
Abstract
Medical advances have enabled infants born premature or with congenital cardiac defects (CHD) to have increased lifespans. Understanding neurodevelopmental profiles and outcomes enhances the identification of potential challenges and helps pinpoint targets for early intervention, starting from infancy. Neurodevelopmental vulnerabilities are documented for both populations, with developmental delays, including cognitive, motor, language, neurosensory, and social-emotional development. Whereas neurodevelopmental follow up for premature infants is established, similar protocols are not typically in place for CHD infants. The current study aims to identify trends in these at-risk populations to better understand developmental trajectories and provide recommendations for follow up. Outcome measures of cognitive, motor, language functioning from the Bayley Scales of Infant and Toddler Development, Third Edition, along with growth measurements and cardiac diagnoses from 322 participants, aged 6 months (cardiac) and 6 months age-corrected (premature infant) were collected. Similarities in functioning were identified. Findings indicate associations between CHD diagnosis and motor development, prematurity and severity of outcomes, and head circumference and cognitive functioning. Cardiac diagnosis severity alone was not associated with outcome severity. These findings expand previous literature identified similar at-risk profiles and needs. Continued follow up through school age is recommended to identify subtle delays that may emerge throughout development.
Introduction
Contemporary advances in medicine have enabled significant changes in the mortality and neurodevelopmental trajectories of children born premature and with congenital cardiac defects.1,2 The World Health Organization (2016) has defined the gestational age determinant of prematurity as birth prior to 37 weeks gestation, with infants born before 28 weeks gestation classified as “extremely preterm,” those born between 28 and 31 weeks as “very preterm,” and between 32 and 37 weeks as “moderate to late preterm.” Currently, prematurity affects 5%-18% of pregnancies, and premature birth is implicated in about half of infant deaths, owing to birth-related or other complications, such as infection. 3 Although survival rates have increased by approximately 50%-70%, nearly half of infants born premature experience some disability. 4 Children born with congenital cardiac defects are similarly at risk for neurodevelopmental delays, which can impact lifetime functioning. 5 Congenital heart diseases (CHD) are the most common birth defect in the United States, affecting 8 to 9 out of every 1,000 children. 6 Whereas in previous decades, infant mortality secondary to congenital cardiac defects was far more common, prenatal diagnosis and intervention along with advances in neonatal care have increased survivorship rates in this population by 90%, even in complex cases. 7 As survival rates improve, patterns of neurological and neurodevelopmental impairments have become apparent in childhood. Surgical interventions are often required soon after birth. While often lifesaving, surgery can lead to brain injury and be associated with long term neurodevelopmental and neurobehavioral impairments. 8
Research has identified various neurodevelopmental outcome similarities among these two high-risk populations, including in areas of cognitive, language, motor, and behavioral functioning.1,9 Children born premature or full term with congenital cardiac defects typically present with immature brain development at birth and are vulnerable to early brain injury and subsequent delayed neurodevelopmental outcomes. 8 Neurodevelopmental delays have been identified in the preterm 10 and cardiac 5 populations, and studies have proposed the importance of neurodevelopmental follow-up through infancy and into childhood and adolescence. 11
Neurodevelopmental outcomes are affected by a combination of prenatal, perinatal, and postnatal factors. Premature and CHD infants are susceptible to brain injury resulting from multiple causes including development in the extrauterine environment 12 as well as secondary to medical interventions and complications. 13 Licht et al. 14 have identified that the neurodevelopmental profiles of children born with CHD are quite similar to children born premature, which is likely related to brain injury subsequent to periventricular leukomalacia (PVL) or white matter injury (WMI) in the developing brain. Other sources of damage, including hypoxia, low blood flow, and reduced delivery of nutrients, have also been implicated in reduced brain development and white matter formation in these vulnerable populations. 15
Neurodevelopmental outcomes
Given the nature of atypical brain development characteristics of premature infants, implications for cognitive, behavioral, motor, and behavior functioning are expected and have been well-researched. 10 Poorer cognitive outcomes are related to insufficient brain development in-utero, 10 and early assessment of cognitive and motor development has demonstrated cognitive, language, and motor delays in children born preterm as compared with term-born peers at preschool age 2 Behavioral concerns have been identified in toddlers 18-22 months corrected age, 16 and in a two-year-old sample 17 that demonstrated more internalizing behaviors, dysregulation problems, sensory sensitivity, as well as reduced attention, pretend play, and empathy, where cognitive and language functioning (per Bayley Scales of Infant and Toddler Development, Third Edition, Bayley-III) 18 mediated behavior and competence.
