
Abstract
Objective
This study assessed the prevalence of refractive error (RE) and its associated factors among elementary school children in Hawassa, Ethiopia.
Methods
In this school-based cross-sectional study, a random selection technique with proportional allocation was used to ensure a representative sample of students. Survey questionnaires were used to collect sociodemographic, environmental, and family history data. Clinical examinations were performed to assess RE and ocular health. Associations between dependent and independent variables were computed using adjusted odds ratios (AORs) and 95% confidence intervals (CIs).
Results
Overall, 529 children participated in this study, with a response rate of 95.5% (529/554). Most participants were aged ≥12 years (337 [63.7%]), in grade levels 5 to 8 (307 [58%]), and attended public schools (366 [69.2%]). RE prevalence was 12.9% (95% CI: 10.0–16.1). Higher grade level (AOR=3.18, 95% CI: 1.68–5.97), positive family history of RE (AOR=3.69, 95% CI: 1.57–8.67), lack of paternal formal education (AOR=3.25, 95% CI: 1.20–8.77), and public school attendance (AOR=3.33, 95% CI: 1.52–7.27) were factors significantly associated with RE.
Conclusions
RE prevalence among elementary school children in Hawassa was higher than in previous reports. Grade level, family history, paternal education level, and school type significantly influenced RE status.
Keywords
Introduction
In refractive error (RE), the eye fails to focus parallel rays of light on the retina; this condition is caused by an imbalance between the axial length and refractive power of the eye. 1 RE is the main cause of visual impairment globally and the second most common cause of treatable blindness regardless of sex, age, or ethnicity. 2 The number of people with RE is increasing worldwide. 3 The World Health Organization reported that 153 million people exhibited visual impairment because of RE in 2004; 4 of these, 12.8 million were children aged 5 to 15 years. 4 In the African nations of Mali, Mauritania, and South Africa, 24% of children aged 5 to 15 years were visually impaired because of RE. 4 Furthermore, of an estimated 19 million children aged <14 years with visual impairment worldwide in 2010, 43% reportedly exhibited RE. 5
Visual impairment from RE can cause impairment of daily activities and poor concentration during educational activities. 6 It also enhances the risks of ocular diseases 7 ; disrupts binocular vision; 8 and reduces intellectual development, maturity, and future personal performance. Poor school performance and unemployment can further reduce the quality of life and contribute to low economic status among individuals, families, and societies. 9 RE is easy to treat, although it cannot be entirely prevented. It can be diagnosed, measured, and corrected in a cost-effective manner;10 early diagnosis by routine eye examination enables prompt treatment with corrective spectacles or contact lenses, as well as plans for refractive surgery. 11
Currently, there is considerable emphasis on the detection and treatment of RE in children. 10 School screening is recommended for areas where RE prevalence is >2%. 12 Early diagnosis and appropriate correction are important for overall visual development, improved academic performance, and prevention of learning disabilities among school children. 13
Various nongovernmental organizations make substantial contributions to eye care services in Ethiopia. However, none are engaged in a national sustainable RE screening program. Most residents of Ethiopia access eye care centers and obtain spectacles for their children after traveling long distances from their homes. The full cost burden is generally carried by the families of affected children.
This study assessed the prevalence of RE and its associated factors among elementary school children in Hawassa, Ethiopia. The findings will help local politicians, policymakers, clinicians, and nongovernmental organizations to establish routine school-based RE screening programs. This early detection of RE will facilitate timely treatment, thus minimizing its lifelong burden among residents of Ethiopia.
Materials and Methods
Study ethical approval, design, and participants
This study protocol received ethical approval from the Institutional Review Board of the Hawassa University College of Medicine and Health Sciences (approval no. IRB/006/08). A support letter and permission were obtained from the Southern Nations Nationalities and Peoples Regional State Education Bureau. The purpose of the study was explained to the heads of selected schools (the selection process is described below). Written informed consent was obtained from each participant’s parents/guardians and written assent was obtained from each child who participated in the study. Students with RE and other ocular pathologies/disorders were referred to the Hawassa University Referral Hospital eye clinic for further evaluation and management. Participant confidentiality was ensured by the removal of personal identifiers from the data.
