countries of developing regions. 2 Ethiopia is one of the countries with high maternal and neonatal mortality with maternal mortality rate of 412 per 100,000 live birth and neonatal mortality rate of 29 per 1000 live birth in 2016. 4 Different studies had been conducted on maternal near miss in Ethiopia. One of the studies conducted in the northern parts of the country found the overall proportion of maternal near misses to be 23.3% (95% confidence interval (CI) = 20%–26%). 5 But another study conducted in Addis Ababa found 8.01 per 1000 live birth. 6
Still, every year, many women suffer from pregnancy-related complications and many die. Linked to this, there is a burden of perinatal mortality and morbidity. 7 This makes the first 28 days of life most vulnerable time for child survival because children face highest risk of dying in their first month of life. 1 The risk of neonatal deaths was increased in both preeclampsia and eclampsia, albeit slightly higher in eclampsia. 8 The prevalence of all maternal complications was significantly higher in early neonatal deaths. 9 The occurrence of neonatal mortality was also affected by maternal sociodemographic and reproductive history. And its occurrence is also related to low birth weight, preterm birth, and admission to a neonatal intensive care unit (NICU). 10 According to a study conducted in Ethiopia, common causes of maternal near miss were extent of antenatal care (ANC) follow-up, anemia, hypertension, educational level, marital status, income, number of child mother, and early marriage. This study also suggests delivery through cesarean section and female genital mutilation (FGM) has nothing to do with maternal near miss. 11
Harmful consequences of severe maternal morbidity are numerous, including separating mothers and newborns, interfering with bonding, lengthy hospital stays and health care costs, and emotional distress. 12 Therefore, the time of childbirth and the period immediately after birth are particularly critical for maternal, fetal, and neonatal survival and well-being. 13 It is estimated that 40% of neonatal deaths could be prevented by providing high-quality care for both mother and baby around the time of birth. 14 But due to the success of modern medicine, maternal deaths are fewer in number, but there are innumerable “near miss” events which have the potential to teach us lessons. Maternal deaths have been described as the tip of the iceberg and maternal morbidity as the base. For every woman who dies of pregnancy-related causes, 20 or 30 others experience acute or chronic morbidity, often with permanent sequelae that undermine their normal functioning. 15
Incidence of maternal near miss ranges from 0.04% to 14.98%. 16 And relying solely on maternal mortality to assess a country’s status in the area of maternal health overlooks the importance of maternal morbidity, which is not only a precursor to maternal mortality but also a potential cause of lifetime disability and poor quality of life. 15
There are several advantages of investigating near-miss cases over maternal mortality.17–19 It could serve as a proxy for maternal and neonatal death to evaluate quality of obstetric care in particular health institutions.17,20 Identification of severe maternal morbidity (maternal near miss) using appropriate and feasible criteria has endless benefits in improving health of mother and baby. 21 Therefore, maternal near miss is the most important area to look for maternal and child health. Most of the evidence discussed above were from other part of the world and they also study effects of specific complications (like preeclampsia, eclampsia) on neonatal mortality. One of the studies conducted in different hospitals of Addis Ababa Ethiopia follows the respondents only for 1 week. Hence, the objective of this study was to assess effect of maternal near miss on neonatal mortality by following selected mothers for full neonatal period (28 days).
Methods
Study setting, period, and design
This study was conducted in two government hospitals located in Southeast Ethiopia from 1 February to 30 May 2019. Hospitals were selected based on average number of deliveries in the last 6 months before the study. Accordingly, Goba Referral and Ginnir General Hospitals, which were located in Bale and East Bale Zone, respectively, were selected. These hospitals are serving community by providing services like ANC, immunization service, basic obstetrics care, emergency obstetric care and postnatal care, laboratory services, inpatient and outpatient services, and intensive care and neonatal intensive care.
The prospective cohort study in which women who come for delivery were classified as exposed (near miss) and non-exposed (non-near miss) based on criteria of classification and followed to assess effect of near-miss neonatal mortality was conducted among women using obstetrics service in selected hospitals. The entry point to the study was different for exposed and non-exposed mothers. For near-miss mother, the entry point to the study was the time of exposure identification as soon as she arrived to the hospital. For non-exposed (non-near-miss) mother, the entry point was the time of random selection as participants in this study. Exit points were completion of neonatal period (28 days after delivery), development of outcome (occurrence of neonatal mortality), and when a study participant cannot be accessed using phone call.
Eligibility criteria
Women who came to the selected hospital for delivery service and fulfill one of modified near-miss criteria according to Delphi international study 21 and those without near miss and selected randomly as non-exposed group were included in the study. Modified near-miss criteria according to Delphi international study comprise 26 criteria which are subdivided into three categories: clinical, laboratory and management based. The detail of it is in the Supplemental Material. Women who came for services other than delivery such as abortion care, women who developed life-threatening condition not related to delivery, and those who come from no phone network area were excluded.
Sample size calculation and sampling procedure
Sample size was calculated using StatCalc of Epi Info version 7.2.2.2 by taking proportion of early neonatal death among mother with eclampsia 8.61% and in mother without eclampsia 1.38% and odds ratio of 6.58 which was taken from study multicounty study conducted by Abalos and his colleagues assuming 80% power, 95% confidence and ratio of exposed to non-exposed 2 and loss to follow up 10% which give the final sample size 384, of whom 128 were exposed (near miss) and 256 were non-exposed (non-near-miss) participants.
Sample size was also calculated by applying formula for two population proportion for hypothesis testing