Meta-analysis has established relationships at school age of prematurity with lower IQ, internalizing and externalizing behaviors, and a significantly higher incidence of attention-related problems and diagnoses of Attention-Deficit/Hyperactivity Disorder (ADHD) compared to term-born peers. 19 Challenges with higher order processing, attention, executive functioning, and sensory processing have also been identified20,21 and are consistent with damage to the neural connections between the prefrontal cortex and other cortical brain regions, as well as with differential white and grey matter volume changes. 22 Executive functioning deficits and behavioral problems can persist through childhood, despite “normal or low normal” cognitive functioning. 23 Achievement deficits are similarly present in reading, with most prominent deficits in mathematics. 20
Similarly, Licht et al. 14 identify the need for academic intervention at school age, given implications of neurodevelopmental outcomes in children who were born with CHD. Children born with CHD typically tend to score in the low-normal range on IQ tests. 1 Lower cognitive and motor functioning have been associated with CHD, with a significant established association between multiple surgeries and impairment severity. 5 A meta-analysis about children born with CHD found decreased motor outcomes following surgery 24 and identified vulnerabilities, including increased length of hospital stay, lower birth weight, longer time on bypass, and poorer growth outcomes. 25 Early deficits in motor functioning and muscle tone abnormalities have been documented, 26 with relationships between impaired fine and gross motor functioning and school performance. 27 Similarities between the CHD and premature populations indicate similar at-risk profiles and related needs for monitoring. Results of the EPICARD study support this, as Calderon et al. 28 observed subtle deficits on executive and global functioning measures in the CHD population. Diagnosis severity has been associated with impaired cognitive functioning at school age, 29 which may be related to the more complex surgical involvement for this population.
The current investigation
Whereas there is a rich body of literature concerning outcomes and treatment trajectories for premature infants that has contributed to a structured intervention approach in early infancy and childhood, less is known about outcomes in the CHD population. 30 A similar intervention structure is not yet in place, despite identified deficits in areas of executive functioning, general cognitive functioning, and motor development, that can broadly impact academic and social functioning. This study aimed to identify similarities and differences in neurodevelopmental trajectories and consider treatment recommendations for future neurodevelopmental follow-up for the CHD and premature infant populations. Gaining a more nuanced understanding of similarities and differences between the neurodevelopmental trajectories of these populations can help to identify how early experience affects developmental outcomes. Further, earlier identification of functioning deficits can inform earlier intervention and thereby contribute to better developmental outcomes. 11
A recent study by Chorna et al. 30 that discussed outcomes of a neurodevelopmental follow-up clinic for evaluation of late-term premature infants and CHD infants at 6, 12, 18, and 24 month time intervals through utilization of existing and established resources that were in place (Early Intervention services largely targeted toward extremely/very preterm infants), assessed for risk and provided services for these populations in which developmental follow-up was previously not emphasized. In this vein, the current study sought to understand similarities in trends within these populations that can support the development and implementation of neurodevelopmental follow-up initiatives, which can indicate whether application of interventions used with the premature infant population can be effective also with the CHD infant population.