This school-based cross-sectional study was conducted from April 24, 2016 to May 15, 2016 in Hawassa, Ethiopia (273 km south of Addis Ababa, Ethiopia). Hawassa is the capital city of the Southern Nations Nationalities and Peoples Regional State, with eight sub-cities and 32 kebeles. In Hawassa, there are 37 public and 68 private elementary schools that serve 62,270 students (31,586 boys and 30,684 girls) and 26,321 students (13,441 boys and 12,880 girls), respectively. 14 One public tertiary eye care center and three private higher ophthalmic clinics are present in Hawassa. All children in public and private elementary schools were included in the study, except children with ocular conditions preventing refraction (e.g., bilateral cataract and corneal opacity) and those with chronic illnesses.
The sample size for the determination of RE prevalence was determined using the following single-population proportion formula:

To ensure representativeness, 20% (21/105) of schools were selected using a computer-generated simple random sampling technique. Proportional allocation for each school was computed by using the following formula:


Sampling procedure for elementary school students in Hawassa, Ethiopia
Variables and definitions
In this study, the dependent variable was RE (yes/no); independent variables were sociodemographic factors (age, sex, grade level, school type, parental education levels, and parental occupations), environmental factors (engaging in outdoor activity, reading books, watching television, using a computer, and playing video games), and family history of RE (Figure 2).
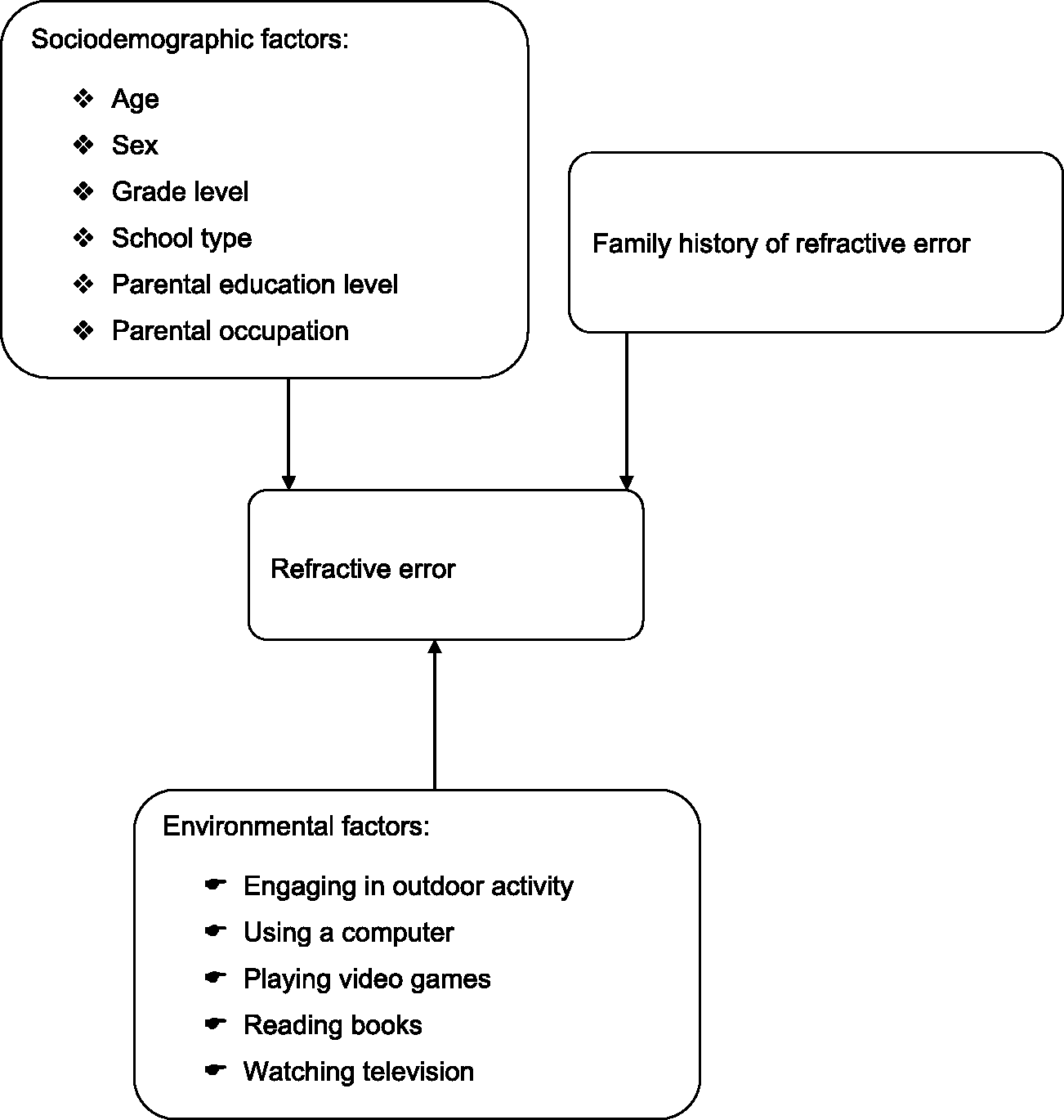
Conceptual framework for assessment of refractive error among elementary school students in Hawassa, Ethiopia
RE was defined as myopia (≥−0.50 diopter sphere) in one eye or both eyes,16–21 hyperopia (≥+1.50 diopter sphere) in one eye or both eyes16,17,20 and/or astigmatism (≥0.50 diopter cylinder) in one eye or both eyes.16,21,22 In accordance with a previous study, longer durations of reading, use of a computer, playing video games, and watching television were each defined as ≥2 hours per day. 23 Shorter duration of engaging in outdoor activity was defined as any outdoor daily visual activity performed for <1 hour. 11 Positive family history of RE was defined as a history of spectacle wear for RE in any family member.
