
Abstract
Background:
Type 2 diabetes mellitus (T2DM) is growing in an epidemic manner across the world with an expected doubling of the incidence to millions of affected individuals in the last decades. At present, adequate data are not available regarding the ACE and FABP2 polymorphisms and their susceptibility with T2DM cases in the North Indian population. Thus we conceived the need for further study of ACE (I/D) and FABP2 (Ala54Thr) genes polymorphism and its susceptibility to T2DM in the North Indian population.
Materials and methods:
In this study, a total of 300 subjects (including 190 T2DM cases and 110 controls) participated. ACE and FABP2 gene polymorphisms in the cases and controls were evaluated by polymerase chain reaction and restriction fragment length polymorphism.
Results:
The frequencies of ACE I/I, I/D and D/D genotypes in T2DM cases and controls were 28.73%, 55.17%, 16.09% and 13.63%, 57.95%, 28.40%, respectively. The frequencies of FABP2 Ala54Ala, Ala54Thr and Thr54Thr in T2DM cases were 18.39%, 66.66%, 14.94% and 22.72%, 61.36%, 15.90% in controls, respectively. ACE I/I genotype was significantly more frequent in cases as compared to controls (p = 0.003, χ2 = 9.13).
Conclusion:
It appears that the ACE I/I genotype frequency was significantly higher in the T2DM cases as compared to the controls.
Introduction
The estimated global burden of type 2 diabetes mellitus (T2DM) for 2010 would be 285 million people, which is projected to increase to 438 million in 2030; a 65% increase. 1 Similarly, for India this increase is estimated to be 58%, from 51 million people in 2010 to 87 million in 2030. 1 The impacts of T2DM are considerable: As a lifelong disease, it increases morbidity and mortality and decreases the quality of life. 2
The significance of genetic factors in the predisposition to this microvascular complication (retinopathy, neuropathy, etc.) can be realized from the fact that various genes have been implicated in susceptibility to diabetic nephropathy,3,4 including the angiotensin-converting enzyme (ACE) gene of the renin-angiotensin system (RAS). ACE is a dipeptidyl carboxypeptidase that removes the C-terminal dipeptide from angiotensin I to produce the potent vasoconstrictor and growth-promoting substance angiotensin I/I. The ACE gene is mapped on chromosome 17q23 encoded by a 21 Kb gene that consists of 26 exons and 25 introns.5,6 Insertion/deletion (I/D) polymorphism (rs 4646994) of a 287 bp Alu repeat sequence in introns 16 of the ACE gene is strongly associated with plasma and cellular ACE levels, and it indicates that the polymorphism may modulate the expression of the ACE gene. 7 Several studies have reported the involvement of the D allele of the ACE gene in hypertension and T2DM in various populations.8–10 In a study carried out on South Indian diabetic nephropathy patients, a significantly high frequency (80.2%) of the D allele was reported compared to T2DM cases with normal urine albumin. 11 The I/I, I/D and D/D genotypes resulting from the polymorphic site of the ACE gene have been shown to have low, intermediate and high plasma expression, respectively. With that, the I/I genotype has been thought to confer protective benefits while the D/D genotype is believed to confer deleterious effects on various disease pathogenetic mechanisms, particularly diabetic nephropathy. 12 In addition, characterization of the ACE I/D gene polymorphism has also been suggested for decision making regarding antihypertensive treatment regimens. 13
Fatty acid binding protein 2 (FABP2) genes play a key role in the absorption and intracellular transport of dietary long chain fatty acids. The gene for FABP2 is located in the long arm of chromosome 4. The G to A polymorphism (rs1799883) of codon 54 results in the substitution of threonine (Thr) for alanine (Ala). 14 Carriers of the Thr54 allele in FABP2 have a twofold greater affinity for the absorption of the long-chain fatty acids than those with the Ala54-containing FABP2. 15 The associations between the FABP2 Ala54Thr polymorphism and increased fasting insulin (FI) concentration, fasting fatty acid oxidation and reduced glucose uptake were identified in Pima Indians, an extreme population with high prevalence rates of obesity and T2DM. 14 Earlier studies have shown that the FABP2 Thr54 allele is significantly associated with higher total cholesterol, with stroke incidence, 16 elevation of fasting and postprandial triglyceride (TG), 17 insulin resistance14,18and nonesterified fatty acid (NEFA) concentrations. 19 Currently, adequate data are not available regarding ACE I and FABP2 genes polymorphism and its susceptibility with T2DM cases in the North Indian population. Thus we conceived the need for further study of ACE (I/D) and FABP2 (Ala54Thr) gene polymorphisms and their susceptibility to T2DM in the North Indian population.
