
Abstract
Objective. Sub-optimal management of childhood asthma in developing countries has been a recognized issue for decades. Our study aimed to evaluate actual practice in the management of asthma among pediatricians in Indonesia and identify gaps to the national guideline. Methods. We conducted an online survey involving 1386 pediatricians from 37 of 38 provinces in Indonesia, representing 28.8% of the pediatricians registered in the Indonesian Pediatric Society. Results. While nebulizers and inhaled reliever medications were widely available, inhaled corticosteroids medications and spirometer were scarce. Only 16.2% of pediatricians used spirometer to support the diagnosis. Meanwhile, routine blood counts and chest X-ray were commonly performed, and nearly 90% of pediatricians reported prescribing oral short acting β2-agonist as relievers, which is inconsistent with guidelines. Conclusion. There are significant gaps between national guidelines and actual practices in childhood asthma management in Indonesia, which may be due to disparities and barriers to medication access.
Introduction
Asthma is a chronic respiratory problem, which mostly prevalent in children. A recent Global Asthma Network (GAN) study reported global prevalence of asthma at 11% in children aged 6 to 7 years and 9.1% in adolescent aged 13 to 14 years. 1 While infectious diseases and malnutrition in children remain primary concerns in most low-and middle-income countries (LMICs), the prevalence of non-infectious diseases, including asthma has been increasing and becoming a major public health problems in these countries.2 -4 The prevalence of reported asthma symptom in children and adolescent in LMICs increased from 12.1% in 1990 to 13.9% in 2010. 5 Asthma contributes not only to high rates of morbidity and emergency hospital visits, but also to missed school days and lower academic performance. 6
The data from a single center in Indonesia in 2016 documented differences in asthma prevalence between children and adolescents in Indonesia. While the rates of reporting wheezing ever and wheezing in the past 12 months are similar across both age groups, a significant contrast emerges in the prevalence of asthma ever and physician-diagnosed asthma. Adolescents demonstrate a higher prevalence for both conditions, with 8.4% reporting asthma ever and 6.6% having received a physician’s diagnosis, compared to 5.4% and 4.4%, respectively, in children. 7 These findings suggest that while the prevalence of asthma in children might appear relatively low, this could reflect the actual rates but may also indicate potential underdiagnosis or mis-diagnosis.8,9 A systematic review showed that 37% to 56% of children with asthma were underdiagnosed, suggesting that the true prevalence in Indonesia might be higher than reported. 10
The increasing prevalence of asthma in developing countries is often associated to suboptimal management, both in the diagnosis and treatment. Challenges include a shortage of resources for accurate diagnosis, insufficient competency among doctors, and limited access to treatment due to the high costs of inhaled therapies and the geographic remoteness of healthcare facilities. Additionally, inadequate awareness and knowledge among the affected population, coupled with poor environmental control of asthma triggers, further complicate effective and optimal asthma management.11 -13 A recent study conducted in Indonesia found that less than 30% of school-age children with asthma reported using inhaled short-acting β2 agonist (SABA), and fewer than 5% had been prescribed inhaled steroid. 7
Physicians’ practices play a crucial role in the management of childhood asthma. However, data in these practices in developing countries, including in Indonesia, is limited. The Indonesian Pediatric Society (IPS) has published a national guideline on childhood asthma, but the implementation has not been thoroughly evaluated. The gap between evidence-based recommendations and actual practice contributes to the inadequate control of asthma, and previously, there was no available data on this gap in Indonesia. Understanding the gaps between policy and practice is crucial to identify barriers, improving healthcare delivery and enhancing outcomes for children with asthma. Therefore, we aimed to address this gap by investigating disparities in resources, common clinical practices, challenges, and barriers in diagnosing and treating asthma in children in Indonesia, and to compare these practices with the recommendations the national guidelines. This objective data is essential for improving asthma management in children, not only in Indonesia but also across other developing nations and LMICs globally.
Material and Methods
Study Design and Setting
We conducted a cross-sectional study using an online national survey of pediatricians across Indonesia from December 2021 to February 2022. Indonesia is a large archipelago with approximately 18 000 islands (6000 of which are inhabited), consists of 38 provinces, with a total population of 273.8 million in 2021. The distribution of human and health resources, along with geographical characteristics, varies significantly across provinces. Provinces in Java and Bali Island generally have better resources compared to those located outside Java, where healthcare facilities are often more constrained or limited.