Ocular assessments
Refraction assessment was considered for participants with subnormal vision (uncorrected visual acuity of 6/9 or worse in the worse eye, in the absence of anterior or posterior segment abnormalities that could explain subnormal vision) and/or for participants with low hyperopia who had visual acuity of 6/6 or better with a +1.50 diopter sphere lens. A Snellen E-chart, pen torch, magnifying loupe (2.5X), direct ophthalmoscope, retinoscope, and trial set were used for the determination of RE and other ocular pathologies/disorders. Visual acuity was measured at 6 m in natural daylight under the shade of a tree in the school compound, using a Snellen E-chart. To rule out any vision-reducing pathology in children with vision of 6/9 or worse in the worse eye, anterior and posterior segment ocular examinations were performed using a torch, loupe (2.5X) and direct ophthalmoscope inside a semi-dark room. Retinoscopy and subjective refraction assessments were performed by optometrists. The examination results were collected daily.
Survey of participant characteristics
A pre-tested and structured questionnaire was used during a face-to-face interview to obtain the following participant information: sociodemographic characteristics, environmental factors, and family history of RE. To ensure data quality, the questionnaire was pre-tested on a group comprising 5% of the sample size (28 students) in Leku at the Leku Union Primary School; based on the pre-test information, variables were amended before the actual data collection. A 1-day training was provided to six data collectors and two supervisors. The supervisors and principal investigator also supervised the entire data collection process. The completed questionnaires were collected daily.
Statistical analysis
The data were stored using Epi-Data, version 3.1 (EpiData Association, Odense, Denmark) and analyzed using IBM SPSS Statistics, version 20 (IBM Corp., Armonk, NY, USA). The Hosmer–Lemeshow test was used to check model fitness (a threshold of P>0.05 was considered adequate). Binary logistic regression was performed to identify factors associated with the outcome variable (RE). Those with P-values ≤0.2 were entered into multiple logistic regression. Adjusted odds ratios with 95% confidence intervals were computed to assess the strengths of associations. P<0.05 was considered statistically significant.