Materials and methods
Patient selection
A total of 190 blood samples of T2DM cases and 110 healthy controls were collected from the diabetic clinic of the Department of Medicine of Era’s Lucknow Medical College and Hospital, Lucknow with prior consent. Data collection was done for each patient on clinical variables, including age, alcohol consumption, body mass index (BMI), height, weight, cigarette smoking, family history, etc. Patients with overnight fasting plasma glucose (FPG) of more than 126 mg/dl on two consecutive events were included in the T2DM category while samples having a fasting blood glucose (FBG) level below 110 mg/dl without family history of diabetes were included in the study as controls. Patients with type 1 presentation, defined as diabetic ketoacidosis, acute presentation with heavy ketonuria (>3+), or uninterrupted requirement of insulin within one year of diagnosis, were excluded. Ethical committee clearances were obtained from the respective departments prior to the recruitment of subjects in this study.
Biochemical estimations
BMI was calculated according to the Quetelet equation by using weight in kilograms/height in meters squared. Serum creatinine (s. creat.) concentration was assessed by a kinetic Jaffe’s method. Fasting plasma glucose (FPG) and random blood glucose (RBG) (glucose oxidase-peroxidase method), serum cholesterol (cholesterol oxidase-peroxidase), serum TG (glycerol phosphate oxidase-peroxidase-amidopyrine method), High-density lipoprotein (HDL) cholesterol (immunoinhibition) were assessed by an XL-300 Transasia Fully Auto Analyzer Transasia, Mannheim, Germany. Very low-density lipoprotein was determined by enzymatic method. Low-density lipoprotein (LDL) cholesterol levels were calculated by using the Friedewald formula. 20 Hemoglobin A1C (HbA1C) was measured using a semiautoanalyzer (Transasia, Mannheim, Germany).
DNA extraction
Five milliliters of peripheral blood was collected from all the subjects in 0.5 M ethylenediaminetetraacetic acid (EDTA) tubes. Genomic DNA was isolated from whole blood using the standard phenol-chloroform extraction method. 21 DNA concentration was determined by spectrophotometer and stored at −20°C.
Analysis of polymorphisms
ACE polymorphism
Polymerase chain reaction (PCR) was employed for genotyping of the ACE I/D polymorphism. Reactions were performed with 10 pmol of each primer: 22 forward primer 5’-CTGGAGACCACTCCCATCCTTTCT-3’, reverse primer 5’-GATGTGGCCATCTTCGTCAGAT -3’, in a final volume of 20 μl containing 3 mM MgCl2, 50 mM KCl, 10 mM Tris-HCl (pH 8.4), 0.5 mM of each dNT and 2U Taq polymerase. PCR amplification was carried out under these conditions: initial denaturation at 94°C for 5 minutes, followed by 35 cycles of denaturation at 94°C for 45 seconds, annealing at 60°C for 1.15 minutes, extension at 72°C for 2.30 minutes and final extension at 72°C for 5 minutes. PCR products were separated on 2.0% ethidium bromide-stained agarose gel and visualized by a UVP BIOLMAGING gel doc system. The products were 490 bp for allele I and 190 bp for allele D (Figure 1).

Agarose gel picture showing PCR products for ACE gene polymorphism. L6: DD genotype, L1, 2, 5: ID genotype, L4: II genotype and L3: 100 bp ladder, L7: blank. PCR: polymerase chain reaction; ACE: angiotensin-converting enzyme; DD: deletion; I: insertion.