Population and Sample
Pediatricians who were members of the IPS and worked in any of health facilities-including public or private hospitals (secondary of tertiary), private practices, and clinics, were invited to participate in the study. The inclusion criteria for this survey were pediatricians practicing in rural or urban area in Indonesia who have clinical experience managing children with asthma in hospitals, clinics, or other healthcare facilities and voluntarily participate in the survey, with submission of responses indicating consent to participate. Pediatricians who were inactive in clinical practice (eg, retired, newly graduated pediatricians without a practice license) were excluded.
To determine the minimum required sample size for the survey, a sample size calculation was conducted based on total population of approximately 4813 pediatric specialists across Indonesia. using 95% confidence level (Z = 1.96), a margin of error of 5% (e = 0.05), and an assumed response proportion (p) of 0.5 to maximize variability, the following formula was applied.

The calculated minimum sample size of 358 respondents was considered sufficient to ensure representativeness of population within the specified level and margin of error.
Participation was voluntary and anonymous. Each pediatrician was allowed to submit only 1 response. All participants who completed the survey within the specified period were included in analysis.
Procedure
The questionnaire was designed and developed to evaluate critical dimensions of pediatric asthma management, including pattern of patient visits, availability of facilities and resources, utilization of diagnostic tests, and therapeutic intervention. The rationale and objective of the study were clearly outlined in the online survey. The questionnaire comprised a combination of multiple-choice question, Likert scale items, and open-ended responses ensuring a comprehensive approach to data collection. It was consisted of 22 question designed to gather information on participant’s background and demographic, including age, sub-specialty, district, and province. It also aimed to collect data on the average number of asthma patients seen daily in their outpatient clinics and monthly in inpatient settings, the availability of spirometers and asthma medications at their clinics, common practices for diagnosing and managing asthma, both during asthma attack and in long-term management. Additionally, the questionnaire explored reasons for not adhering to the current recommendations. The questionnaire was structured to prevent incomplete submissions and minimize missing data.
The instrument was drafted in Indonesian language and underwent rigorous content review by 3 pediatric asthma specialist (RT, EO, and SAKI), with revisions made accordance with the expert recommendations. The reliability of the questionnaire was assessed using Cronbach’s alpha, which yielded a value of .803. This indicates good internal consistency, suggesting that the items in the questionnaire are well correlated and effectively measure the intended constructs.
The questionnaire was distributed as a Google Form link shared with all registered IPS members. Responses were automatically recorded in a spreadsheet and collected over a 2-month period.
We then compared the findings with the recommendation outlined in the national guidelines to analyze the gap between policy and practices. The Indonesian national guideline on childhood asthma recommends to establish a diagnosis of asthma based on the algorithm outlined in Figure 1. Spirometry is advised to support the diagnosis if accessible, while routine chest X-ray are not recommended for diagnosing asthma in children. Medical management should be based on the severity of asthma—intermittent or persistent. For children with persistent asthma, controller therapy is recommended, with inhaled steroid as the first-line option. These can be delivered via metered dose inhaler (with spacer) or dry powder inhaler, depending on the child’s age. The recommended reliever is SABA administered via inhaler or nebulizer.

The Indonesia algorithm for diagnosis asthma in children. 14 (a) If spirometer not available, use peak flow meter (PFM). (b) Suggestive for asthma: FEV1 <80%; FEV1/FVC <90%; BDR > 12%: PEF variability > 13% (spirometry may be normal in patients with asymptomatic intermittent asthma).
Statistical Analysis
The data was analyzed descriptively. Categorical variables are presented as proportion, while continuous variables are expressed as means or medians, as appropriate. All data were analyzed using Stata version 14.1 (Stata, RRID:SCR_012763).
Ethical Approval and Informed Consent
This study was approved by the Ethics Committee, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia, under reference number KE/FK/0875/EC/2022. As the survey was conducted anonymously and participation was entirely voluntary, informed consent was not required for this study.
Results
Responses were received from 1386 pediatricians participated in the survey, representing 28.8% of the 4813 total pediatricians registered in the IPS database during the study period. Among them, 35 were pediatric respirologists, highlighting representation from specialists with advanced expertise in managing pediatric asthma (Table 1). Participants were from 37 of 38 provinces in Indonesia with approximately 45% of them were based in Java and Bali Islands, regions known for having better healthcare resources (Table 2).
Characteristics of the Participants.

Availability of Modalities for Diagnosis and Management of Childhood Asthma in Indonesia.