where r is the allocation ratio of group 2 to group 1, that is, n2: n1 (n2 = r × n1), p1 is proportion of neonatal mortality among eclamptic mother, p2 is proportion of neonatal mortality among non-eclamptic mother, Zα /2 is the quintile of the standard normal distribution for type I error, Zβ is the quintile of the standard normal distribution for type II error/power, n1 is the sample size for near-miss group, and n2 is the sample size for non-near-miss group.
Two hospitals were selected purposely based on the average number of delivery and neonatal mortality they had in the last 6 months. Sample sizes were allocated to the selected hospitals proportionally. Then, every mother who comes with severe maternal complication (near miss) were included. Then, for every selected near-miss mother, two non-near-miss mothers (randomly if there are more than two) were selected in each health facility separately.
Operational definition
Measurement of variable
Gestational age was measured from last normal menstrual period (if mother remember LNMP) or from ultrasound examination if she has, as well as from mother recall and by measuring fundal height.
Neonatal birth weight was measured using electronic weight scale after removing thick cloth and will be recorded by rounding to the last 1 g of the measurement.
Time of neonatal mortality was measured by close follow-up during hospital stay and using phone call follow-up by asking family members or close relatives after discharge from hospital and recording the exact days of occurrence.
Data collection and quality control
Data were collected using structured questionnaires and checklist. The checklist was adopted from Delphi international study for modification of WHO near-miss criteria for Sub-Saharan Africa and other developing region. 21 Maternal sociodemographic, reproductive history, and neonatal outcome after delivery were measured using tools adopted from Ethiopia Demographic and Health Survey (EDHS) and previous articles. Before the actual data collection, questionnaires were pretested on 5% of total sample size participants who were not included in the study.
Data were collected by two non-provider nurses (those who do not work in selected hospitals) after providing 2 days training. Then, data on sociodemographic characteristics and maternal reproductive history were collected through interview with patient or relative. Other measures such as diagnosis and management provided were retrieved from card using checklist. Phone follow-up was done for all selected women to check neonatal outcome after discharge from the hospital. Then, after data collection, filled questionnaires were kept carefully.
Data processing and analysis
Data entry was done using EpiData version 3.1 and exported to Stata version 14.0 for analysis. Data cleaning was done using frequency distribution and descriptive statistics. Frequency distribution was also done for sociodemographic (general maternal characteristics), maternal reproductive medical and surgical history, and for neonatal outcome for both near-miss and non-near-miss group. Bar chart was done to compare common complications leading to maternal near miss. Life table for neonatal mortality from mothers with maternal near miss and without maternal near miss was done separately. Survival analysis using Cox regression (to look effect of different independent variable on neonatal outcome) was done. Assumption for Cox regression was checked graphically, using goodness of fit and by including time-varying variable in the model. Crude hazard ratio with 95% confidence interval was calculated by including each independent variable and outcome (neonatal outcome whether dead or alive) only. Then, variables with p value of 0.25 or less in bivariate analysis were included in final multivariable analysis. Then, adjusted hazard ratio (AHR) with 95% confidence interval was calculated by including other variables from general maternal characteristics, previous obstetrics and gynecology and medical and surgical history as well as neonatal cause of mortality. Ethical clearance from Institutional Review Board of College of Health Sciences, Addis Ababa University and informed oral consent from study participants were obtained.
Results
General characteristics of study participants
There were 1677 women who gave birth in these two selected hospitals during 3 months of data collection period. Of these, 384 pregnant women were sampled, and 30 questionnaires were excluded because of loss to follow-up. Complete responses were obtained from a total of 354 respondents yielding a response rate of 92.2%. The mean age of the participants was 25.3 years and 186 (52.5%) were rural residents. Based on educational status, 196 (55.4%) were learned up to elementary, 78 (22%) illiterate, and 313 (88.4%) were house wife. Out of 148 (41.8%) of them were referred from other health facility 146 of them were referred from public health sector. Referring health facility provides transportation for 116 (32.8%) of these women. The mean time taken by these pregnant women to reach these selected hospitals was 61 min ranging from 15 to 180 minutes (see Table 1).
Showing general characteristics of study participants of selected women.