FABP2 polymorphism
PCR was employed for genotyping of the FABP2 gene polymorphism. Reactions were performed with 10 pmol of each primer: 23 forward primers 5’-ACAGGTGTTAATAT AGTGAAAAG-3’ and reverse primer 5’-TACCCTGAG TTCAGTTCCGTC-3’, in a final volume of 20 µl containing 0.3 U of Taq DNA polymerase, 10 mmol/l Tris-HCl pH 8.3, 50 mmol/l of KCl, 1.5 mmol/l of MgCl2 and 100 mmol/l of dNTPs. PCR amplification was carried out under these conditions: 35 cycles for 1 minute at 94°C, 1 minute at 5°C and 1 minute at 72°C; the PCR products were analyzed on 2% agarose gel stained with ethidium bromide to certify the proper amplification. The amplified PCR products of 180 bp were digested with the addition of 2 U HhaI (New England Biolabs), 10 mmol/l Tris-HCl pH 7.9, 50 mmol/l NaCl, 10 mmol/l MgCl2 and 1 mmol/l dithiothreitol. After incubation at 37°C for two hours, digested samples were separated on 10% ethidium bromide-stained polyacrylamide gel electrophoresis and visualized by a UVP BIOLMAGING gel doc system. PCR products having an intact HhaI site were cleaved into 99- and 81-bp fragments; the Ala54Thr substitution abolished the restriction site (Figure 2).

Polyacrylamide gel picture showing digested PCR products for FABP2 gene polymorphism. L1, 2, 3, 5: AT genotype, L6: TT genotype, L4: 100 bp ladder and L7: undigested PCR product of FABP2 (180 bp). PCR: polymerase chain reaction; FABP2: fatty acid binding protein 2.
Statistical analysis
All the figures are presented as means ± SD. The genotyping data were compared between cases and controls using the Chi square test. Biochemical parameters were compared using the Student’s t test. The Kruskal Wallis test was used to check the genetic association with biochemical parameters. The correlations between the biochemical parameters were estimated by Karl Pearson’s coefficient of correlation. All statistical tests were performed using SPSS (Statistical Package for the Social Sciences) version 12 software.
Results
Our study includes 190 T2DM cases (129 males and 61 females) and 110 controls (60 males and 50 females). The mean age of cases in this study was 41.29 ± 11.39 years, while in the control group 40 ± 10 years. The age of onset (years) in T2DM cases was 44 ± 11 years. Clinical and biochemical parameters of cases and controls are shown in Table 1. The mean BMI, blood pressure, RBG, FBG, HbA1C, total cholesterol (s. chol.), high-density lipoprotein cholesterol (HDL-C), very low-density lipoprotein cholesterol (VLDL-C), TG and s. creat. levels in the diabetic patients were significantly higher than the control subjects (p < 0.001). We have found significant correlation of RBS with HbA1C, s. chol. and TG (p < 0.001, p = 0.007, p = 0.049), s. creat with HbA1C, TG and VLDL (p = 0.002, p < 0.001, p < 0.001), s. chol. with TG and HDL (p = 0.001, p < 0.001), VLDL with HDL and TG (p = 0.019, p < 0.001). The frequencies of the ACE D/D, I/D and I/I genotypes in T2DM cases and controls were 16.09%, 55.17%, 28.73% and 28.40%, 57.95%,13.63%, respectively (p = 0.378, 0.623, 0.003; X2 = 0.78, 0.24, 9.13; power = 0.816, 0.759, 0.999). The frequency of the ACE I and D allele in T2DM cases and controls were 56.32%, 43.68% and 42.61%, 57.39% (p = 0.001, 0.001; X2 = 10.30, 10.30; power = 0.999, 0.999). The frequencies of FABP2 Ala54Ala, Ala54Thr and Thr54Thr genotypes in T2DM cases and controls were 18.39%, 66.66%, 14.94% and 22.72%, 61.36%, 15.90%, respectively (p = 0.369, 0.379, 0.867, X2 = 0.81, 0.77, 0.03; power = 0.82, 0.817, 0.874). The frequency of Ala54 and Thr54 allele in T2DM cases were 51.72% and 48.28% as compared to 53.40% and 46.60% in the controls (p = 0.752, 0.752; X2= 0.10, 0.10; power = 0.796, 0.796). The genotype and allele frequencies of ACE and FABP2 and statistical analysis among the cases and controls are also shown in Table 2.
Clinical and biochemical parameters of T2DM cases and control subjects.

For finding p values, student’s unpaired t test has been applied except in case of gender comparison, where Chi square test has been applied. T2DM: type 2 diabetes mellitus; M: male; F: female; BMI: body mass index; RBG: random blood glucose; FBG: fasting blood glucose; BP: blood pressure; HbA1C: hemoglobin A1C; TG: triglyceride; HDL: high-density lipoprotein; LDL: low-density lipoprotein; VLDL: very-low density lipoprotein.
The genotype and allele frequencies of ACE (rs4646994) and FABP2 (rs1799883) genes and their statistical analysis among the cases and controls.
