
Abstract
Introduction. Despite the global decrease, the neonatal mortality rate has remained high in sub-Saharan Africa, including Somalia. There is a need to continually identify and localize the drivers of neonatal mortality to help policy interventions aimed at its reduction. This study estimated the prevalence of and factors associated with Neonatal Mortality among newborns attending Banadir Hospital 2023. Methods. A facility-based cross-sectional study was conducted among 1435 neonates admitted to the neonatal intensive care unit (NICU) of Banadir Hospital from January to December 2023, and data were extracted from the medical charts and through a structured questionnaire administered to the parents. Descriptive and logistic regression analyses were performed to identify the factors associated with neonatal mortality. Results. The median age of the neonates was 1 (IQR: 1-6) days, 59.4% (853/1435) were male, 54.5% (782/1435) were born at Banadir Hospital, 25.6% (95% CI: 23.5-28.0, 368/1435) newborns died before discharge. The median age of the mothers was 27 years (IQR: 23-30) years. The majority of the mothers 1127 (78.5%) were multiparous, 50.7% (728/1435) had no ANC follow-up, and 79.4% of the neonates stayed at the hospital <7 days. Mother’s education (aOR: 0.01; 95% CI: 0.01-0.05), parity (aOR: 9.7; 95%: 5.33-17.7), age of the baby (aOR: 0.23; 95% CI: 0.13-0.39), gestational age (aOR: 7.12; 95% CI: 2.61-19.33), history of chronic disease (aOR: 0.2; 95% CI: 0.06-0.41) and History of abortion (aOR: 0.2; 95% CI: 0.11-0.31) were significantly associated with neonatal mortality. Conclusion. The prevalence of neonatal mortality is high. Neonatal mortality was associated with mother’s education, parity, prematurity, history of abortion, history of chronic disease, and being less than 7 days of life. Improved maternal education, early management of preterm birth, and newborn illnesses should be priorities for reducing neonatal deaths.
Introduction
Neonatal mortality, defined as death within the first 28 days after birth, plays a vital role as a fundamental indicator for evaluating the health and well-being of newborns. This indicator requires special attention from health authorities because of its significance in comprehending and addressing the unique challenges faced during the early infancy period. 1
The global neonatal mortality rate (NMR) decreased by 43% from 31 deaths per 1000 live births in 2000 to 18 deaths per 1000 live births in 2021. 2 In Sub-Saharan Africa, a child born is 11 times more likely to die in the first 28 days of life, with 22 deaths per 1000 live births, compared to those born in Australia and New Zealand. 3
The Sustainable Development Goals (SDGs-3) have set a target to lower the burden of newborn mortality by 2030 to 12 deaths per 1000 live births. 4 Efforts to achieve this target involve implementing various approaches and policies worldwide, specifically targeting the reduction of mortality among newborns, infants, and children under the age of 5. 5
Previous studies have extensively investigated factors associated with neonatal mortality, revealing several significant predictors. Factors such as sepsis,6,7 respiratory distress syndrome, 8 low socioeconomic status,9,10 cesarean section delivery,8,9 preterm birth, 9 low birth weight,10,11 low Apgar scores, 8 and age at admission 8 are recognized as significant contributors to neonatal mortality.
Somalia ranks among the countries with the lowest global health indicators. 12 The devastating impact of several decades of civil war has severely weakened Somalia’s healthcare system, leading to significant challenges. 12 However, the newborn mortality rate in Somalia has dropped gradually from 45.4 deaths per 1000 live births in 2002 to 36 deaths per 1000 live births in 2021. In 2021, the rate of was 36/1000 live births.13,14
Therefore, this study was designed to evaluate the prevalence of neonatal mortality and associated factors at Banadir Maternal and Child Hospital, a national referral Hospital in Mogadishu, Somalia.