Abbreviations: PICU, pediatric intensive care unit.
Table 2 highlight the regional disparities in the availability of essential asthma diagnosis and management resources, suggesting a need for targeted interventions to improve access and ensure optimal and uniform asthma care for children across Indonesia. Nebulizers and inhaled reliever medications were widely available in all provinces, with close to or 100%. However, the availability of spirometers was low across all provinces, with the highest in Java (15.7%) and none in Maluku. In addition, only 225 (16.2%) pediatricians having used spirometer to support a diagnosis of asthma. In contrast, a high proportion of pediatricians performed routine blood count examination (82%) and chest X-ray (84.8%) to diagnose asthma, which is not recommended in the national guideline (Table 3).
Investigations Performed by Participants in Diagnosing Asthma.

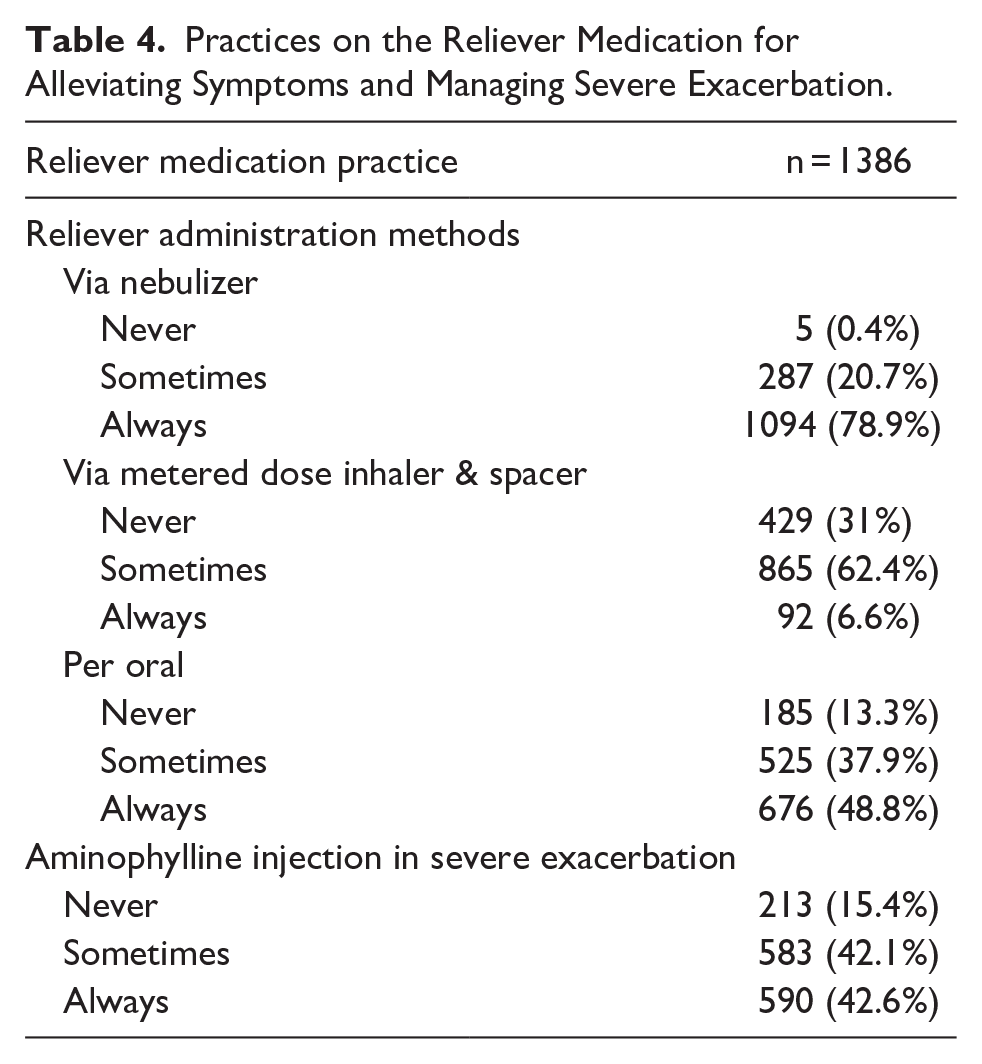
The availability of inhaled corticosteroids medication was a concern in all provinces, with only around 40% of pediatricians reported the availability in their settings. In line with this, spacers were less available. Pediatricians outside Java and Bali reported more challenges, particularly in Nusa Tenggara, Papua, and Maluku. Among those who did not prescribe inhaled corticosteroids to their patient as asthma controllers, the reasons included a lack of eligible patients for controller therapy (62.6%), the medications not being covered by the national insurance (54.8%), unavailability of the medication (59.8%), parental refusal (21.2%), and a lack of confidence in prescribing inhaled controllers (16.6%). In contrast, nearly 90% of the pediatricians reported prescribing oral β2-agonist as reliever, a practice inconsistent with the guidelines (Table 4).