Given established literature that has discussed the relationships between CHD diagnosis and increased motor deficits especially in infancy 24 and understanding the nature of motor restriction following cardiac surgery, it was predicted that motor delays would present most prominently in the CHD sample. Further, given established relationships between decreased cognitive functioning and earlier preterm birth, 10 it was predicted that the most severe cognitive outcomes would present in the earliest-born preterm group. As research has established relationships between growth and neurodevelopmental outcomes with associations between lower cognitive scores and motor scores, 31 smaller head circumference and lower cognitive scores 32 and lower language functioning, 33 and lower birth weight, this study sought to identify associations between growth parameters and neurodevelopmental outcomes in the CHD and premature infant populations. Finally, as associations have been identified between severity of cardiac diagnosis and related interventions, 28 this research aimed to explore the effect of specific cardiac diagnoses on overall outcomes.
Methods
Participants
Data were available for 322 infants who were treated in the Neonatal Intensive Care Units (NICU) at New York University (NYU) Tisch and Bellevue hospitals for medically indicated reasons and were subsequently followed up at the Neonatal Comprehensive Care Program (NCCP). Two participants were excluded from analyses due to missing data, leaving 320 infants included in the adjusted and overall sample, including 76 infants diagnosed with CHD and 244 premature infants included in the initial data set. For a summary of demographic data, see Table 1.
Demographic Characteristics of Participants.

Preterm infants were grouped into three categories, and CHD infants were grouped into five categories. While some premature infants were secondarily diagnosed with cardiac conditions at birth, and some CHD infants were born premature, the primary referral diagnosis was used for category groupings.
Premature infant groups- Infants were classified into three groups by gestational age at birth (extremely preterm: below 28 weeks gestation; very preterm: between 28 and 31 weeks gestation; and moderate-to-later term: between 32 and 36 weeks gestation). Infants in the moderate-late term category were dually diagnosed with a medical condition (e.g. anoxia, intrauterine growth restriction) and thus referred for follow-up care in the NCCP.
CHD infant groups- Five established STAT Mortality Scores were used to group CHD infants into categories. 34 Category 1 included diagnoses of patent foramen ovale, atrial septal defect, and ventral septal defect. Category 2 included diagnoses of patent ductus arteriosus, tetralogy of Fallot, pulmonic valve stenosis, and coarctation of the aorta. Category 3 included TGA and pulmonary atresia. Category 4 included diagnoses of double outlet right ventricle, Ebstein’s malformation, and Blalock-Taussig shunt, while category 5 included hypoplastic left heart syndrome and hypoplastic right heart syndrome.
Measures
The Bayley Scales of Infant and Toddler Development- Third Edition (Bayley-III) The Bayley-III is a revised version of the BSID-II 35 that was designed to measure the developmental functioning of young children, ranging from 1 to 42 months of age. 18 The Bayley-III provides composite scores for cognitive, language, and motor functioning, as well as social-emotional and adaptive behavior scales. The standardization sample for the Bayley-III included a 10% proportion of participants who had developmental problems, with the goal of improving the ability to identify developmental delay in high-risk children. 35
Procedures
The study is cross-sectional study of medically fragile infants who are 6 months of age and graduates of the NICU. A retrospective chart review was completed to include data for infants followed up at the NCCP because of premature or cardiac diagnoses. Children from the premature infant and CHD populations born between January 2015 and February 2018 were included in this study. Participants underwent neurodevelopmental assessment at 6 months gestational or corrected gestational age (i.e. 6 months from proposed due date, or 6 months plus number of weeks prior to due date at birth), 36 as appropriate. Developmental follow-up information was collected to assess development in cognitive, language, and motor domains using the Bayley-III. 18 The Bayley-III was administered by either a trained clinical psychologist or occupational therapist, both of whom are members of the follow-up program’s interdisciplinary team. Although the participant may have returned for multiple follow-up visits, The composite score data from each domain were analyzed for each participant, from the follow-up visit at 6 months. Institutional Review Board (IRB) approval was obtained from New York University Langone Medical Center (IRB# i18-00040) and Pace University (IRB# 1195228-1) before data analysis.