Results
Participant sociodemographic characteristics
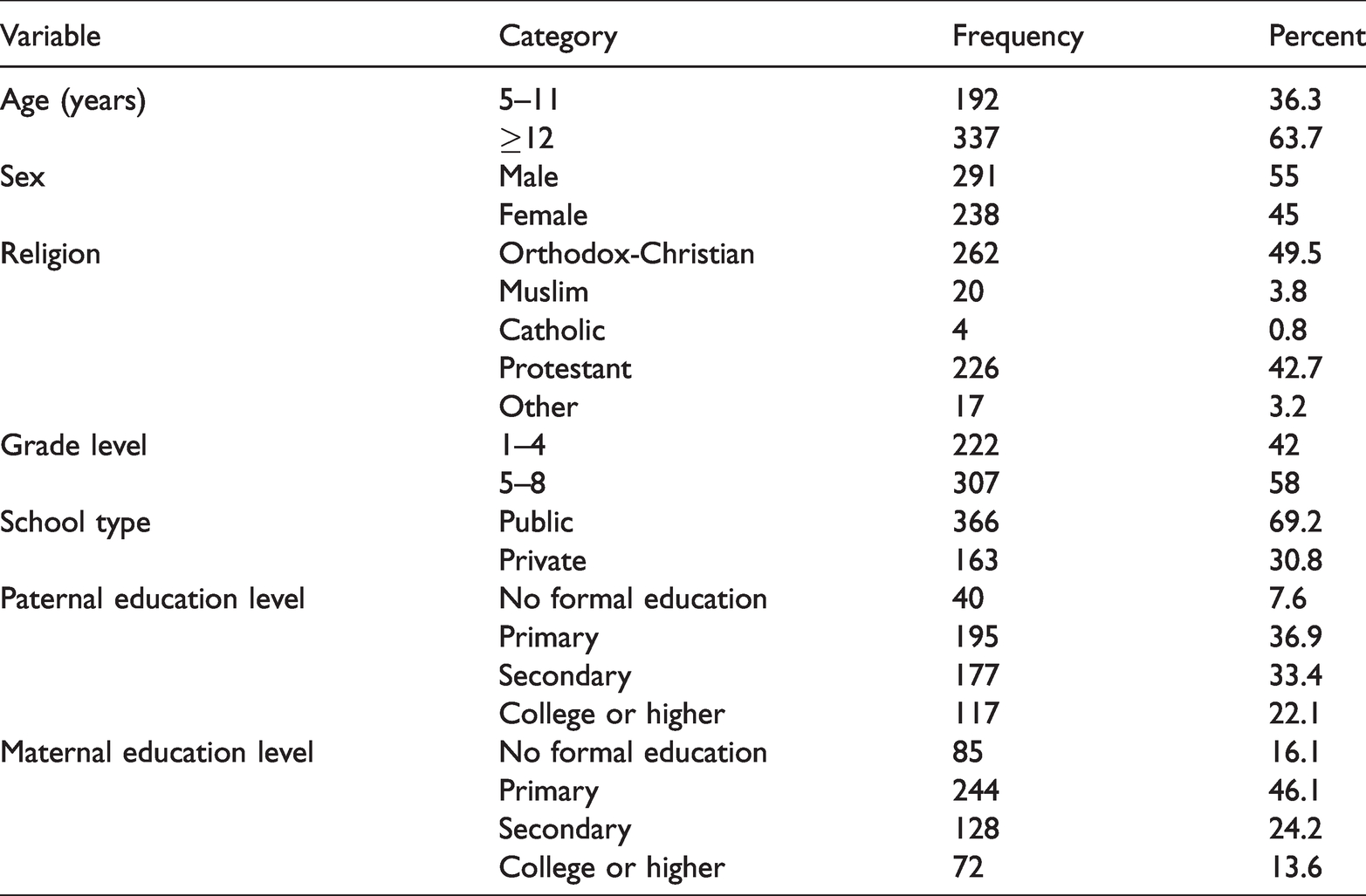
In total, 529 students participated in this study, with a response rate of 95.5% (529/554). The mean participant age (± standard deviation) was 12±2.4 years (range, 5–21 years); the male to female ratio was 1: 1.2. Most participants were aged ≥12 years (337 [63.7%]), in grade levels 5 to 8 (307 [58%]), and attended public schools (366 [69.2%]). Among the study participants, 262 (49.5%) were members of the Orthodox Christian religion. Most parents had only primary education (373 [70.50%]) (Table 1).