SD: standard deviation.
Maternal reproductive history
As shown in Table 2, the average number of pregnancy was 3.07, and on average, 2.7 children were alive. Of all, 55 (15.5%) of them have previous history of abortion, and the mean age at first marriage was 18.44 years. The median gestational age was 38 weeks and the maximum length of hospital stay was 10 days. Of all respondents, 44 (12.4%) were admitted to the ICU during delivery and 22 (6.2%) have history of past delivery of still birth.
Showing maternal reproductive history of pregnant women.

Min: minimum; max: maximum SD: standard deviation; ANC: antenatal care; SVD: spontaneous vaginal delivery; C/S: Caesarean section; ICU: intensive care unit.
Neonatal characteristics
Of 354 women participated in the study, 313 (88.4%) had normal singleton live birth and 31 (8.8%) had still birth. More than half (186 (52.5%)) of neonates were female. There were 290 (81.9%) neonates in the normal birth weight, 53 (15%) were low birth weight, and the rest 11 (3.1%) have large birth weight. Of all live birth neonates, 27 (7.6%) were born with complication, of whom 18 (5.1%) were admitted to neonatal intensive care unit (NICU). Of those 18 neonates admitted to NICU, 11 were cured while 7 died. Of the total live birth, there were 17 (48 per 1000 live birth) neonatal deaths at the end of the study in 8739 person day stayed. Six of these occurred in the first day. See Table 3.
Neonatal characteristics of babies born from selected pregnant women.

NICU: neonatal intensive care unit.
Common complication lading to maternal near miss
As shown in Table 4, severe preeclampsia with ICU admission was common complication leading to maternal near miss (occurred in 42 women), followed by severe anemia with transfusion of greater than 2 units of blood among 33 of women included in the study. Eclampsia ranked third while sepsis/systematic infection ranked fourth. Bar graph in Figure 1 also shows the same finding.
Complication leading to maternal near miss.

ICU: intensive care unit.

Common complication leading to maternal near miss in study participants.
As shown in Figure 1, severe preeclampsia with ICU admission was common complication leading to maternal near miss, followed by severe anemia with transfusion of greater than 2 units of blood. Eclampsia ranked third while sepsis/systematic infection ranked fourth.
Observed survival of neonates among study participants
As shown in Figure 2, neonatal mortality occurs sharply from day 1 to postnatal day 3. Then, it continues to occur from third day up to 10 postnatal days in steady fashion. After 12 days, no neonate died until the end of the follow-up in these women.