Methods
Study Setting
The study was performed at Banadir Hospital, a mother-and-child referral teaching hospital located in Mogadishu, Somalia’s capital city. The hospital is run by the Minister of Health (FMOH) and has a 700-bed capacity. Employees with over 501 staff members offer specialized pediatric services, including neonatal intensive care, where it manages newborns needing specialized care and preterm babies. The neonatal intensive care unit (NICU) is equipped with incubators, radiant warmers, phototherapy, machines, infusion pumps, syringe pumps, oxygen cylinders, and neonatal resuscitation essential for caring for neonates with special care needs. The Banadir Hospital receives high-risk neonates and children from different parts of the country.
Study Design and Population
A prospective cross-sectional study was conducted to investigate the prevalence of neonatal mortality rates and associated factors. The study applied a convenience sampling technique, selecting all neonates admitted who met the predetermined inclusion and exclusion criteria during the designated study period so the target population consisted of neonates admitted to the NICU for any reason from 1st January to 31st December 31, 2023. Neonates who were immediately referred to specialized health facilities for further management were excluded from this study because of the difficulty in measuring their outcomes. In total, 1488 newborns were admitted to the NICU. Of these, 53 patients were deemed ineligible for participation in the study due to incomplete records; therefore, 1435 patients who fulfilled the study’s inclusion criteria were included.
Data Collection
Data were collected by reviewing medical charts and through a structured questionnaire administered to parents. The variables collected included clinical diagnosis at admission, sex, maternal and neonatal age, level of education of mother, gestational age, number of antenatal care visits, birth weight, place of birth (BH or other), mode of delivery, and outcome (alive/death).
Data Analysis
After data cleaning, SPSS v26 was used for data analysis. Frequencies and percentages were calculated for all variables. Bivariate binary logistic regression analysis was performed to assess the association between each independent variable and outcome variable. All variables with a value of P < .05 during bivariate analyses were considered for multivariable logistic regression analysis. Odds Ratios (OR) with 95% Confidence Intervals (CI) were calculated to assess the association between dependent and independent variables. Variables with P-values less than 5% were considered statistically significant.