Sociodemographic characteristics of study participants (529 elementary school children in Hawassa, Ethiopia)
RE prevalence
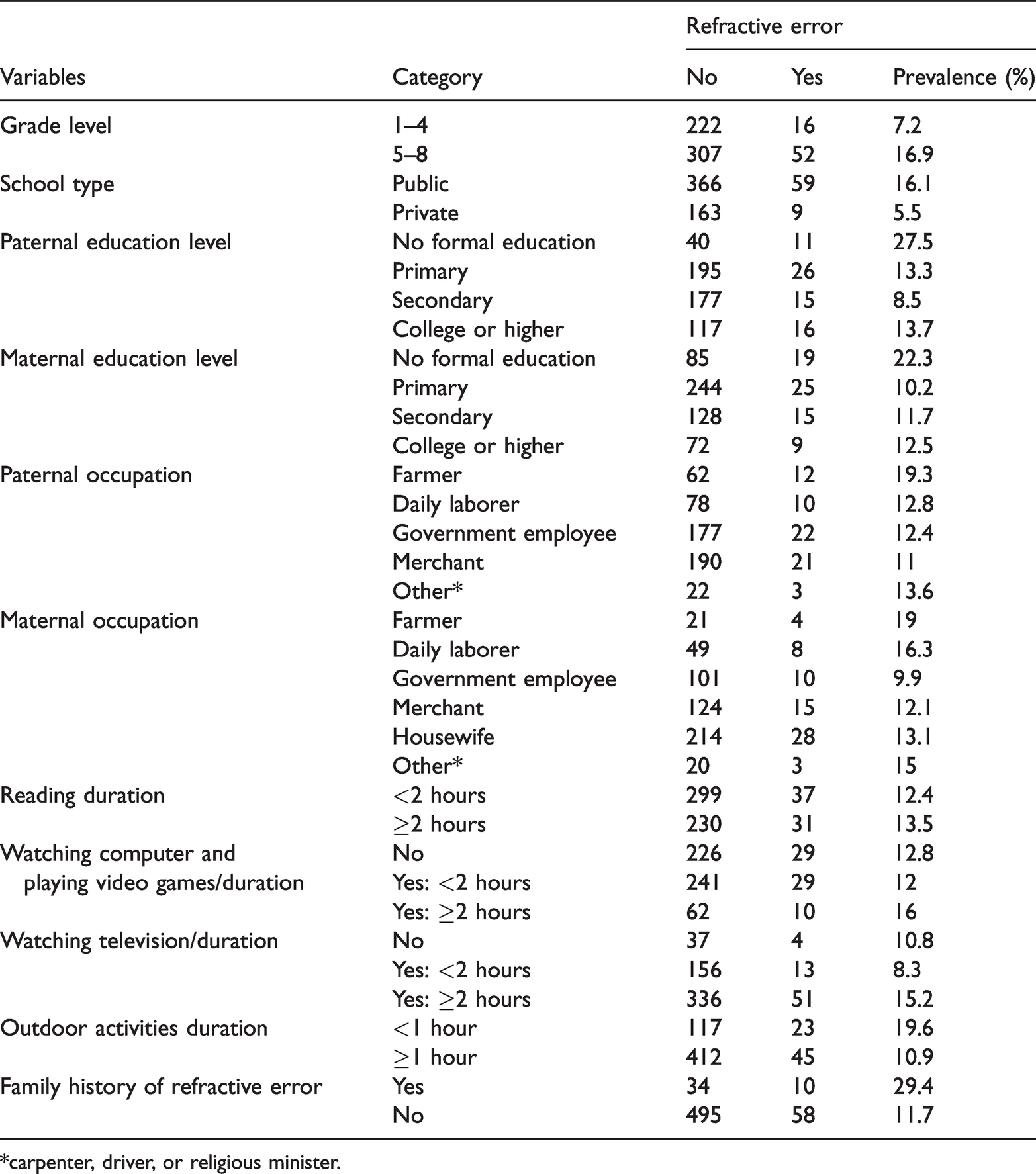
The prevalence of RE was 12.9% (68 students) (95% confidence interval: 10–16.1). Among the affected students, 76.5% had myopia, 14.7% had astigmatism, and 8.8% had hyperopia. The proportions of 5 to 11-year-old students with myopia, astigmatism, and hyperopia were 66.67%, 16.67%, and 16.67%, respectively; these proportions among ≥12-year-old students were 78.57%, 14.29%, and 7.14%, respectively. Among male students with RE, 81.82% had myopia, 12.12% had astigmatism, and 6.06% had hyperopia. Among female students with RE, 71.43% had myopia, 17.14% had astigmatism, and 11.43% had hyperopia. Of the 68 students with RE, 52 were in grade levels 5 to 8 and 59 were public school students. Furthermore, the numbers of students with RE who reported longer durations of reading, using a computer, and playing video games were 31 (13.5%), 10 (16%), and 51 (15.2%), respectively. Finally, 10 (29.4%) students with RE had a positive family history of RE (Table 2).
Refractive error status stratified according to multiple factors among 529 elementary school children in Hawassa, Ethiopia
*carpenter, driver, or religious minister.