Demographic and medical information was gathered from participants’ medical charts via chart review. Demographic information included: gender, birth date, gestational age, birth weight, and head circumference at follow-up. Medical information included cardiac diagnoses. The data used in the current study were taken from several previously compiled data sets and were de-identified prior to analysis.
Ethical approval and informed consent
This study was conducted using archival data only, with no direct involvement of human participants. As such, the study qualifies for exempt status concerning informed consent. All data analyzed was archival and met criteria for waiver of patient consent. Thus, in accordance with applicable ethical standards and institutional IRB policies, the data examined was collected and anonymized prior to analysis, ensuring the confidentiality and privacy of all individuals represented in the dataset. Institutional Review Board (IRB) approval was obtained from New York University Langone Medical Center, (IRB# i18-00040) and Pace University (IRB# 1195228-1) before data analysis.
Data Analyses
Descriptive statistics were calculated to characterize the sample and test hypotheses. Means and standard deviations were calculated for Bayley-III composite scores, birth weight measurements, and head circumference measurements for the premature and CHD groups. Independent samples t-tests were used to compare motor outcomes between CHD and preterm groups. A one-way ANOVA was conducted to examine composite score outcomes (i.e. cognitive, motor, and language scores) between preterm and CHD subgroups. Pearson product-moment correlations were used to assess relationships of growth parameters (head circumference and birth weight) with composite scores. Finally, a one-way ANOVA was conducted to examine differences in composite score outcomes between CHD subgroups.
Results
Motor outcomes
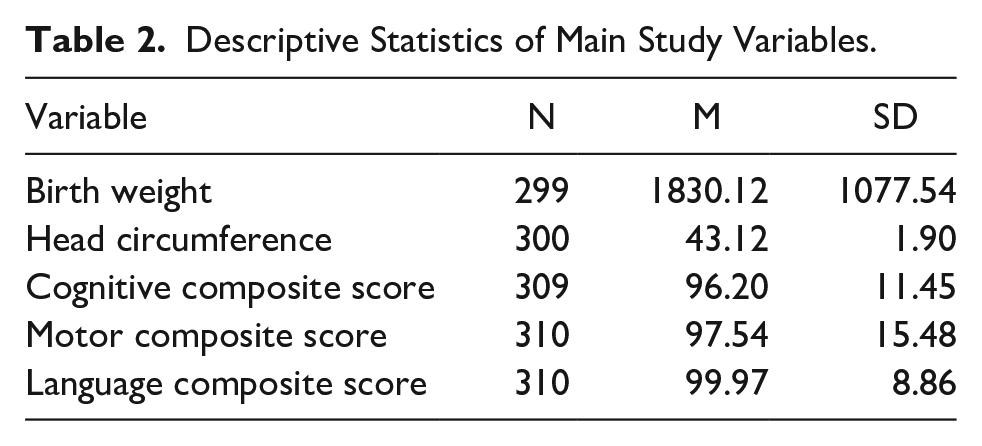
Given the unique impact on motor outcomes in the CHD population, differences in motor outcomes between the premature sample as a whole and CHD sample were explored. Using Bayley-III motor scale composite scores as the outcome variable, an independent samples t-test indicated a significant difference in outcomes between the premature and CHD samples, with poorer motor outcomes in the CHD population; t (308) = 2.76, p = .006, d = .35 (see Tables 2 and 3 for group means and standard deviations).
Descriptive Statistics of Main Study Variables.
Bayley-III Composite Scores and Growth Parameters by Group.