Survival curve of observed survival of neonates among women of Bale Zones, Oromia region Southeast Ethiopia.
As shown in Figure 3, neonatal mortality occurs in steady fashion among non-near-miss mothers. But among near-miss mothers, neonatal death occurs rapidly in the first 10 days of postnatal days. Then, no neonates die.
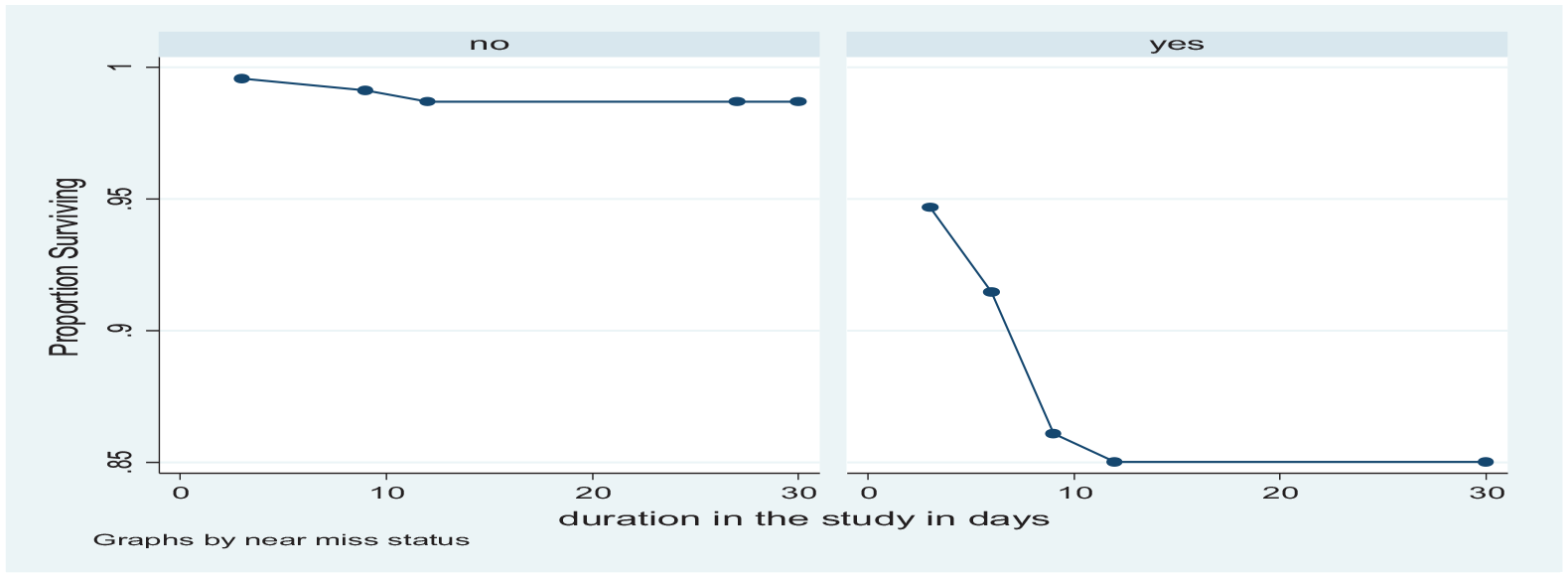
Graph for observed survival of study participants for non-near-miss and near-miss mothers separately.
Comparison of neonatal survival experience in study participants
There is a significant difference on survival experience between neonates born to mother with near miss and mother without near miss (log-rank test χ2 of 25.531, which is significant at p value less than 0.000) (see Table 5).
Log rank comparison of neonatal survival experience in study participants.

Effects of maternal near miss on neonatal mortality
Checking assumptions of Cox regression
Graphical method of testing assumption
The findings from -ln (-ln) show parallel line for near-miss and non-near-miss mothers, which indicates assumption for Cox regression (assumption of proportional hazard) is fulfilled. Also observed versus predicted survival time graph shows the line which is close together for both groups, which suggests assumption for Cox regression is fulfilled (see Figure 4).

