
Abstract
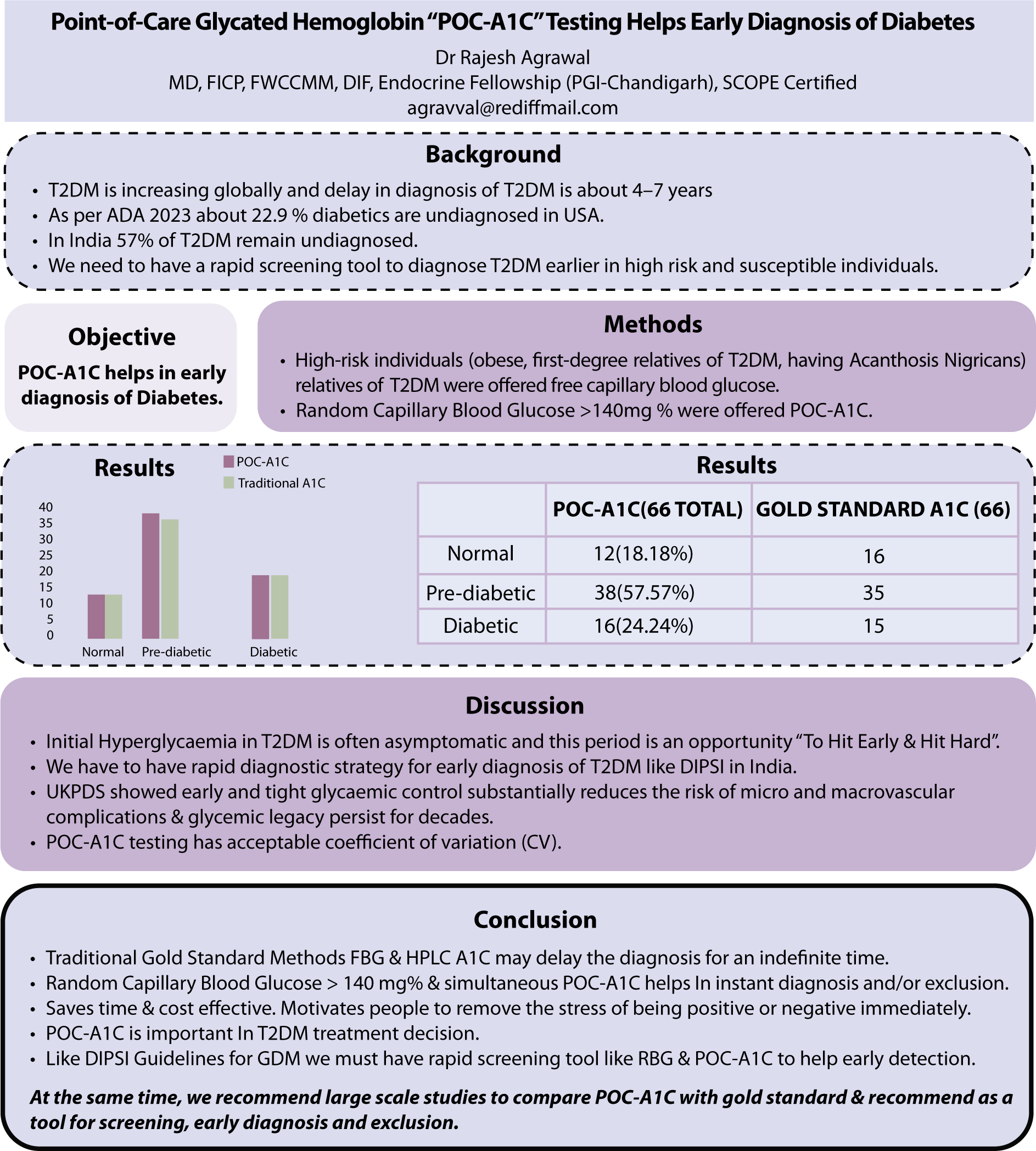
Just like the DIPSI Guidelines for GDM in India, we must have a rapid screening tool like POC-A1c, which gives an estimate of long-term hyperglycemia and helps early detection. Traditional gold standard methods may delay the diagnosis for an indefinite time, as we have seen in our observations that of those who did not opt for POC-A1c, about 34% did not turn up even after three months. We infer that random capillary blood glucose (with a history of meal timings) of more than 140 mg% using POC-A1c helps in instant diagnosis accuracy of about 93%, or exclusion and necessary action can be taken immediately compared to traditional gold standard methods.
It also saves time and is cost-effective as no preparation is required, transportation can be avoided, and it also removes the stress or burden of being positive immediately. We know the important role of POC-A1c in treatment intensification or deintensification in the management of known T2DM patients. We also know that POC-A1c is not recommended for the diagnosis of DM by ADA, but evidence suggests we can opt for RPG and POC-A1c to screen and confirm or exclude T2DM.
At the same time, we also recommend large-scale cross sectional studies to recommend POC-A1c as a tool for early screening and diagnosis and definitely reconfirmation is always possible and can be recommended.
Get full access to this article
View all access options for this article.