Factors associated with RE
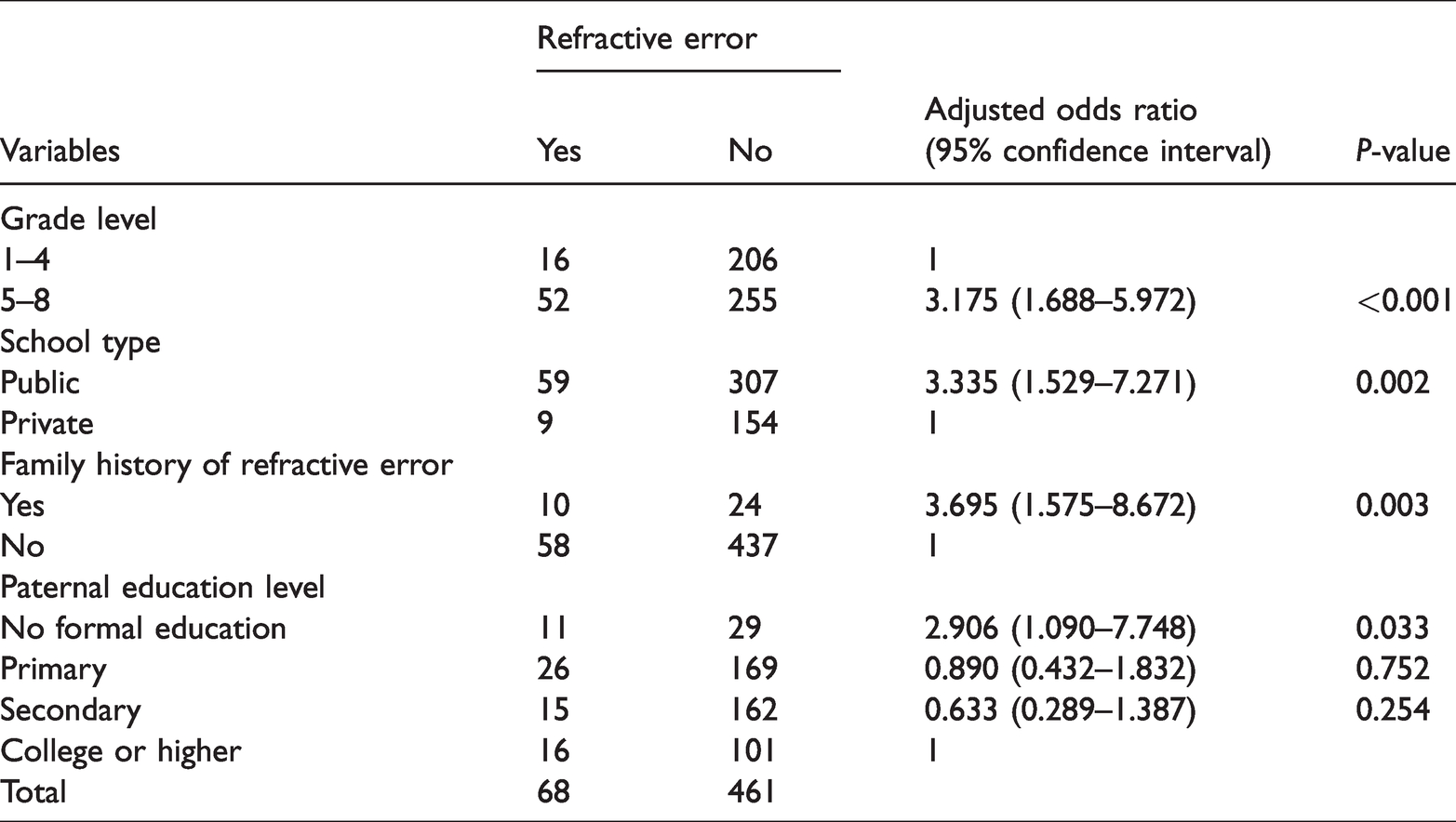
Multivariate logistic regression analysis showed that higher grade level, public school attendance, lack of paternal formal education, and positive family history of RE were associated with a greater risk of RE. Students with a high grade level (5–8) were 3.17-fold more likely to have RE than were those with a low grade level (1–4) (P<0.001). Public school students were 3.33-fold more likely to have RE than were private school students (P=0.002). Students whose fathers had no formal educational were 2.91-fold more likely to have RE than were those whose fathers had college education or higher (P=0.033). Finally, students with a positive family history of RE were 3.69-fold more likely to have RE than were those with a negative family history (P=0.003) (Table 3).