-ln (-ln) graph and observed versus predicted survival graph.
Test of proportional hazard assumption using goodness-of-fit test
Goodness-of-fit test for Cox regression assumption (assumption of proportional hazard) suggests assumption for Cox regression was fulfilled because its p value is greater than 0.1 (0.7319) (see Table 6).
Test of proportional hazard assumption using Goodness of fit test.

Breslow method for checking time-varying variables
The result from considering near-miss status as time-dependent variable is not significant which suggests that the assumption of proportional hazard is fulfilled (see Table 7).
Breslow method for checking time-varying variables.

SE: standard error; Tvc: time-varying covariate.
Bivariate and multivariable Cox regression
Multivariable Cox regression was done by including variable found to be important in bivariate analysis. The results from this multivariable analysis demonstrate the variables that are important in predicting neonatal survival. Eight variables were included in multivariable analysis after selection was done based on the finding from bivariate Cox regression. As shown in Table 8, four variables were found as significant factors for the survival of neonates: these were household monthly income (from general characteristics), fetal presentation and near-miss status (from maternal reproductive history), 5-minute APGAR (from neonatal characteristics and near-miss status of the mother). And the remaining four variables such as time taken to arrive to the selected hospital, ANC follow-up status, duration of hospital stays, and birth weight failed to be statistically significant in multiple logistic regression model.
Bivariate and multivariable Cox regression showing factors affecting occurrence of time of neonatal mortality.