Ethics Consideration
This study was approved by Ethics and Research Committee of Somali National Institute of Health with approval number (Ref: NIH/IRB/06/MAR/2024). Prior to data collection, informed, voluntary, written, and signed consent was acquired from the administrators of Banadir Hospital. All collected data were rigorously maintained in confidentiality and will not report the data to the public as an individual level but will be as aggregate findings form.
Results
Out of 1435 neonates included, 59% (853/1435) were male, 54.5% (782/1435) were born at Banadir Hospital, 36% (513/1435) were preterm (Table 1). The median age of the mothers was 27 years (IQR: 23-30) years. The majority of the mothers, 78.5% (1127/1435) were multiparous, 50.7% (728/1435) had no ANC follow-up, and 71.7% (1030/1435) had a spontaneous vaginal delivery (SVD). Of all admitted neonates, 79.4% of the neonates stayed at hospital <7 days. (Table 1)
Socio-Demographic Characteristics of the Respondents at Banadir Hospital, From January to December 2023 (N = 1435).

Prevalence of Neonatal Mortality
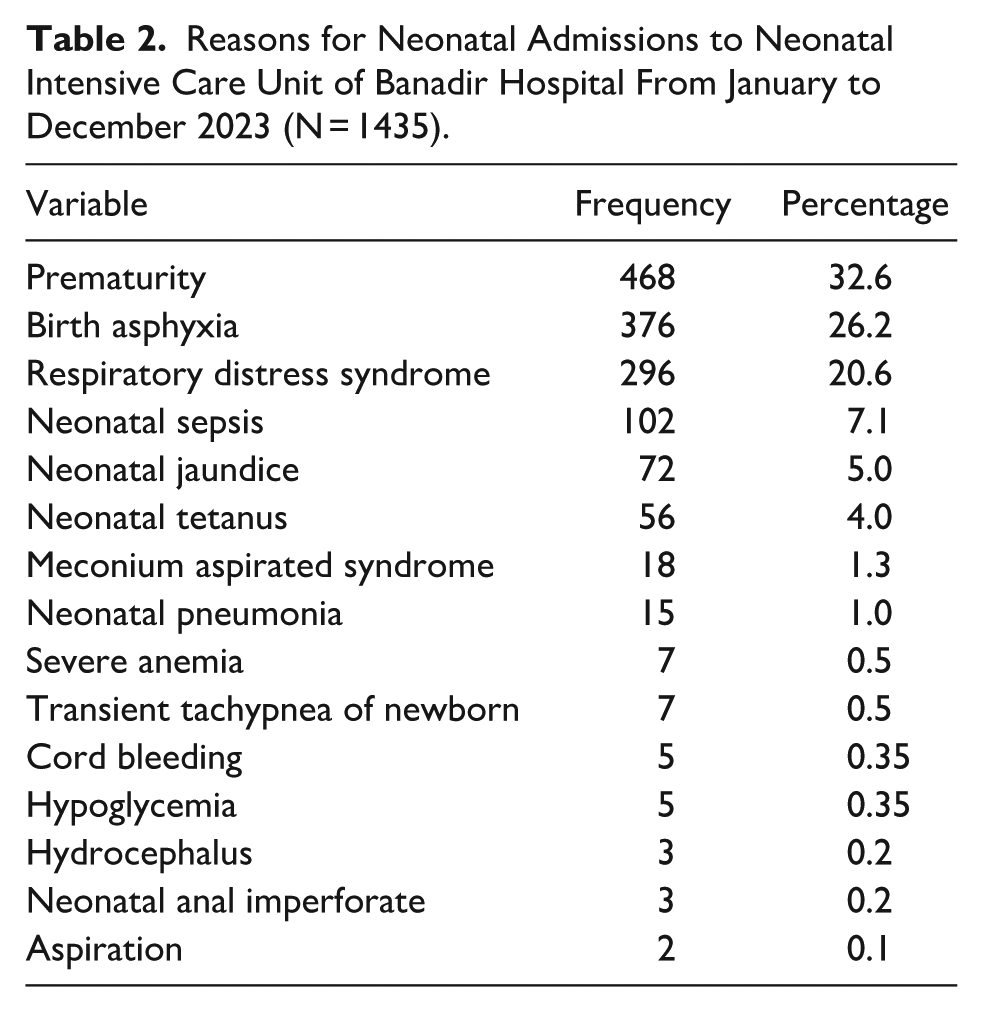
A total of 368 (25.6%) of the newborns died before discharge. Therefore, the prevalence of neonatal death was 25.6% (95% CI: 23.5-28.0). The majority, 230/368 (62.5%) of the neonates died within 7 days of life. A total of 468 (32.6%) neonates were admitted with prematurity, 376 (26.2%) with perinatal asphyxia, and 296 (20.6) with respiratory distress syndrome Table 2).
Reasons for Neonatal Admissions to Neonatal Intensive Care Unit of Banadir Hospital From January to December 2023 (N = 1435).
Pattern Associated with Neonatal Mortality
Variables such as maternal education, ANC, TD vaccination, chronic disease, history of abortion, history of neonatal death, maternal parity, sex of newborn, age of the baby, mode of delivery, and gestational age were significantly associated with bivariate logistic regression. In multiple logistic regression analysis, neonatal mortality was significantly associated with Education of mother (AOR: 0.1; 95%: 0.03-0.08), history of neonatal death (AOR: 0.4; 95%: 0.20-0.71), chronic disease (AOR: 0.2; 95%: 0.06-0.41), history of abortion (AOR: 0.2; 95%: 0.11-0.31), maternal parity (AOR: 9.7; 95%: 5.33-17.7), age of the baby (AOR: 0.23; 95%: 0.13-0.39), and gestational age (AOR: 7.12; 95%: 2.61-19.33) (Table 3).
Factors Associated With Neonatal Mortality Among Newborns Admitted at Banadir Hospital.

Abbreviation: Hx, History.
P-value less than .05 is typically considered to be statistically significant.
Chronic diseases, such as hypertension, diabetes, asthma, liver disease, and renal disease.