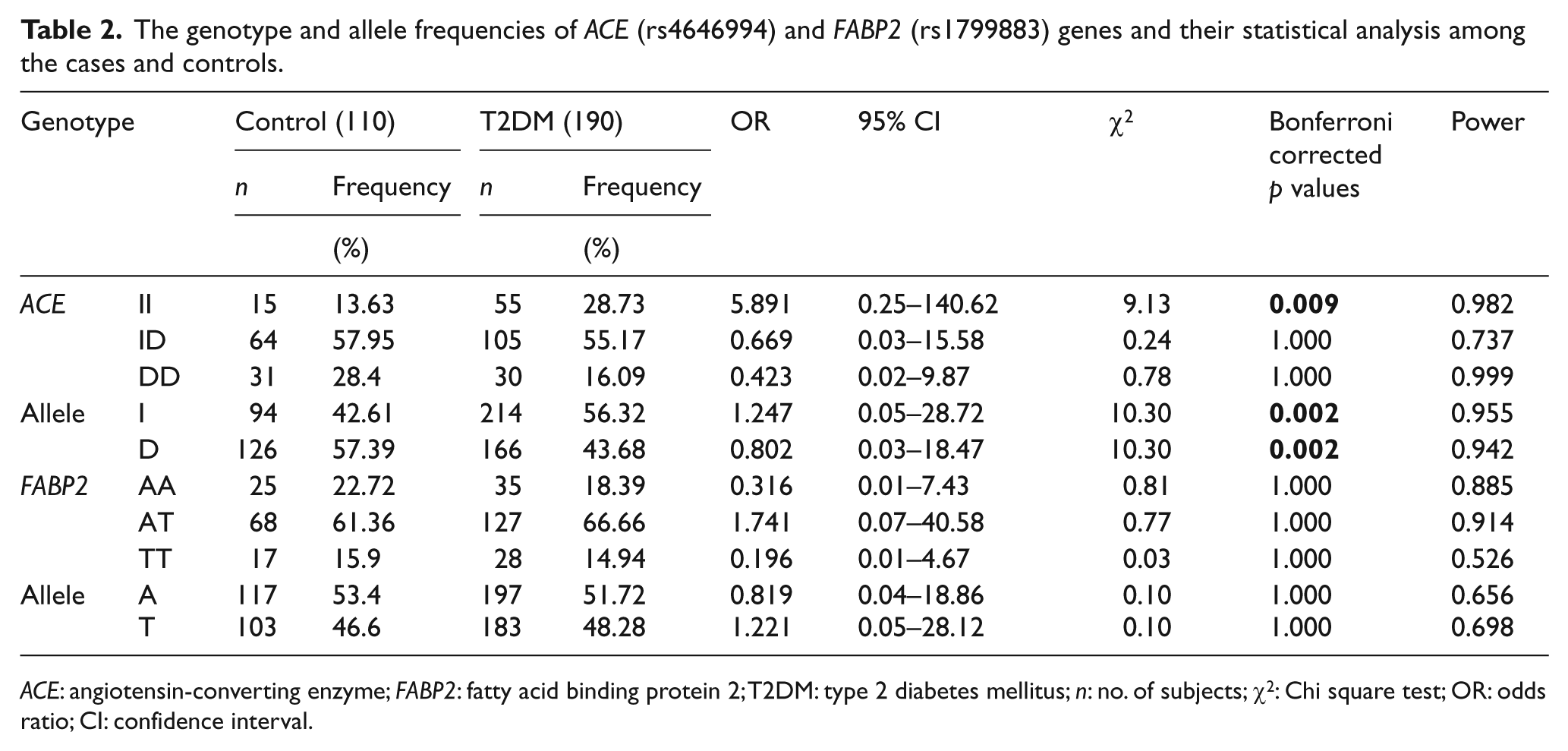
ACE: angiotensin-converting enzyme; FABP2: fatty acid binding protein 2; T2DM: type 2 diabetes mellitus; n: no. of subjects; χ2: Chi square test; OR: odds ratio; CI: confidence interval.