CHR: crude hazard ratio; CI: confidence interval; AHR: adjusted hazard ratio; ANC: antenatal care.
Indicates significant factors at p value of <0.05.
There is strong predictive ability of monthly household income on neonatal survival status. In other term, participants with low monthly income experience more neonatal mortality compared with those with relatively high income. As monthly household income increases by one Ethiopian birr, the risk of neonatal mortality decreases by 0.002 ( AHR = 0.998, 95% CI = 0.997–0.999; with p value of 0.032) after controlling for the effect of other variables. The study also found fetal presentation as important predictor variable for neonatal mortality. The rate ratio of neonatal death was 4.5 times for non-cephalic presentation than for cephalic presentation after controlling for the effect of other seven variables in the model (AHR = 4.483, 95% CI = 1.848–22.734; with p value of 0.004). The other variable from neonatal characteristics that has significant effect on the survival of neonatal mortality is 5-min APGAR score. As 5-min APGAR score increases by one score, the risk of neonatal mortality decreases by 0.2 (AHR = 0.746, 95% CI = 0.620–0.898; with p value of 0.002) after controlling for the effect of other variables in the model. Moreover, this study also reveals maternal near-miss status as statistically significant predictor for the occurrence of neonatal mortality.
The risk of neonatal death before 28 days of their birth was 8.406 times for mother with severe morbidity than for mother with no maternal near miss after controlling for the effect of other variables (AHR = 8.406, 95% CI = 1.636–43.116; with p value of 0.001). Duration of hospital stay and time taken to arrive at the selected hospital, birth weight, and status of ANC follow-up show no significant effects on neonatal survival.
Discussion
This study tried to show common complications leading to maternal near miss and effect of maternal near miss on neonatal mortality. The study identified hypertensive disorder of pregnancy (preeclampsia with ICU admission) as common cause of maternal near miss. This finding was in line with the study conducted in Turkish tertiary hospital. 22 Effect of maternal near miss on neonatal mortality was also detailed by collecting hospital-based data prospectively. It shows high neonatal mortality ratio which is higher than national figures reported in EDHS 2016. 4 Proportion of cesarean delivery is lower in this study when compared with findings of two studies from Kenya and Pakistan.23,24 This might be because women in this area prefer to have spontaneous vaginal delivery. Current stillbirth was also higher than what were found in other studies conducted in Ethiopia and Pakistan.24,25 The reason for the difference in this study might be high proportions of mothers with severe maternal morbidities were included. It can be also due to difference in sociodemographic status of study participants. The finding from current study reveals severe pregnancy-induced hypertension, severe anemia with transfusion of greater than two units of blood, and sepsis as common causes of severe maternal morbidity (maternal near miss). This finding was supported by the results of others studies.9,11,23,26
The study found monthly household income as significant factor which affects neonatal survival. This finding was in line with other multi-country study conducted in 194 countries. 27 This might be because household income level may determine early seeking of care during labor and influence access to health facility as soon as possible. For those with low-income level, preparing financial requirement is one of the barriers in seeking early care. The other variable which shows significant effect on neonatal mortality in bivariate and which loses significance in multivariable analysis is the time required to reach selected health facility. This finding is consistent with the study conducted in Indonesia on maternal characteristics and obstetrical complications’ impact on neonatal outcomes. 28 ANC follow-up status which shows statistically significant finding in bivariate analysis at 95% confidence level loses its effect after inclusion of other variables in the model. This result is in agreement with the finding from studies conducted in Uganda and Pakistan.24,29 But it is in conflict with other study which found ANC as significant factor on neonatal mortality. 28
This might be because only few (5.9%) women in this study did not have ANC follow-up and hide effect of ANC follow-up on neonatal survival. Fetal presentation was also found as one of the factors that affects neonatal mortality in this study. This finding was similar to the finding from multi-country study conducted in 29 countries and another study conducted in Kenya.9,30 This might be because malpresentation prolongs duration of labor and increases likelihood of intrapartum complication on neonate. This study found duration of hospital stay as statistically non-significant factor for survival of neonate. This finding supported other study which found duration of hospital stay as statistically non-significant factor for neonatal mortality. 28 This might be due to more neonatal mortality occurs in the first day of delivery and mothers were excluded from contributing in the study. The major finding of the study is that the presence of maternal near miss is a risk factor for neonatal mortality independent of time taken to reach selected hospitals, monthly income, fetal presentation, birth weight, and 5-min APGAR score. This study was consistent with other studies conducted by various authors in different parts of the world.8,9,23,24,28-30 This might because severe maternal morbidity affects well-being of baby. Neonatal birth weight was found as not statistically significant factors for neonatal mortality. This was not in line with the various studies finding.9,25,26,31 This might be because of difference in sociodemographic characteristics as well as inclusion of other important variables in this study. Five-minute APGAR score is the last variable found as a significant factor in determining neonatal survival. This agrees with the finding of other studies.9,31 This is because neonates with low APGAR score might have underlining complications which affect their survival.
Study use self-reported information for occurrence of outcome of interest which could be subjected to reporting errors and biases, especially in measuring accurate time of outcome development. The study is solely quantitative and not supplemented by qualitative data. The study was conducted only in public hospitals; hence, neonatal mortality in these two groups does not represent those who deliver at private health facility and home delivery. Hence, generalizability of this finding should be taken by considering this issue. Neonatal mortality may also relate to quality-of-care issues that this study does not investigate. And we recommend future researchers to conduct studies addressing these issues.
Conclusion
Neonatal survival was not only the result of maternal complication. General sociodemographic and neonatal characteristics also have their share. Hence, most of the factors were modifiable if efforts were done to improve socioeconomic status of community. The study found that women with maternal near miss have adverse neonatal outcome, which requires evidence-based management to improve neonatal survival from all concerned.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211042219 – Supplemental material for Effect of maternal near miss on neonatal mortality in selected hospitals: Prospective cohort study, Southeast Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121211042219 for Effect of maternal near miss on neonatal mortality in selected hospitals: Prospective cohort study, Southeast Ethiopia by Ahmednur Adem Aliyi, Negussie Deyessa and Mengistu Yilma Dilnessie in SAGE Open Medicine
Footnotes
Availability of data
The authors confirm that all data underlying the findings are fully available without restriction. All the necessary data were included in the paper. However, the raw data set in SPSS or STATA can be obtained by email request at
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethical approval was obtained from Institutional Review Board of Addis Ababa University with ethical approval number 004/11, and oral consent from each study participant was obtained. This board approved verbal informed consent. The checklist was cited as it was obtained from other source.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Addis Ababa University from the School of Public Health. The funders had no role in study design, data collection and analysis, or preparation of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.