Severity of overall outcomes
A one-way ANOVA was conducted to determine whether the most severe neurodevelopmental outcomes presented in the extremely preterm group, with significant differences found between groups in cognitive outcomes, F (3,305) = 2.70, p = .046 and motor outcomes, F (3,306) = 4.94, p = .002; while there were no significant differences for language outcomes, F (3,306) = 1.30, p = .273 (refer to Table 3 for group means and standard deviations). Bonferroni post-hoc comparisons found that cognitive scores in the extremely preterm group were lower than the very preterm group (p = .029, d = .45). There were also significant differences between groups in motor outcomes, with the CHD group scores being lower than the very preterm (p = .050, d = .43) and moderate-late preterm/dual diagnosis (p = .006, d = .53) infant groups. There were no significant differences in cognitive outcomes between moderate-late preterm/dual diagnosis and CHD groups, and no significant differences in motor outcomes between the extremely preterm and very preterm, or extremely preterm and CHD groups. No differences were found between groups for language outcomes (see Table 4 for related data).
Cognitive, Motor, and Language Score Bonferroni Post-Hoc Comparisons.

Growth Outcomes
Bivariate relationships between growth outcomes and Bayley-III composite scores were evaluated with Pearson product-moment correlations (see Table 5). There was a significant negative correlation between smaller head circumference and lower cognitive composite scores. Associations of head circumference with motor and language outcomes were nonsignificant. There was a marginally significant trend between lower birth weight and lower language composite score, while relationships of birth weight with cognitive and motor scores were not significant. It is notable that the mean cardiac birth weight (M = 2664.75, SD = 957.24) was nearly 2000 grams higher than the mean birth weight for the extremely preterm group (M = 975.40, SD = 772.95), suggesting a possible negative association between language outcomes and preterm birth.
Bivariate Correlations among Growth Parameters and Composite Scores.

STAT Categories
One-way ANOVAs were conducted to investigate whether Bayley-III outcome scores differed based on STAT category. There were no significant differences for cognitive outcomes, F (4,83) = 0.92, p = .456; motor outcomes, F (4,83) = 0.27, p = .899, or language outcomes F (4,83) = 0.22, p = .927.
Discussion
While long-term survival for premature infants and infants born with congenital cardiac conditions has improved, these populations are at risk for adverse neurodevelopmental outcomes.1,2 Stålnacke et al. 37 describe significant heterogeneity of outcomes among preterm-born infants in a study of cognitive and executive functioning outcomes from early childhood through adolescence. The current research joins early analyses of neurodevelopmental outcome similarities and supports the proposed importance of neurodevelopmental follow-up for identification and provision of early intervention services.30,11
It is notable that the Bayley-III outcome scores in the current study largely fall in the low-to-middle average range of functioning (90-109). Although clinically significant deficits are not identified for most preterm or CHD patients included in this sample, early sub-clinical deficits may be a marker of more pronounced decreases in functioning during late-childhood and early adolescence. Mild to moderate delays in functioning may emerge as children progress through school and subtle deficiencies may emerge as children struggle to attain more advanced skills that depend on basic abilities. 38 Heightened awareness and readiness to provide services can provide important advantages to children in these populations.
Motor outcomes for the CHD infant sample were comparatively worse than the premature sample, which is consistent with earlier research, 5 including findings of decreased motor outcomes following cardiac surgery, as measured by the BSID-II. 24 Contributing factors include length of hospital stay, lower birth weight, time on bypass, and poorer growth outcomes, 25 which are consistent with the clinical experience of CHD participants in the current study who have undergone surgery. Mobility is limited during post-surgical hospital stays, impacting the ability to develop and maintain motor skills critical for development and functioning. 39 Notably, motor outcome similarities were not significantly different between the extremely preterm and CHD populations, supporting assertions that these populations have similar motor outcome profiles.1,9
Motor skills, and fine motor skills in particular, are critical for developing early learning skills necessary for later school success. 40 These early indicators of decreased neurodevelopmental functioning are consistent with later established deficits in cognitive and academic functioning.8,13 Documented improvement in motor deficits in a sample of CHD patients evaluated at 6-8 months 41 supports the assertion that neurodevelopmental follow-up care is critical for supporting success in this vulnerable population.