Practices on the Reliever Medication for Alleviating Symptoms and Managing Severe Exacerbation.
The gaps in diagnosis and management of asthma in children between recommendation outlined in the national guidelines and the actual practices are summarized in Table 5.
The Gap Between National Guidelines and Current Practices, Along With Recommended Solutions.

Discussion
Local guidelines on childhood asthma are frequently developed by LMICs based on the updated global recommendation. However, these guidelines are frequently not accompanied by adequate dissemination and training for healthcare providers in rural areas. In addition, the updated guidelines often do not account for the resources limitations in these regions. Consequently, this leads to suboptimal and inappropriate diagnosis and further management. Our study highlight the gaps between policy and practice in the management of childhood asthma in Indonesia. The low utilization of spirometer, reliance on chest X-rays and complete blood count for diagnosis, and common prescription of oral medications as relievers are concerning findings that inconsistent with the national guidelines. The lack of inhaled corticosteroids for controller medication in many provinces further hinders appropriate management. While similar issues have been documented in other developing countries, this study is the first to highlight these specific gaps in Indonesia. The result underscore the urgent need for targeted interventions to bridge the gap between the recommendation and actual practice, not only in Indonesia but also globally.
Diagnosis of asthma can be made clinically, but performing spirometer in patient with asthma is essential for effective and optimal management and treatment. Spirometry is an important tool to demonstrate reversible airway obstruction, which is a hallmark of asthma. In addition, spirometry helps to assess the severity of the disease, to monitor disease progression and the effectiveness of treatment, ensuring that management strategies are adjusted as necessary. Yet its use in developing countries faces several challenges. Spirometer are often unavailable in many health facilities due to cost, lack of infrastructure, and maintenance issue.15,16 Shortage of trained staff and clinicians is also the barriers. The high cost of spirometer and related consumables, combined with limited healthcare budgets, restricts widespread use. Additionally, economic constraints may limit patient access to healthcare facilities where spirometry is available.17,18 In childhood asthma, these challenges are complicated with the difficulties in performing spirometry in young children, under 6 years of age. Addressing these challenges through targeted interventions, training and resource allocation is essential to close this gap.
Chest X-rays are frequently utilized in the evaluation of children with respiratory problems. However, their role in the diagnosis of asthma is limited and remains a subject of debate. Routine chest X-rays are not recommended for the diagnosis of asthma, but are warranted in cases of severe acute asthma to identify potential complications such as pneumothorax, pneumomediastinum or atelectasis, or to investigate comorbid condition like pneumonia.19,20 A study in Abu Dhabi evaluated the use of chest X-ray in 243 children with asthma exacerbation, revealed that 88% of the children underwent chest X-ray, and only 18% of them had focal/multifocal pneumonia on the chest X-ray. 21 Chest X-rays may also be performed to rule out conditions that present with similar symptoms to asthma, such as pneumonia, congenital heart diseases, foreign body inhalation, or other structural lung abnormalities. This context may explain our findings, where chest X-ray are commonly employed to diagnose asthma in children. Nevertheless, clinicians should use chest X-rays judiciously, guided by clinical indications, and relay primarily on clinical evaluation and spirometry for asthma management. Beside the risk of radiation, there is a significant correlation between requesting chest X-ray and the use of antibiotics. 21
The management of patient with asthma in LMICs are commonly suboptimal, most of the patient do not receive guideline-based therapy, as documented in our study. 22 Inhaled corticosteroids are pivotal for the effective management of childhood asthma, offering significant benefits in controlling symptoms and preventing exacerbations. Despite the long-standing recommendation, global use of controller therapy remains limited. Results from REcognise Asthma and Link to Symptoms and Experience (REALSIE) Asia, Asthma Insights and Management (AIM), and Asthma Insights and Reality (AIR) survey have shown that less than one-third of children and adults with asthma in the Asia Pacific Region use daily controller medications, while more than two-thirds rely solely on reliever medication.6,23,24 Among school-aged children in Indonesia who were identified to have asthma through asthma survey using ISAAC questionnaire, less than 5% had been prescribed with inhaled corticosteroids for their asthma. 7 Similarly, in India only 6.8% of asthma patients all ages groups were prescribed inhaled corticosteroids. 25 In South Africa, only 38% of adult with mild asthma were prescribed inhaled corticosteroids. 26 Challenges contributing to limited used of inhaled corticosteroids for children with asthma in Indonesia are the same as previously described, which span from factors related to accessibility, healthcare infrastructure, policy, patients, and doctors. More global and comprehensive strategies and interventions is of importance to address these challenges.