Discussion
ACE polymorphism
The frequency of ACE gene polymorphism is quite variable in different geographic and ethnic groups, and it is also used as a marker in population structure analysis (Table 3). Bonnet (2008) reported in healthy subjects that the D allele conferred an increased risk of having glucose tolerance by decreasing insulin sensitivity. 24 On the other hand, D allele was associated with a reduction in insulin secretion.24,25 Allelic frequency of ACE I and D in Japanese cases with T2DM 26 were 57.14% and 42.85%, which is similar to our data, where the frequency of ACE I allele is 56.32% and D is 43.68%. A positive association between the D allele (I/D and D/D genotype) of ACE polymorphism and diabetic nephropathy was found in patients with T2DM in South India.11,27 ACE D/D genotype frequency in our study was 16.09%, which is comparable to the 18.15% ACE D/D frequency reported in Taiwanese cases with T2DM. 28 A significant relationship was observed between the D/D genotype of ACE polymorphism and diabetic nephropathy 29 in Iranians. The frequency of the D allele is considerably lower, 27.9%, in Malaysians, compared to Caucasians30,31 (56.73%) and North Indians (43.68%, our study). The frequency of I allele is 72.1% in Malaysian 30 patients with T2DM, which is higher in comparison with our data, where I allele is 56.32%. The observed I/I genotype frequency in our study was 28.73% in T2DM cases, which is higher in comparison with Caucasian 10.6%, UK 17.77%, Turkish 18.88% and Australian patients 20.96%.31–34 In our study ACE D/D genotype frequency was 16.09% in T2DM cases, which is lower than the Caucasians, having 43.26% of ACE D/D genotype in T2DM cases.
ACE (rs4646994) and FABP2 (rs1799883) genes polymorphism in different ethnic groups.

ACE: angiotensin-converting enzyme; FABP2: fatty acid binding protein 2; I: insertion; D: deletion; T2DM: type 2 diabetes mellitus; n: significant.
Lee and Tsai (2002) reported a strong association of the I/I genotype with insulin resistance in T2DM patients. 35 Our data also showed a stronger association of the I/I genotype in T2DM patients. On analyzing the ACE gene polymorphisms in cases and controls, the I/I genotype was significantly more frequent in cases as compared to controls (p <0.05) (Table 2).
FABP2 polymorphism
The FABP2 gene has been proposed as a candidate gene for diabetes and insulin resistance because the protein it encodes is involved in fatty acid absorption and metabolism. 18 Numerous studies have assessed FABP2 gene variants and their association with insulin resistance and T2DM. The most studied variant is the Ala54Thr variation at codon 54, a missense variant that has a definite effect on the primary structure of the protein and affects its fatty acid binding properties. Previous studies have found a significant association between the FABP2 genotype and occurrence of T2DM or decreased insulin sensitivity. 14 Several studies have reported associations between this polymorphism and insulin resistance, BMI, dyslipidemia, stroke, metabolic syndromes and hypertriglyceridemia.14,16,18,36 Our study revealed higher levels of serum TGs and higher BMI in Thr54 homozygotes in agreement with the earlier studies of Carlsson et al., 16 who demonstrated similar elevations of TG levels in the Thr54 homozygotes. Vimaleswaran (2006) reported that the Ala54Thr variant was extensively associated with hypertriglyceridemia. 36 Previous studies have failed to establish ascertainable associations between the FABP2 gene and T2DM in Asian Indians. 11 The frequency of FABP2 Ala54Thr polymorphism described in other populations fluctuates between 37% and 45% (Table 3) as in T2DM cases in the United States (36.93%), Sweden (41.9%), Japan (40.62%), Britain (44.77%), Korea (41.66%) and India (42.04%).16,17,23,36–38 The frequency of the Thr54Thr genotype in our study was 14.94%, which is similar to the frequency of the Thr54Thr genotype that is 15.62% in Japanese and 13.54% in Korean23,38 populations. The frequency of the Ala54Ala genotype in our study was 18.39%, which is lower than 50.74% in British and 56.4% in Swedish T2DM cases.16,37 Significant differences were not observed in the genotypic and allele frequencies between the T2DM cases and controls in our study.
Conclusions
In this case-control study, it appears that the ACE I/I genotype frequency was significantly higher in the T2DM cases as compared to the controls, while the FABP2 gene polymorphism shows no significant difference in genotypes and allele frequencies found in the cases and controls. It might be recommended that the ACE gene I/D polymorphisms might be a good marker for the early identification of populations at risk of T2DM. Further study with larger groups may be required to validate the study.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by an intramural grant from the Era’s Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India (Grant no. ELMC/E-1/2010/3942).