Our results identified lower cognitive outcomes in the extremely preterm infant sample as compared with their very preterm counterparts, which supports the conclusion that most severe deficits are present in infants born at earlier term. 21 MRI scanning supports a relationship between severity of WMI and severity of cognitive delay from early childhood through early adolescence. 42 Our findings that the preterm group primarily scored at the low end of the normal range are consistent with previous findings. 10 As positive outcomes have been demonstrated for continued cognitive and motor improvement following early intervention in premature infant samples, 17 these results underscore the importance of early sensitivity and intervention for even slight deficits.
Although significant cognitive deficits were not identified in the current CHD sample at 6 months, emergence of deficits in the CHD population in later childhood and early adolescence has been found previously. 29 Whereas deficits in premature infants can be attributed to early brain development factors, children with cardiac problems face ongoing health challenges, with risk factors that can evolve over time depending on their condition. 7 Research highlights that this is particularly true for populations with single-ventricle CHD. 7 Academic and social difficulties can relate to these later-emerging medical problems as children with cardiac problems reach school age, and assessment and intervention should be incorporated into care.
Our findings indicated correlations between smaller head circumference and lower cognitive scores, as well as between lower birth weight and lower language scores, consistent with established relationships between lower cognitive scores and head circumference. 31 As discussed, lower cognitive outcomes are likely associated with interrupted brain development and related WMI in the premature infant and CHD populations, 42 which are likely contributors to decreased head circumference.
The marginally significant trend toward an association between lower birth weight and lower language outcomes supports established research that associates language deficits with preterm and very low birth weight (VLBW) status. 33 The Early Preterm Infants in Sweden Study (EXPRESS) 43 identified decreased cognitive, language, and motor deficits in the preterm population, and proposed that greater awareness of deficits can direct intervention and communication with caregivers. Zimmerman 44 identified through a meta-analysis of studies with preterm and VLBW children that the language scores were typically below average but often still within normal limits, and that deficits typically persisted to school age. Other research has suggested a relationship between delayed brain development and use of ventilators with language and related feeding difficulties. 45 Although scores did not necessarily indicate a need for services based on the cut-off scores for receiving services in most school districts (1-2 SDs below the mean), functional deficits were observed to impact language abilities.
Finally, there were no significant relationships between STAT Mortality Scores and Bayley-III outcomes, and our results support the assertion that the CHD population can be treated similarly across STAT categories with regard to risk monitoring. It is notable that sample sizes for severe cardiac diagnosis categories were small, which mimics lack of stratification based on severity in available research samples (e.g. Calderon et al. 28 ). It is possible that a larger sample size with a greater proportion of CHD severity would reveal different patterns.
Implications
This study contributes to a growing body of research that is focused on better understanding neurodevelopmental outcomes in medically fragile infants (e.g. Ref. [30,1,46]). The current findings underscore the potential for adapting and applying resources established for intervention with the preterm population to best serve the needs of the CHD population. Multi-disciplinary neurodevelopmental follow-up is important to assess the array of potential deficits in high-risk infants, and early identification can be critical for providing appropriate intervention. 47 Intensive follow-up for premature and CHD populations can assess neurodevelopment in populations that have otherwise been assumed to be of lower risk, and implementing established resources (e.g. early intervention services) can provide greater opportunity to provide services where developmental follow-up was previously not emphasized. 30 Long-term attention from neurodevelopmental specialists is particularly important, as many medical providers are not aware of potential neurodevelopmental deficits or the appropriate referral options. 48
In this study, infants with dual diagnoses of prematurity and CHD were analyzed together with those having only one of these conditions. While this approach reflects the real-world clinical scenario, where such co-occurrences are common, we acknowledge that the combined effects of prematurity and CHD may have influenced the outcomes differently than in those with either condition alone. Future research should further investigate these subgroups to clarify their specific contributions to clinical outcomes.