Discussions
We observed a high neonatal mortality rate among newborn babies admitted to the neonatal intensive care unit at the Banadir Maternal and Child Hospital. This was expected from the hospital-level study, given that these were referral hospitals that received high-risk cases with poorer prognoses. Despite the high levels observed, the value was found to be lower than the previously reported national level, 13 which was similar to that reported in a study conducted in South-West Ethiopia 15 but higher than that reported in studies conducted in Ethiopia16,17 and Mauritania. 18 The high percentage of neonatal deaths can be explained by the absence of adequate health services, which may result in insufficient prenatal care. Limited access to health care, skilled birth attendants, and poor parental health-seeking behavior. In addition, Banadir Hospital is the main referral hospital in the country, and most patients were transferred from another hospital.
After multivariate logistic regression, several factors were found to be significantly associated with neonatal death, such as mother’s education, parity, previous history of neonatal death, mother with chronic disease, history of abortion, baby age less than 7 days, and gestational age <37 weeks (premature).
Prematurity remained the strongest predictor of neonatal death. This finding is in line with those of a study conducted in Ethiopia15,19 and Somalia. 20
Likewise, Mothers with informal education had a higher risk of neonatal death than mothers with formal education. This finding is supported by those of studies conducted in Nepal 21 and Indonesia. 22 The role mother’s education and by extension girl child education has been on child survival and well-being have been well documented. Mothers with formal education are more likely to take precautions, attend ANC, recognize danger signs of pregnancy, and seek health care early to protect the child and her health.
In this study, neonates born to multiparous mothers had higher odds of neonatal mortality than those born to primipara mothers. This finding is consistent with that of other studies conducted in Nepal 21 and Morocco. 23 This could be because as the family size grows, parental resources might be insufficient to maintain the proper level of nutrition for more children, and the mother herself could be undernourished during pregnancy.
The findings of this study also showed that low gestational age was significantly associated with neonatal death, which is supported by other studies in Morocco 23 and Indonesia. 22
Neonates born to mothers who did not receive antenatal care (ANC) consultations had a higher likelihood of neonatal death than those born to mothers who had ANC consultations. This finding is supported by a study carried out in Ethiopia, 24 for ANC follow-up, mothers were aware of postpartum care, newborn care, neonatal warning signs, and pregnancy warning signals.
The results of our study demonstrated that mothers with chronic diseases were more likely to understanding neonatal death compared to mothers without chronic conditions. Several studies conducted elsewhere have confirmed this finding. 25
The results of our study indicated that mothers with a previous history of neonatal death were more likely to experience neonatal death compared to mothers without a history of neonatal death. 26
Our study’s findings revealed that mothers with a history of abortion had an increased risk of neona-tal death compared to those without a history of abortion.26,27
Lastly, neonates with less than 7 days of gestation had a higher risk of death than their counterparts. This finding is consistent with those reported by the World Health Organization. 28
The limitation of this study is that it might not have a cause-effect relationship because the study design was cross-sectional. The study was conducted in a single referral hospital, which limits its generalizability as it does not distinguish between inborn and referral cases. Additionally, our study utilized an adapted questionnaire that was neither validated nor pilot-tested. Future research should prioritize the development and validation of standardized tools specifically tailored to the study population to enhance the robustness and applicability of the results.
Conclusion
Mothers with no education, multipara history of neonatal death, baby age less than 7 days, and gestational age <37 weeks (premature) were significantly associated with neonatal mortality in the NICU Banadir Hospital, Mogadishu Somalia. Therefore, improving maternal education regarding ANC, early management of preterm birth, and newborn problems should be top priorities for tracking local neonatal deaths. Designing approaches to the associated burdens and understanding the characteristics relevant to particular contexts are also important.
Footnotes
Acknowledgements
We gratefully acknowledge the priceless assistance and guidance of the Banadir Hospital Research Center and the devoted staff of the Neonatal Intensive Care Unit (NICU) without whom this work would not have been possible. Similarly, we extend our sincere appreciation to all authors for their significant contributions.
Author Contribution
Data Availability Statement
The data of this study are available upon request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study was approved by Ethics and Research Committee of Somali National Institute of Health with approval number (Ref: NIH/IRB/06/MAR/2024). Prior to data collection, informed, voluntary, written, and signed consent was acquired from the administrators of Banadir Hospital. All collected data were rigorously maintained in confidentiality and will not report the data to the public as an individual level but will be as aggregate findings form.