Regression analysis of factors associated with refractive error risk among 529 elementary school children in Hawassa, Ethiopia
Discussion
The prevalence of RE in this study (12.9%) is comparable with prevalences reported in Al-Hassa, Saudi Arabia (13.7%), 22 Ghana (13.3%), 16 Uganda (11.6%), 24 and Debre-Markos, Ethiopia (10.2%). 25 However, the prevalence of RE in this study is lower than prevalences reported in Iran (64.4%), 17 Malaysia (47%), 18 Vietnam (21.4%), 19 and southern India (19.5%). 26 These differences might result from ethnicity-related changes in genetic susceptibility to RE, such that Asian nations tend to have higher prevalences of RE. 27 Notably, the prevalence of RE in this study is higher than prevalences reported in Nigeria (2.2%), 28 Kenya (5.2%), 29 Gondar, Ethiopia (9.4%), 20 Addis Ababa, Ethiopia (4%), 30 and rural central Ethiopia (6.3%). 15 These differences might be due to disparate operational definitions of RE and/or distinct methods of data collection. Furthermore, variations among cultures in terms of norms and attitudes towards spectacle use might be contributing factors.
Myopia (76.5%) was the most common type of RE in this study, which is consistent with the findings in Malaysia, 18 Saudi Arabia, 22 and Nepal. 31 Hepsen reported that excessive near work/activity is a main cause of myopia. 32 Astigmatism (14.7%) was the second most common type of RE in our study, as in Nepal; 31 however, it was the most common type of RE in studies performed in Ghana 21 and Kampala. 24 Hyperopia (8.8%) was the least common type of RE in this study, similar to findings in Debre Markos, Ethiopia 25 and Nepal. 31
Participants in higher grade levels were approximately threefold more likely to have RE than were participants in lower grade levels (Table 3), which is consistent with findings in Egypt. 33 This is presumably because vision demand increases with grade level. In particular, smaller font size is used in coursework at higher grade levels, which leads to overuse of the eye’s focusing mechanism and causes blurred distance vision. 31 In this study, students with a positive family history of RE were 3.69-fold more likely to have RE than were those with a negative family history; this result is consistent with findings in a study of Egyptian school children 33 and a study in Nakhon Pathom Province, Thailand. 34 We suspect that these findings were related to genetic factors that predisposed children to develop RE. Importantly, students whose fathers had no formal education were 2.91-fold more likely to have RE than were those whose fathers had college education or higher. This is presumably because those fathers could not gain sufficient information concerning RE and its correctability; moreover, they might have been financially limited and unable to pay for eye examinations and/or spectacles. This result conflicts with the findings of a study in Ghana, 21 potentially due to differences in the study setting. Finally, public school students were 3.33-fold more likely to have RE than were private school students; we speculate that the families of students who attend private schools have better economic statuses, thereby facilitating eye examinations and subsequent RE correction. Teachers in private schools also have better relationships with their students, which may aid in identifying children with vision problems and informing their families. This result contradicts the findings in Jhapa, Nepal, 31 presumably because of differences in the participants’ socioeconomic statuses.
This study had some limitations. First, it included some >18-year-old students who had repeated grades and/or began school attendance late because of family-related problems; this may have interfered with our ability to draw conclusions based on findings from children aged ≤18 years. Second, some participants experienced discomfort related to some of the locations used for data collection, which may have led to bias in the results.
Conclusions
The prevalence of RE among elementary school children was higher in Hawassa, Ethiopia than in previous studies performed in African countries. Higher grade level, positive family history of RE, lack of paternal formal education, and public school attendance were factors significantly associated with a greater risk of RE. Therefore, eye examinations are recommended for children before they begin attending school in Ethiopia. Moreover, regular vision screenings are needed in schools to reduce the prevalence of uncorrected RE among children in Ethiopia.
Footnotes
Acknowledgements
We thank the Southern Nations Nationalities and Peoples Regional State Education Bureau and Hawassa City Elementary School heads for facilitating the necessary conditions for data collection.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by Hawassa University.
Author contributions
KA: acquired the funding, managed resources, administered the project, and supervised the data collection. EG: entered data and performed analysis. Both authors performed conceptualization, investigation, writing the original draft, and reviewing and editing of the manuscript.