These findings are notable in light of the “vulnerable child phenomenon,” 49 which identifies that parents of children who experience extreme medical risk in early childhood may be less perceptive of mild deficits in functioning given the challenges associated with simply achieving survival and have been identified in parents of a CHD infant sample. 50 As children without physical impairment who experience mild delays are less likely to receive intervention services, 51 educating medical and educational professionals to identify deficits in these populations and recommend interventions and resources is warranted. 46
Although no participants in this study had a diagnosis of cerebral palsy (CP), it is noteworthy to mention this vulnerable population of infants is at an increased risk for CP, when compared to the full-term population. 52 While there has been advancement in the technology utilized for neonatal care, cerebral palsy continues to be a prevalent neurological complication among extremely low birth weight survivors, affecting 9%-17% of them. 52 Awareness of the risks of cerebral palsy in preterm infants enables medical teams to make well-informed choices about neonatal care, treatments, and follow-up services, helping to reduce the chances of complications. Additionally, this knowledge would be beneficial for families as it will enable them to access resources such as emotional support groups and prepare for the challenges of raising a child with specialized needs.
Helping mitigate deficits early on can encourage engagement in the school environment and increase participation in academic activities while preventing later and potentially compounded delays. 53 In addition, creating awareness of the potential need for services despite not meeting traditional criteria is a critical recommendation of our study.
Limitations
Our study evaluated neurodevelopmental outcomes using Bayley-III composite scores to assess development in cognitive, language, and motor functioning. While this assessment has been updated and is widely used, limitations have been addressed with regard to overestimation of functioning. 54 Thus, continued neurodevelopmental follow-up over time is recommended to monitor outcomes, 11 with a particular focus on identifying areas of mild delay. Additionally, data available for CHD infants were sizeable overall, but included relatively small proportions of infants with higher levels of cardiac severity, and results may overestimate functioning in infants diagnosed with more severe cardiac diagnoses. Further, whereas infants in this sample were classified based on the referral diagnosis to the NCCP (preterm or CHD), a small proportion of this sample included infants who were dually diagnosed. Future research that includes larger sample sizes of dually-diagnosed CHD-preterm infants may provide more nuanced information about functioning and can better direct intervention needs for these children. Finally, whereas previous research has identified racial and socioeconomic factors that contribute to risks and outcomes in the preterm and CHD populations, this study did not focus on the relationships between these factors and neurodevelopmental outcomes.
Conclusions and Future Research
As medical advances continue to improve the likelihood of survivorship in premature and CHD infant populations, it is critical to understand neurodevelopmental trends and outcomes. Our findings identified an overall trend toward functioning in the low-normal range in areas of cognitive, language, and motor functioning. Cognitive functioning is a particular area of vulnerability for extremely preterm infants, while motor functioning is a specific area of vulnerability for CHD infants. Early brain damage subsequent to preterm birth, low oxygenation, or surgical intervention appears to be a significant factor in shaping early outcomes, and directing early and ongoing intervention efforts can have invaluable effects on outcomes through school and into adulthood. Educating and empowering parents to be aware of the possibility of deficits and encouraging them to seek out services at the first sign of concern is critical to providing intervention for children in this population, who may not be otherwise identified as in need of services.
Future research with larger CHD samples will expand the growing literature and provide further direction for early trajectories and intervention needs. Additionally, longitudinal follow-up may provide a better understanding of the individual and related trajectories for these populations. Finally, research with a more diverse sample that focuses on the roles of socioeconomic status- and race-related factors may provide greater insights about the most effective approach to intervention for specific populations. It is expected that continued focus on areas of vulnerability to best direct education and intervention in family, medical, and educational settings can improve outcomes and quality of life for individuals and their families.
Footnotes
Author Contributions
MK: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MZ: Contributed to conception and design; Contributed to analysis; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LR: Contributed to conception and design; Contributed to analysis; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
FS: Contributed to conception and design; Contributed to analysis; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
HH: Contributed to conception and design; Contributed to analysis; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JS: Contributed to analysis; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.