The use of reliever medications in asthma is also problematic. Prescription of SABA is more common than inhaled corticosteroids, with a global trend of overusing SABA globally. The SABINA (SABA use IN asthma) III study in Asia revealed over-prescription of SABA (>3 canisters/year) in 26% of asthma patients aged >12 years. 27 This overuse of reliever medications has been linked to severe exacerbations and poor clinical outcome, contributing to inadequate asthma control in Asia and other LMICs. 27 Additionally, the use of oral reliever medications remains common. Our study found that 90% of the pediatricians prescribed oral salbutamol as reliever medication. An audit for asthma prescriptions in a tertiary hospital in Gujarat, India found that 93% of the asthma prescription contained oral methylxantines and 28% included oral salbutamol. 28
We have identified gaps in the management of asthma in children, characterized by disparities among different socioeconomic groups, populations (across regions, provinces, rural-urban areas), and age groups. These gaps include unequal treatment in terms of access and affordability of recommended inhaled medication, as well as communication and care across primary, secondary, and tertiary healthcare levels. Generally, patients in urban areas had better access to medication and diagnostic facilities compared to those in rural areas. Consequently, the pediatricians in rural areas rely more on clinical judgment and basic equipment for diagnosis and treatment, which potentially leading to underdiagnosis, undertreatment, and inadequate asthma control. 19 Our study underscores significant impact of the availability of asthma medication and diagnostic facilities on how pediatricians managed asthma. This highlights the urgency for a national asthma strategy that incorporate political commitment, asthma education, and provision of affordable asthma medications for the pediatric population. 21
This study has several potential limitations that should be acknowledged. First, although the survey was distributed to all members of IPS, underrepresentation of certain groups remains a potential limitation, particularly for pediatricians in remote areas or those with limited internet access. This may have resulted in a bias toward responses from urban or resource-rich settings. Furthermore, this may lead to geographical bias and failing to capture the full spectrum of sources and practices across Indonesia. Secondly, there was potential for voluntary response bias, as participation was self-selected. This may have resulted in overrepresentation of pediatricians with greater interest or access to resources for managing asthma, while underrepresentating those with limited knowledge or practice in this area. Future studies should employ more systematic sampling methods to improve representativeness. Lastly, the reliance on self-reported data from an online survey poses challenges in verifying the accuracy or authenticity of the responses
Conclusion
This study addresses the identified gaps between policy recommendations and actual practice in the management of childhood asthma in Indonesia, which may be due to disparities of knowledge and sources, as well as access to proper asthma medication. Closing this gap is crucial to develop more appropriate strategy to improve asthma outcome in children. While this study provides valuable insights into the current practices and challenges in the management of childhood asthma in Indonesia, this also may reflect the situation in other developing countries. Global efforts and innovations are needed to overcome the longstanding barriers and challenges of childhood asthma management in developing countries.
Footnotes
Acknowledgements
Board and Members of Indonesia Pediatric Society.
Author Contributions
RT: contributed to conception or design; contributed to acquisition, analysis, or interpretation; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. EO: contributed to conception or design; contributed to acquisition, analysis, or interpretation; drafted the manuscript; critically revised the manuscript; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SAKI: contributed to conception or design; contributed to acquisition, analysis, or interpretation; drafted the manuscript; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. FFY: contributed to conception or design; drafted the manuscript; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. FS: contributed to conception or design; drafted the manuscript; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. RAS: contributed to acquisition, analysis, or interpretation; drafted the manuscript; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. MSA: contributed to acquisition, analysis, or interpretation; drafted the manuscript; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. RF: contributed to acquisition, analysis, or interpretation; drafted the manuscript; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study obtained ethical approval (reference number: KE/FK/0875/EC/2022) from the Ethics Committee, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia.